REFERRAL GUIDELINE Congenital Muscular Torticollis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
New Guidelines Review Evidence on PT, Helmets for Positional Plagiocephaly by Sandi K
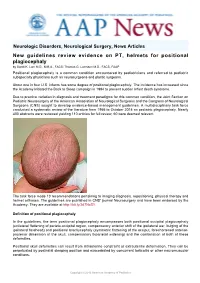
Neurologic Disorders, Neurological Surgery, News Articles New guidelines review evidence on PT, helmets for positional plagiocephaly by Sandi K. Lam M.D., M.B.A., FACS; Thomas G. Luerssen M.D., FACS, FAAP Positional plagiocephaly is a common condition encountered by pediatricians and referred to pediatric subspecialty physicians such as neurosurgeons and plastic surgeons. About one in four U.S. infants has some degree of positional plagiocephaly. The incidence has increased since the Academy initiated the Back to Sleep campaign in 1994 to prevent sudden infant death syndrome. Due to practice variation in diagnosis and treatment paradigms for this common condition, the Joint Section on Pediatric Neurosurgery of the American Association of Neurological Surgeons and the Congress of Neurological Surgeons (CNS) sought to develop evidence-based management guidelines. A multidisciplinary task force conducted a systematic review of the literature from 1966 to October 2014 on pediatric plagiocephaly. Nearly 400 abstracts were reviewed yielding 110 articles for full review; 60 were deemed relevant. The task force made 10 recommendations pertaining to imaging diagnosis, repositioning, physical therapy and helmet orthoses. The guidelines are published in CNS' journal Neurosurgery and have been endorsed by the Academy. They are available at http://bit.ly/2d7NzS1. Definition of positional plagiocephaly In the guidelines, the term positional plagiocephaly encompasses both positional occipital plagiocephaly (unilateral flattening of parieto-occipital region, compensatory anterior shift of the ipsilateral ear, bulging of the ipsilateral forehead) and positional brachycephaly (symmetric flattening of the occiput, foreshortened anterior- posterior dimension of the skull, compensatory biparietal widening) and the combination of both of these deformities. -

West Texas Craniofacial Center of Excellence
TEAM MEMBERS Tammy Camp, M.D. PAID PERMIT #68 LUBBOCK, TX LUBBOCK, U.S. POSTAGE POSTAGE U.S. NONPROFIT ORG Pediatrician, Texas Tech Physicians Desiree Pendergrass, M.D. Pediatrician Dr. Camp Dr. Camp and Dr. Pendergrass will screen infants and children for cardiac, renal, feeding or airway problems often associated with syndromic craniofacial deformities. Alan Eisenbaum, M.D. Pediatric ophthalmologist, Dr. Pendergrass Texas Tech Physicians Curt Cockings, M.D. Pediatric ophthalmologist Dr. Eisenbaum and Dr. Cockings will screen infants and children with abnormal head shapes for any evidence of optic disc swelling of papilledema Dr. Eisenbaum suggestive of elevated intracranial pressure. They will also screen for any visual loss secondary to optic neuropathy, amblyopia or exposure keratopathy as a results of small orbital volume in syndromic synostoses. APPOINTMENTS Dr. Demke sees patients at the Texas Tech Physicians Medical Pavilion in the Surgery Clinic. His clinic days are Tuesday and Thursday, 8 a.m. – 5 p.m. Please call (806)743-2373 for a referral. SURGERY Dr. Nagy sees patients at Covenant Women’s and Children’s Hospital on Tuesdays and Wednesdays 9am – 5pm weekly. For this clinic location, Lubbock, 79430 Texas please call (806) 743-7700 for a referral. He also sees patients at Texas Department Surgery of Tech Physicians Medical Pavilion, 3rd floor, on Mondays from 9am – 5pm 8312 – MS Street 4th 3601 weekly. For this clinic location, please call (806) 743-7335 for a referral. If a patient needs to see both Dr. Demke and Dr. Nagy, arrangements SURGERY will be made to see the patient on the same day. -

Occipital Plagiocephaly: a Critical Review of the Literature
Occipital plagiocephaly: a critical review of the literature Harold L. Rekate, M.D. Pediatric Neurosurgery, Barrow Neurologic Institute, Phoenix, Arizona The objective of this review was to determine what information is available on the incidence, pathophysiology, late complications, and treatment paradigms for occipital plagiocephaly based on a critical review of the literature obtained from recognized databases in peer-reviewed scientific publications. The content of this article is based on a critical review of the literature, and when discussing treatment options, classification of those articles with respect to the strength of the recommendations they contain. Using standard computerized search techniques, databases containing medical literature were queried for key words related to occipital plagiocephaly beginning in 1966. Key words used for this search were: lambdoid, craniosynostosis, cranial sutures, facial asymmetry, torticollis, and plagiocephaly. Titles of all articles were scanned for relevance. Copies of all potentially relevant articles published in the English language were obtained and received at least a cursory review. Several articles not captured by these methods were found to be important when referenced in the articles obtained. Articles discussing treatment were divided into Class I, Class II, and Class III data for the purpose of deciding on their applicability to the development of a potential consensus for the treatment of this controversial condition. Using the aforementioned key words, there were 4308 articles identified with potential relevance: scanning by title excluded all but 89. Of the 89, those with on-line abstracts were scanned, the remainder were obtained via interlibrary loan when needed for scanning of the article itself. The actual incidence of occipital plagiocephaly is unknown and there are no population-based studies of its incidence or prevalence. -

Occipital Plagiocephaly: a Critical Review of the Literature
Occipital plagiocephaly: a critical review of the literature Harold L. Rekate, M.D. Pediatric Neurosurgery, Barrow Neurologic Institute, Phoenix, Arizona The objective of this review was to determine what information is available on the incidence, pathophysiology, late complications, and treatment paradigms for occipital plagiocephaly based on a critical review of the literature obtained from recognized databases in peer-reviewed scientific publications. The content of this article is based on a critical review of the literature, and when discussing treatment options, classification of those articles with respect to the strength of the recommendations they contain. Using standard computerized search techniques, databases containing medical literature were queried for key words related to occipital plagiocephaly beginning in 1966. Key words used for this search were: lambdoid, craniosynostosis, cranial sutures, facial asymmetry, torticollis, and plagiocephaly. Titles of all articles were scanned for relevance. Copies of all potentially relevant articles published in the English language were obtained and received at least a cursory review. Several articles not captured by these methods were found to be important when referenced in the articles obtained. Articles discussing treatment were divided into Class I, Class II, and Class III data for the purpose of deciding on their applicability to the development of a potential consensus for the treatment of this controversial condition. Using the aforementioned key words, there were 4308 articles identified with potential relevance: scanning by title excluded all but 89. Of the 89, those with on-line abstracts were scanned, the remainder were obtained via interlibrary loan when needed for scanning of the article itself. The actual incidence of occipital plagiocephaly is unknown and there are no population-based studies of its incidence or prevalence. -

Identifying the Misshapen Head: Craniosynostosis and Related Disorders Mark S
CLINICAL REPORT Guidance for the Clinician in Rendering Pediatric Care Identifying the Misshapen Head: Craniosynostosis and Related Disorders Mark S. Dias, MD, FAAP, FAANS,a Thomas Samson, MD, FAAP,b Elias B. Rizk, MD, FAAP, FAANS,a Lance S. Governale, MD, FAAP, FAANS,c Joan T. Richtsmeier, PhD,d SECTION ON NEUROLOGIC SURGERY, SECTION ON PLASTIC AND RECONSTRUCTIVE SURGERY Pediatric care providers, pediatricians, pediatric subspecialty physicians, and abstract other health care providers should be able to recognize children with abnormal head shapes that occur as a result of both synostotic and aSection of Pediatric Neurosurgery, Department of Neurosurgery and deformational processes. The purpose of this clinical report is to review the bDivision of Plastic Surgery, Department of Surgery, College of characteristic head shape changes, as well as secondary craniofacial Medicine and dDepartment of Anthropology, College of the Liberal Arts characteristics, that occur in the setting of the various primary and Huck Institutes of the Life Sciences, Pennsylvania State University, State College, Pennsylvania; and cLillian S. Wells Department of craniosynostoses and deformations. As an introduction, the physiology and Neurosurgery, College of Medicine, University of Florida, Gainesville, genetics of skull growth as well as the pathophysiology underlying Florida craniosynostosis are reviewed. This is followed by a description of each type of Clinical reports from the American Academy of Pediatrics benefit from primary craniosynostosis (metopic, unicoronal, bicoronal, sagittal, lambdoid, expertise and resources of liaisons and internal (AAP) and external reviewers. However, clinical reports from the American Academy of and frontosphenoidal) and their resultant head shape changes, with an Pediatrics may not reflect the views of the liaisons or the emphasis on differentiating conditions that require surgical correction from organizations or government agencies that they represent. -

Congenital Scoliosis of the Pediatric Cervical Spine
Congenital Scoliosis of the Pediatric Cervical Spine Brandon Toll, Amer Samdani, Joshua Pahys and Steven Hwang Shriners Hospitals for Children-Philadelphia ICEOS Portugal 2018 Introduction Literature on congenital scoliosis predominantly focuses on thoracic and thoracolumbar curves Papers to date include a handful of 1-2 patients and one series of 18 patients of cervicothoracic hemi vertebra (Chen et al, Spine 2018) Purpose: to better define surgical outcomes of patients having undergone spinal fusions for cervical scoliosis with osseous anomalies Methods Retrospective chart and radiographic review of 17 patients was conducted (2009-2016) from a single center (Shriners Hospitals for Children-Philadelphia) All patients treated surgically for cervical congenital scoliosis with adequate clinical and radiographic data available for analysis Analysis was performed with t-tests (paired and independent samples) and binary correlation Concurrent Findings Cohort Total Number (%) VACTERL Syndrome 2 (11.8) 9 boys/8 girls Tethered Cord 2 (11.8) The most prevalent presentations Sprengel’s Deformity 2 (11.8) were torticollis (29%), and Klippel- Torticollis 5 (29.4) Feil syndrome (17.6%) Klippel-Feil Syndrome 3 (17.6) Pierre Robin Syndrome 1 (5.9) Mean age at surgery was 7.07 ± Brown Syndrome 1 (5.9) 3.38 years Bruck Syndrome 1 (5.9) Average follow-up of 3.06 ± 1.78 Poland’s Syndrome 1 (5.9) years Goldenhar Syndrome 1 (5.9) Larsen Syndrome 2 (11.8) 4 cognitively delayed (23.5%) and 3 non-ambulatory (17.6%) Cognitively Delayed 4 (23.5) Non-ambulatory -

Craniofacial Syndromes: Crouzon, Apert, Pfeiffer, Saethre-Chotzen, and Carpenter Syndromes, Pierre Robin Syndrome, Hemifacial Deformity 10/4/17, 4�06 PM
Craniofacial Syndromes: Crouzon, Apert, Pfeiffer, Saethre-Chotzen, and Carpenter Syndromes, Pierre Robin Syndrome, Hemifacial Deformity 10/4/17, 406 PM Craniofacial Syndromes Updated: Feb 21, 2016 Author: Kongkrit Chaiyasate, MD, FACS; Chief Editor: Jorge I de la Torre, MD, FACS more... Crouzon, Apert, Pfeiffer, Saethre-Chotzen, and Carpenter Syndromes Crouzon Syndrome Crouzon syndrome was first described in 1912. Inheritance Inheritance is autosomal dominant with virtually complete penetrance. It is caused by multiple mutations of the fibroblast growth factor receptor 2 gene, FGFR2. [1, 2, 3] Features Features of the skull are variable. The skull may have associated brachycephaly, trigonocephaly, or oxycephaly. These occur with premature fusion of sagittal, metopic, or coronal sutures, with the coronal sutures being the most common. In addition, combinations of these deformities may be seen. [4] See the image below. http://emedicine.medscape.com/article/1280034-overview PaGe 1 of 61 Craniofacial Syndromes: Crouzon, Apert, Pfeiffer, Saethre-Chotzen, and Carpenter Syndromes, Pierre Robin Syndrome, Hemifacial Deformity 10/4/17, 406 PM Typical appearance of a patient with Crouzon syndrome, with maxillary retrusion, exorbitism, and pseudoprognathism. Anteroposterior view. View Media Gallery The orbits are shallow with resulting exorbitism, which is due to anterior positioning of the greater wing of the sphenoid. The middle cranial fossa is displaced anteriorly and inferiorly, which further shortens the orbit anteroposteriorly. The maxilla is foreshortened, causing reduction of the orbit anteroposteriorly. All these changes result in considerable reduction of orbital volume and resultant significant exorbitism. In severe cases, the lids may not close completely. The maxilla is hypoplastic in all dimensions and is retruded. -
A Guide to Understanding Craniosynostosis
a guide to understanding craniosynostosis a publication of children’s craniofacial association 1 a guide to understanding craniosynostosis his parent’s guide to craniosynostosis is designed to answer tquestions that are frequently asked by parents of a child with craniosynostosis. It is intended to provide a clearer understanding of the condition for patients, parents and others. how can children’s craniofacial association (cca) benefit my family? CA understands that when one family member has a ccraniofacial condition, each person in the family is affected. We provide programs and services designed to address these needs. A detailed list of CCA’s programs and services may be found on our website at www.ccakids.org or call us at 800.535.3643. The information provided here was written by a member of the Medical Advisory Board of the Children’s Craniofacial Association. This booklet is intended for information purposes only. It is not a recommendation for treatment. Decisions for treatment should be based on mutual agreement with the craniofacial team. Possible complications should be discussed with the physician prior to and throughout treatment. Design and Production by Robin Williamson, Williamson Creative Services, Inc., Carrollton, TX. ©2015 Children’s Craniofacial Association, Dallas, TX what is craniosynostosis? raniosynostosis is a medical term that literally means fused cbones of the skull. It is a condition that some children are born with or later develop. The skull is abnormally shaped because of the fusion of skull bones. To better understand craniosynostosis, it is helpful to know that our skulls are not made up of one single “bowl” of bone. -

Craniosynostosis
European Journal of Human Genetics (2011) 19, 369–376 & 2011 Macmillan Publishers Limited All rights reserved 1018-4813/11 www.nature.com/ejhg PRACTICAL GENETICS In association with Craniosynostosis Craniosynostosis, defined as the premature fusion of the cranial sutures, presents many challenges in classification and treatment. At least 20% of cases are caused by specific single gene mutations or chromosome abnormalities. This article maps out approaches to clinical assessment of a child presenting with an unusual head shape, and illustrates how genetic analysis can contribute to diagnosis and management. In brief Apart from the genetic implications, it is important to recog- nise cases with a genetic cause because they are more likely to Craniosynostosis is best managed in a multispecialty tertiary be associated with multiple suture synostosis and extracranial referral unit. complications. Single suture synostosis affects the sagittal suture most com- Genes most commonly mutated in craniosynostosis are monly, followed by the coronal, metopic and lambdoid sutures. FGFR2, FGFR3, TWIST1 and EFNB1. Both environmental factors (especially intrauterine fetal head As well as being associated with syndromes, some clinically constraint) and genes (single gene mutations, chromosome non-syndromic synostosis (usually affecting the coronal abnormalities and polygenic background) predispose to cra- suture) can be caused by single gene mutations, particularly niosynostosis. the Pro250Arg mutation in FGFR3. Most genetically determined craniosynostosis is characterised In severe cases, initial care should be directed towards main- by autosomal dominant inheritance, but around half of cases tenance of the airway, support of feeding, eye protection and are accounted for by new mutations. treatment of raised intracranial pressure. -

Orthoses in Paediatrics: Supporting Development and Therapeutic Intervention in Babies, Children and Young People
Clinical specialties in orthotics and prosthetics Image Courtesy of Orthokids Orthoses in paediatrics: supporting development and therapeutic intervention in babies, children and young people What is an orthosis? Cranial orthoses for babies with An orthosis (pl. orthoses) is an externally applied device that is positional plagiocephaly and designed and fitted to the body. Orthoses (historically known as splints or braces) are described by the body part they brachycephaly encompass. An orthosis may be used to correct body alignment, What is positional plagiocephaly and support function, minimise discomfort or pain, protect a body part after injury or surgery, re-distribute pressure, correct deformity or brachycephaly? assist in rehabilitation. Positional (or deformational) plagiocephaly (pron. play-gee-o-kef- a-lee) and brachycephaly (pron. brak-ee-kef-a-lee) are types of Orthoses in paediatrics – who needs them? cranial deformity – meaning a misshapen head. Plagiocephaly Orthoses play an important role in supporting development occurs when there is flattening on one side of the head, causing and therapeutic intervention across a range of pathologies in asymmetry. Brachycephaly occurs when there is flattening of the the paediatric population – from hip orthoses to encourage hip back of the head. Plagiocephaly and brachycephaly are common development in newborn babies, to spinal orthoses to reduce cranio-facial conditions that occur most often when babies spend abnormal spinal curves in adolescents with scoliosis or kyphosis. prolonged periods lying with their head in the same position. How do cranial orthoses help? Hip orthoses for babies with Cranial orthoses are a developmental dysplasia of the hip (DDH) treatment option for babies What is DDH? with more severe deformity, where counter positioning Developmental dysplasia (or dislocation) of the hip (DDH) is an is not possible or has not abnormal development of the hip joint. -

Shprintzen-Goldberg Syndrome: Case Report Shprintzen-Goldberg Sendromu: Olgu Sunumu Sinem Yalçıntepe1, Özge Özalp Yüreğir1, Sevcan Tuğ Bozdoğan2, Hüseyin Aslan3
Meandros Med Dent J Case Report / Olgu Sunumu Shprintzen-Goldberg Syndrome: Case Report Shprintzen-Goldberg Sendromu: Olgu Sunumu Sinem Yalçıntepe1, Özge Özalp Yüreğir1, Sevcan Tuğ Bozdoğan2, Hüseyin Aslan3 1Adana Numune Training and Research Hospital, Genetic Diagnosis Center, Adana, Turkey 2Mersin University Faculty of Medicine, Department of Medical Genetics, Mersin, Turkey 3Eskişehir Osmangazi University Faculty of Medicine, Department of Medical Genetics, Eskişehir, Turkey Abstract Shprintzen-Goldberg syndrome is a rare syndrome with craniosynostosis of coronal, sagittal or lambdoidal sutures, dolichocephaly, typical craniofacial features, skeletal abnormalities, scoliosis, joint hyperextensibility or contractures, neurological findings and brain malformations. Fifteen months old male patient with hydrocephalus and dysmorphic facial appearance was referred to our clinic for genetical evaluation. In his dysmorphic examination, the findings were dolichocephaly, prominent forehead and glabella, hypertelorism, prominent eyes, proptosis, depressed nasal root, anteverted nostrils, small nose, low-set and posteriorly rotated, dysplastic ears, microretrognathia, short philtrum, fish mouth of mouth, plump cheeks, high and narrow palate, secondary alveolar arch, pectus carinatum. Hands were small and he had arachnodactyly. Toes were thin. He had also hypotonia and umbilical hernia. With these findings, he was clinically diagnosed Keywords as Shprintzen-Goldberg syndrome. This is the first reported case of Shprintzen- Shprintzen-Goldberg syndrome, Goldberg syndrome from Turkey according to literature review. dolichocephaly, craniosynostosis AnahtarKelimeler Shprintzen-Goldberg sendromu, dolikosefali, Öz Shprintzen-Goldberg sendromu koronal, sagital ya da lambdoid sütürlerin kraniosinostoz kraniyosinostozu, dolikosefali, tipik kraniofasiyal özellikler, iskelet anomalileri, skolyoz, eklem hiperekstansibilitesi veya kontraktürleri, nörolojik anomaliler Received/GelişTarihi : 01.04.2015 ve beyin anomalileri ile karakterize nadir görülen bir sendromdur. -

Paediatric Orthopedics : When Does Physiology Become Pathology?
Paediatric Orthopedics : When does Physiology become Pathology? A/Prof Arjandas Mahadev Head and Senior Consultant Department of Orthopaedic Surgery KK Women’s and Children’s Hospital SINGAPORE SCOPE FLATFEET When to Worry? LOWER LIMB MALALIGNMENT INTOEING ACHES AND PAINS ABNORMAL GAIT/LIMPING CHILD FLATFEET FLATFEET Two diagnostic groups Physiological • Dynamic – Due to generalised ligamentous laxity – Due to tight TA • Fixed Flatfeet – Neuromuscular e.g. CP – Idiopathic – Tarsal coalition with/without peroneal spasm Pathological FLATFEET Dynamic FLATFEET Management Dynamic with no tight TA • Watch and Masterly Inactivity Dynamic with tight TA • Stretching and Medial Arch Support Fixed • Treat underlying problem - usually needs surgery. Good Shoeing • Heel in line with back of leg – Firm heel counter • Arch lifted off and not bearing weight – Built in soft arch supports • No pressure on weight bearing area – Good padding of the sole with good flexibility Arch Supports • Most effectively used when the heel is aligned in a good pair of shoes • DOES NOT create an arch- only supports it and arch will collapse again once removed • No need for custom made ones as child is still growing. Arch Supports Heel Cord Stretching FLATFEET When to Worry ? THE VALGUS FOOT Biomechanics FLATFEET TARSAL COALITION Calcaneo Navicular • Dynamic 9 to 12 years – Due to generalised ligamentous laxity oblique xray – Due to tight TA Talo - calcaneum • Fixed Flatfeet 12 to 15 years – Due to pathological ligament laxity. CT – Due to pathological tight muscles 50% bilateral /contracture – Talar anatomy Treat if < 30% involved- treat with soft tissue interposition • oblique talus - fat • Vertical talus - ext digitorum brevis – Tarsal coalition with/without peroneal spasm Spasmodic peroneal flatfoot.