PURE TONE AUDIOMETRY Maggi Soer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

CASE REPORT Resolution of Delayed Sudden Sensorineural Hearing Loss After Stapedectomy
The Mediterranean Journal of Otology CASE REPORT Resolution of Delayed Sudden Sensorineural Hearing Loss After Stapedectomy: A Case Report and Review of the Literature Noam Yehudai, MD, Michal Luntz, MD From the Department of Significant sensorineural hearing loss may develop immediately after suc- Otolaryngology, Head and Neck cessful stapedectomy but sometimes occurs months or even years later. Surgery, Bnai-Zion Medical The rate of recovery from that disorder has not been determined. Several Center, Technion-Israel School of Technology, Haifa, Israel reports in the 1960s described patients with delayed sensorineural hear- ing loss, but that entity has not been mentioned in the English-language Correspondence literature for the last 30 years. We present a review of the literature on this Michal Luntz, MD postsurgical auditory complication and describe a patient with delayed Department of Otolaryngology, Head and Neck Surgery poststapedectomy sensorineural hearing loss that developed 15 months Bnai-Zion Medical Center, after surgery and resolved completely after treatment with an oral steroid. Technion-Israel School of Technology 47 Golomb St, PO Box 4940, Haifa 31048, Israel Phone: 972-4-8359544 Fax: 972-4-8361069 E-mail: [email protected] Submitted: 05 February, 2006 Revised: 07 May, 2006 Accepted: 09 May, 2006 Mediterr J Otol 2006; 3: 156-160 Copyright 2005 © The Mediterranean Society of Otology and Audiology 156 Resolution of Delayed Sudden Sensorineural Hearing Loss After Stapedectomy: A Case Report and Review of the Literature -

OMS II Medical Skills Competencies
SOMA OMS II Medical Skills Competencies Exam Checklist #1 Performed Performed Did not satisfactorily less than perform General, Vital Signs, Skin, Hair, and Nails (1 point) satisfactorily (0 point) (0.5 point) GENERAL 1. Introduces self to patient including full name and status (2nd year osteopathic medical student). 2. Demonstrates respect in addressing patient. 3. Washes hands before shaking hands. 4. Washes hands before beginning physical exam. VITAL SIGNS 5. Takes radial pulse rate. 6. Palpates radial pulse bilaterally. 7. Takes respiratory rate. 8. Takes BP, patient seated comfortably, feet on floor, cuff at heart level and arm supported. 9. Explains vital sign results to patient. SKIN 10. Inspects entire skin surface, explaining reason for inspection to patient 11. Demonstrates proper draping to preserve patient modesty. 12. Palpates skin for turgor, texture, and capillary refill. HAIR 13. Notes observed hair distribution on scalp and body. When possible and appropriate, includes pelvic hair distribution. 14. Describes scalp hair color, distribution and character (thick, thin, straight, curly). NAILS 15. Describes nail abnormalities- color, shape, texture, thickness (lines, brittleness, thickening, discoloration, pitting, ridges, spooning) Score ___/15 Student Name: ________________________________ Student Name: _____________________ Community Campus: ________________________________ Signature of Preceptor: _________________________ Name of Preceptor:_______________________ Date of Completion: ______________ Form Updated 7/10/15 SOMA OMS II Medical Skills Competencies Physical Exam Checklist #2: Performed Performed less Did not perform Head, Eyes, CN’s II-XII satisfactorily than (0 point) (1 point) satisfactorily (0.5 point) EYES 1. Visual Acuity (CN II.) 2. Visual Fields to confrontation 3. Extraocular Movements: (CNs - III, IV, VI.) 4. -

HEENT EXAMINIATION ______HEENT Exam Exam Overview
HEENT EXAMINIATION ____________________________________________________________ HEENT Exam Exam Overview I. Head A. Visual inspection B. Palpation of scalp II. Eyes A. Visual Acuity B. Visual Fields C. Extraocular Movements/Near Response D. Inspection of sclera & conjunctiva E. Pupils F. Ophthalmoscopy III. Ears A. External Inspection B. Otoscopy C. Hearing Acuity D. Weber/Rinne IV. Nose A. External Inspection B. Speculum/otoscope C. Sinus areas V. Throat/Mouth A. Mouth Examination B. Pharynx Examination C. Bimanual Palpation VI. Neck A. Lymph nodes B. Thyroid gland 29 HEENT EXAMINIATION ____________________________________________________________ HEENT Terms Acuity – (ehk-yu-eh-tee) sharpness, clearness, and distinctness of perception or vision. Accommodation - adjustment, especially of the eye for seeing objects at various distances. Miosis – (mi-o-siss) constriction of the pupil of the eye, resulting from a normal response to an increase in light or caused by certain drugs or pathological conditions. Conjunctiva – (kon-junk-ti-veh) the mucous membrane lining the inner surfaces of the eyelids and anterior part of the sclera. Sclera – (sklehr-eh) the tough fibrous tunic forming the outer envelope of the eye and covering all of the eyeball except the cornea. Cornea – (kor-nee-eh) clear, bowl-shaped structure at the front of the eye. It is located in front of the colored part of the eye (iris). The cornea lets light into the eye and partially focuses it. Glaucoma – (glaw-ko-ma) any of a group of eye diseases characterized by abnormally high intraocular fluid pressure, damaged optic disk, hardening of the eyeball, and partial to complete loss of vision. Conductive hearing loss - a hearing impairment of the outer or middle ear, which is due to abnormalities or damage within the conductive pathways leading to the inner ear. -

An Evaluation of Two Pulse-Type Tests Oe Hearing
AN EVALUATION OF TWO PULSE-TYPE TESTS OE HEARING Dissertation Presented in Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the Graduate School of The Ohio State University By THOMAS BROWN ANDERSON, B.S., M. S. The Ohio State University 1952 Approved by: TABLE OE CONTENTS CHAPTER I. INTRODUCTION .... ............. 1 The Problem...................... 7 The Hypotheses ................. 8 Explanation of Terms . ........ 12 II. REVIEW OE LITERATURE ............. 14 III. PROCEDURES........................ 26 Apparatus........................ 26 Stimuli................... .. 28 Subjects ........................ 29 Presentation ................... 30 Scoring of Tests ............... 33 IV. RESULTS AND DISCUSSION........... 34 Part I .......................... 34 Part II ........................ 96 V. CONCLUSIONS ...................... 99 BIBLIOGRAPHY............................ 104 APPENDIX A ............................... 108 APPENDIX B ............................... 110 APPENDIX C............................... 111 APPENDIX D . ............................ 112 APPENDIX E ............................... 113 APPENDIX E ............................... 114 AUTOBIOGRAPHY .......................... 115 ii E09365 LIST OE TABLES TABLE PAGE I. Order of Tests for Each. Group of 10 Subjects . 27 II. Analyses Made and Statistical Methods Used . 36 III. Summary of Tests of Independence and Correla tion of Pure-Tone Scores and Speech- Reception Scores ...................... 38 IV. Summary of Eight Analyses of Variance: Measures -
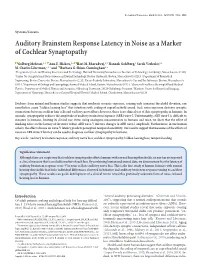
Auditory Brainstem Response Latency in Noise As a Marker of Cochlear Synaptopathy
The Journal of Neuroscience, March 30, 2016 • 36(13):3755–3764 • 3755 Systems/Circuits Auditory Brainstem Response Latency in Noise as a Marker of Cochlear Synaptopathy X Golbarg Mehraei,1,2 XAnn E. Hickox,1,4 X Hari M. Bharadwaj,2,7 Hannah Goldberg,1 Sarah Verhulst,2,6 M. Charles Liberman,1,4,5 and XBarbara G. Shinn-Cunningham2,3 1Program in Speech and Hearing Bioscience and Technology, Harvard University/Massachusetts Institute of Technology, Cambridge, Massachusetts 02139, 2Center for Computational Neuroscience and Neural Technology, Boston University, Boston, Massachusetts 02215, 3Department of Biomedical Engineering, Boston University, Boston, Massachusetts 02215, 4Eaton-Peabody Laboratory, Massachusetts Eye and Ear Infirmary, Boston, Massachusetts 02114, 5Department of Otology and Laryngology, Harvard Medical School, Boston, Massachusetts 02114, 6Cluster of Excellence Hearing4All and Medical Physics, Department of Medical Physics and Acoustics, Oldenburg University, 26129 Oldenburg, Germany, 7Martinos Center for Biomedical Imaging, Department of Neurology, Massachusetts General Hospital/Harvard Medical School, Charlestown, Massachusetts 02129 Evidence from animal and human studies suggests that moderate acoustic exposure, causing only transient threshold elevation, can nonetheless cause “hidden hearing loss” that interferes with coding of suprathreshold sound. Such noise exposure destroys synaptic connections between cochlear hair cells and auditory nerve fibers; however, there is no clinical test of this synaptopathy in humans. In animals, synaptopathy reduces the amplitude of auditory brainstem response (ABR) wave-I. Unfortunately, ABR wave-I is difficult to measure in humans, limiting its clinical use. Here, using analogous measurements in humans and mice, we show that the effect of masking noise on the latency of the more robust ABR wave-V mirrors changes in ABR wave-I amplitude. -

Hearing Loss Due to Myringotomy and Tube Placement and the Role of Preoperative Audiograms
ORIGINAL ARTICLE Hearing Loss Due to Myringotomy and Tube Placement and the Role of Preoperative Audiograms Mark Emery, MD; Peter C. Weber, MD Background: Postoperative complications of myrin- erative and postoperative sensorineural and conductive gotomy and tube placement often include otorrhea, tym- hearing loss. panosclerosis, and tympanic membrane perforation. How- ever, the incidence of sensorineural or conductive hearing Results: No patient developed a postoperative sensori- loss has not been documented. Recent efforts to curb the neural or conductive hearing loss. All patients resolved use of preoperative audiometric testing requires docu- their conductive hearing loss after myringotomy and tube mentation of this incidence. placement. There was a 1.3% incidence of preexisting sen- sorineural hearing loss. Objective: To define the incidence of conductive and sensorineural hearing loss associated with myrin- Conclusions: The incidence of sensorineural or con- gotomy and tube placement. ductive hearing loss after myringotomy and tube place- ment is negligible and the use of preoperative audiomet- Materials and Methods: A retrospective chart re- ric evaluation may be unnecessary in selected patients, view of 550 patients undergoing myringotomy and tube but further studies need to be done to corroborate this placement was performed. A total of 520 patients under- small data set. going 602 procedures (1204 ears), including myrin- gotomy and tube placement, were assessed for preop- Arch Otolaryngol Head Neck Surg. 1998;124:421-424 TITIS MEDIA (OM) is one erative hearing status and whether it has of the most frequent dis- either improved or remained stable after eases of childhood, af- MTT. A recent report by Manning et al11 fecting at least 80% of demonstrated a 1% incidence of preop- children prior to school erative sensorineural hearing loss (SNHL) Oentry.1-4 Because of the high incidence of in children undergoing MTT. -

PDF in English
Case Report Article Labyrinthitis Ossificans. Report of One Case and Literature Review Leandro Ricardo Mattiola*, Mark Makowiecky**, Carlos Eduardo Guimarães de Salles**, Marcela Pozzi Cardoso***, Samir Cahali****. * ENT doctor. Post-graduation student in Head and Neck Surgery at HSPE-SP. ** 2nd yr. Resident Doctor in ENT and Head and Neck Surgery at HSPE-SP. *** ENT Doctor. Assistant doctor in the Otology Department at HSPE-SP. **** PhD in Otorhinolaryngology by UNIFESP. Head of ENT and Head and Neck Surgery Department at HSPE-SP. Institution: Hospital do Servidor Público Estadual de São Paulo - FMO. Departamento de Otorrinolaringologia e Cirurgia de Cabeça e Pescoço. São Paulo / SP – Brazil. Address for correspondence: Leandro Ricardo Mattiola – Rua José de Magalhães 600 - Vila Clementino – São Paulo / SP – Brazil - Zip code: 04026-090 – Telephone/ Fax: (+55 11) 5088-8406 - E-mail: [email protected] Article received on May 31st, 2007. Article approved on November 8th, 2007. SUMMARY Introduction: Labyrinthitis ossificans is a pathology characterized by sensorioneural hearing loss; secondary to infectious process, which produces irreversible injury to inner ear. Objective: To report a labyrinthitis ossificans case and review the literature. Case Report: A seven-year-old male patient, with profound hearing loss in tonal audiometry; no response from brainstem audiometry and compatible CT findings. Conclusion: Labyrinthitis ossificans results ossification on the inner ear structures. Pacient presents profound irreversible hearing loss, followed or not by disequilibrium, that can have important implication on educational socio-development. Diagnosis is important for cochlear implantation cases of the selected cases. Key words: labirinthitis, cochlea, hearing loss, osteogenesis 300 Intl. Arch. Otorhinolaryngol., São Paulo, v.12, n.2, p. -

Correlations Between Audiogram and Objective Hearing Tests in Sensorineural Hearing Loss
International Tinnitus Journal, Vol. 5, No.2, 107-112 (1999) Correlations Between Audiogram and Objective Hearing Tests in Sensorineural Hearing Loss L. Bishara,1 J. Ben-David,l L. Podoshin,1 M. Fradis,l C.B. Teszler,l H. Pratt,2 T. Shpack,3 H. Feiglin,3 H. Hafner,3 and N. Herlinger2 I Department of Otolaryngology, Head and Neck Surgery, and 3Institute of Audiology, Bnai-Zion Medical Center, and 2Evoked Potentials Laboratory, Technion, Haifa, Israel Abstract: Owing to its subjective nature, behavioral pure-tone audiometry often is an unre liable testing method in uncooperative subjects, and assessing the true hearing threshold be comes difficult. In such cases, objective tests are used for hearing-threshold determination (i.e., auditory brainstem evoked potentials [ABEP] and frequency-specific auditory evoked potentials: slow negative response at 10 msec [SN-1O]). The purpose of this study was to evaluate the correlation between pure-tone audiogram shape and the predictive accuracy of SN-IO and ABEP in normal controls and in patients suf fering from sensorineural hearing loss (SNHL). One-hundred-and-fifty subjects aged 15 to 70, some with normal hearing and the remainder with SNHL, were tested prospectively in a double-blind design. The battery of tests included pure-tone audiometry (air and bone conduction), speech reception threshold, ABEP, and SN- 10. Patients with SNHL were divided into four categories according to audiogram shape (i.e., flat, ascending, descending, and all other shapes). The results showed that ABEP predicts behavioral thresholds at 3 kHz and 4 kHz in cases of high-frequency hearing loss. -

CASE REPORT 48-Year-Old Man
THE PATIENT CASE REPORT 48-year-old man SIGNS & SYMPTOMS – Acute hearing loss, tinnitus, and fullness in the left ear Dennerd Ovando, MD; J. Walter Kutz, MD; Weber test lateralized to the – Sergio Huerta, MD right ear Department of Surgery (Drs. Ovando and Huerta) – Positive Rinne test and and Department of normal tympanometry Otolaryngology (Dr. Kutz), UT Southwestern Medical Center, Dallas; VA North Texas Health Care System, Dallas (Dr. Huerta) Sergio.Huerta@ THE CASE UTSouthwestern.edu The authors reported no A healthy 48-year-old man presented to our otolaryngology clinic with a 2-hour history of potential conflict of interest hearing loss, tinnitus, and fullness in the left ear. He denied any vertigo, nausea, vomiting, relevant to this article. otalgia, or otorrhea. He had noticed signs of a possible upper respiratory infection, including a sore throat and headache, the day before his symptoms started. His medical history was unremarkable. He denied any history of otologic surgery, trauma, or vision problems, and he was not taking any medications. The patient was afebrile on physical examination with a heart rate of 48 beats/min and blood pressure of 117/68 mm Hg. A Weber test performed using a 512-Hz tuning fork lateral- ized to the right ear. A Rinne test showed air conduction was louder than bone conduction in the affected left ear—a normal finding. Tympanometry and otoscopic examination showed the bilateral tympanic membranes were normal. THE DIAGNOSIS Pure tone audiometry showed severe sensorineural hearing loss in the left ear and a poor speech discrimination score. The Weber test confirmed the hearing loss was sensorineu- ral and not conductive, ruling out a middle ear effusion. -

Bates' Pocket Guide to Physical Examination and History Taking
Lynn S. Bickley, MD, FACP Clinical Professor of Internal Medicine School of Medicine University of New Mexico Albuquerque, New Mexico Peter G. Szilagyi, MD, MPH Professor of Pediatrics Chief, Division of General Pediatrics University of Rochester School of Medicine and Dentistry Rochester, New York Acquisitions Editor: Elizabeth Nieginski/Susan Rhyner Product Manager: Annette Ferran Editorial Assistant: Ashley Fischer Design Coordinator: Joan Wendt Art Director, Illustration: Brett MacNaughton Manufacturing Coordinator: Karin Duffield Indexer: Angie Allen Prepress Vendor: Aptara, Inc. 7th Edition Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Copyright © 2009 by Wolters Kluwer Health | Lippincott Williams & Wilkins. Copyright © 2007, 2004, 2000 by Lippincott Williams & Wilkins. Copyright © 1995, 1991 by J. B. Lippincott Company. All rights reserved. This book is protected by copyright. No part of this book may be reproduced or transmitted in any form or by any means, including as photocopies or scanned-in or other electronic copies, or utilized by any information storage and retrieval system without written permission from the copyright owner, except for brief quotations embodied in critical articles and reviews. Materials appear- ing in this book prepared by individuals as part of their official duties as U.S. government employees are not covered by the above-mentioned copyright. To request permission, please contact Lippincott Williams & Wilkins at Two Commerce Square, 2001 Market Street, Philadelphia PA 19103, via email at [email protected] or via website at lww.com (products and services). 9 8 7 6 5 4 3 2 1 Printed in China Library of Congress Cataloging-in-Publication Data Bickley, Lynn S. Bates’ pocket guide to physical examination and history taking / Lynn S. -

Hearing Screening Training Manual REVISED 12/2018
Hearing Screening Training Manual REVISED 12/2018 Minnesota Department of Health (MDH) Community and Family Health Division Maternal and Child Health Section 1 2 For more information, contact Minnesota Department of Health Maternal Child Health Section 85 E 7th Place St. Paul, MN 55164-0882 651-201-3760 [email protected] www.health.state.mn.us Upon request, this material will be made available in an alternative format such as large print, Braille or audio recording. 3 Revisions made to this manual are based on: Guidelines for Hearing Screening After the Newborn Period to Kindergarten Age http://www.improveehdi.org/mn/library/files/afternewbornperiodguidelines.pdf American Academy of Audiology, Childhood Screening Guidelines http://www.cdc.gov/ncbddd/hearingloss/documents/AAA_Childhood%20Hearing%2 0Guidelines_2011.pdf American Academy of Pediatrics (AAP), Hearing Assessment in Children: Recommendations Beyond Neonatal Screening http://pediatrics.aappublications.org/content/124/4/1252 4 Contents Introduction .................................................................................................................... 7 Audience ..................................................................................................................... 7 Purpose ....................................................................................................................... 7 Overview of hearing and hearing loss ............................................................................ 9 Sound, hearing, and hearing -
Current Audiometric Tests for the Detection of Functional Hearing Loss
CURRENT AUDIOMETRIC TESTS FOR THE DETECTION OF FUNCTIONAL HEARING LOSS by JOAN PHYLLIS COOPER X^^ Be A., Union College, 1965 A MASTER'S REPORT submitted in partial fulfillment of the J requirements for the degree MASTER OF ARTS Department of Speech KANSAS STATE UNIVERSITY Manhattan, Kansas 1963 Approved by: Ma j or ? ro re s s or . bo 11 C6£ TABLE OF CONTENTS Chapter Page I , Introduction .••••••••••••••••••«••• • • • 1 Definitions ....?................«« •••••••• 2 II. Tests for Functional Hearing Loss 4 General Behavior in the Clinical Evaluation 4 The Ear, Nose, and Throat Examination 9 Pure-tone Audiometry 12 Saucer-shaped Audiograms 14 False-alarm Responses During Pure-tone Audiometry ...................... c 17 Inappropriate Lateralization ,« 17 Bone Conduction Audiometry 20 Speech Audiometry ••••••••••••••••• • 22 Speech Discrimination ••••••••••• 22 Speech Reception Threshold ........ ............... 23 Errors During Measurement of Spondee Threshold ... 2 3 Inappropriate Lateralization 26 Pure-tone Stenger Test 26 Modified (Speech) Stenger Test 29 Doerf ler-Stewart Test 30 Lombard Test ............ o 36 De layed Auditory Feedback ., 39 Psychogalvanic Skin Resistance Test 45 Modification of EDR Test , . .. 50 Bekesy Type V Tracing ......... o ..... ....... ... s ...... 51 c ^ . iii Chapter Page ( II. Rainville Test 5S Sensorineural Acuity Level Test ..... 59 Lipreading Test .....«•..•.<.«•......,....•............ 61 The Variable Intensity Pulse Count Method 62 Rapid Random Loudness Judgments ..................... c 63 Middle Ear