Meta-Analysis of a Multi-Ethnic, Breast Cancer Case-Control Targeted Sequencing Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

4-6 Weeks Old Female C57BL/6 Mice Obtained from Jackson Labs Were Used for Cell Isolation
Methods Mice: 4-6 weeks old female C57BL/6 mice obtained from Jackson labs were used for cell isolation. Female Foxp3-IRES-GFP reporter mice (1), backcrossed to B6/C57 background for 10 generations, were used for the isolation of naïve CD4 and naïve CD8 cells for the RNAseq experiments. The mice were housed in pathogen-free animal facility in the La Jolla Institute for Allergy and Immunology and were used according to protocols approved by the Institutional Animal Care and use Committee. Preparation of cells: Subsets of thymocytes were isolated by cell sorting as previously described (2), after cell surface staining using CD4 (GK1.5), CD8 (53-6.7), CD3ε (145- 2C11), CD24 (M1/69) (all from Biolegend). DP cells: CD4+CD8 int/hi; CD4 SP cells: CD4CD3 hi, CD24 int/lo; CD8 SP cells: CD8 int/hi CD4 CD3 hi, CD24 int/lo (Fig S2). Peripheral subsets were isolated after pooling spleen and lymph nodes. T cells were enriched by negative isolation using Dynabeads (Dynabeads untouched mouse T cells, 11413D, Invitrogen). After surface staining for CD4 (GK1.5), CD8 (53-6.7), CD62L (MEL-14), CD25 (PC61) and CD44 (IM7), naïve CD4+CD62L hiCD25-CD44lo and naïve CD8+CD62L hiCD25-CD44lo were obtained by sorting (BD FACS Aria). Additionally, for the RNAseq experiments, CD4 and CD8 naïve cells were isolated by sorting T cells from the Foxp3- IRES-GFP mice: CD4+CD62LhiCD25–CD44lo GFP(FOXP3)– and CD8+CD62LhiCD25– CD44lo GFP(FOXP3)– (antibodies were from Biolegend). In some cases, naïve CD4 cells were cultured in vitro under Th1 or Th2 polarizing conditions (3, 4). -

Transcriptional Control of Tissue-Resident Memory T Cell Generation
Transcriptional control of tissue-resident memory T cell generation Filip Cvetkovski Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Graduate School of Arts and Sciences COLUMBIA UNIVERSITY 2019 © 2019 Filip Cvetkovski All rights reserved ABSTRACT Transcriptional control of tissue-resident memory T cell generation Filip Cvetkovski Tissue-resident memory T cells (TRM) are a non-circulating subset of memory that are maintained at sites of pathogen entry and mediate optimal protection against reinfection. Lung TRM can be generated in response to respiratory infection or vaccination, however, the molecular pathways involved in CD4+TRM establishment have not been defined. Here, we performed transcriptional profiling of influenza-specific lung CD4+TRM following influenza infection to identify pathways implicated in CD4+TRM generation and homeostasis. Lung CD4+TRM displayed a unique transcriptional profile distinct from spleen memory, including up-regulation of a gene network induced by the transcription factor IRF4, a known regulator of effector T cell differentiation. In addition, the gene expression profile of lung CD4+TRM was enriched in gene sets previously described in tissue-resident regulatory T cells. Up-regulation of immunomodulatory molecules such as CTLA-4, PD-1, and ICOS, suggested a potential regulatory role for CD4+TRM in tissues. Using loss-of-function genetic experiments in mice, we demonstrate that IRF4 is required for the generation of lung-localized pathogen-specific effector CD4+T cells during acute influenza infection. Influenza-specific IRF4−/− T cells failed to fully express CD44, and maintained high levels of CD62L compared to wild type, suggesting a defect in complete differentiation into lung-tropic effector T cells. -

SELP Asp603asn and Severe Thrombosis in COVID-19 Males
Fallerini et al. J Hematol Oncol (2021) 14:123 https://doi.org/10.1186/s13045-021-01136-9 LETTER TO THE EDITOR Open Access SELP Asp603Asn and severe thrombosis in COVID-19 males Chiara Fallerini1,2, Sergio Daga1,2, Elisa Benetti2, Nicola Picchiotti3,4, Kristina Zguro2, Francesca Catapano1,2, Virginia Baroni1,2, Simone Lanini5, Alessandro Bucalossi6, Giuseppe Marotta6, Francesca Colombo7, Margherita Baldassarri1,2, Francesca Fava1,2,8, Giada Beligni1,2, Laura Di Sarno1,2, Diana Alaverdian1,2, Maria Palmieri1,2, Susanna Croci1,2, Andrea M. Isidori9, Simone Furini2, Elisa Frullanti1,2 on behalf of GEN-COVID Multicenter Study, Alessandra Renieri1,2,8* and Francesca Mari1,2,8 Abstract Thromboembolism is a frequent cause of severity and mortality in COVID-19. However, the etiology of this phenom- enon is not well understood. A cohort of 1186 subjects, from the GEN-COVID consortium, infected by SARS-CoV-2 with diferent severity was stratifed by sex and adjusted by age. Then, common coding variants from whole exome sequencing were mined by LASSO logistic regression. The homozygosity of the cell adhesion molecule P-selectin gene (SELP) rs6127 (c.1807G > A; p.Asp603Asn) which has been already associated with thrombotic risk is found to be associated with severity in the male subcohort of 513 subjects (odds ratio 2.27, 95% Confdence Interval 1.54–3.36). As the SELP gene is downregulated by testosterone, the odd ratio is increased= in males older than 50 (OR 2.42, 95% CI 1.53–3.82). Asn/Asn homozygotes have increased D-dimers values especially when associated with poly Q 23 in the androgen receptor (OR 3.26, 95% CI 1.41–7.52). -

Engineered Type 1 Regulatory T Cells Designed for Clinical Use Kill Primary
ARTICLE Acute Myeloid Leukemia Engineered type 1 regulatory T cells designed Ferrata Storti Foundation for clinical use kill primary pediatric acute myeloid leukemia cells Brandon Cieniewicz,1* Molly Javier Uyeda,1,2* Ping (Pauline) Chen,1 Ece Canan Sayitoglu,1 Jeffrey Mao-Hwa Liu,1 Grazia Andolfi,3 Katharine Greenthal,1 Alice Bertaina,1,4 Silvia Gregori,3 Rosa Bacchetta,1,4 Norman James Lacayo,1 Alma-Martina Cepika1,4# and Maria Grazia Roncarolo1,2,4# Haematologica 2021 Volume 106(10):2588-2597 1Department of Pediatrics, Division of Stem Cell Transplantation and Regenerative Medicine, Stanford School of Medicine, Stanford, CA, USA; 2Stanford Institute for Stem Cell Biology and Regenerative Medicine, Stanford School of Medicine, Stanford, CA, USA; 3San Raffaele Telethon Institute for Gene Therapy, Milan, Italy and 4Center for Definitive and Curative Medicine, Stanford School of Medicine, Stanford, CA, USA *BC and MJU contributed equally as co-first authors #AMC and MGR contributed equally as co-senior authors ABSTRACT ype 1 regulatory (Tr1) T cells induced by enforced expression of interleukin-10 (LV-10) are being developed as a novel treatment for Tchemotherapy-resistant myeloid leukemias. In vivo, LV-10 cells do not cause graft-versus-host disease while mediating graft-versus-leukemia effect against adult acute myeloid leukemia (AML). Since pediatric AML (pAML) and adult AML are different on a genetic and epigenetic level, we investigate herein whether LV-10 cells also efficiently kill pAML cells. We show that the majority of primary pAML are killed by LV-10 cells, with different levels of sensitivity to killing. Transcriptionally, pAML sensitive to LV-10 killing expressed a myeloid maturation signature. -

Forms of Supplemental Selenium in Vitamin-Mineral
University of Kentucky UKnowledge Theses and Dissertations--Animal and Food Sciences Animal and Food Sciences 2019 FORMS OF SUPPLEMENTAL SELENIUM IN VITAMIN-MINERAL MIXES DIFFERENTIALLY AFFECT SEROLOGICAL AND HEPATIC PARAMETERS OF GROWING BEEF STEERS GRAZING ENDOPHYTE-INFECTED TALL FESCUE Yang Jia University of Kentucky, [email protected] Digital Object Identifier: https://doi.org/10.13023/etd.2019.028 Right click to open a feedback form in a new tab to let us know how this document benefits ou.y Recommended Citation Jia, Yang, "FORMS OF SUPPLEMENTAL SELENIUM IN VITAMIN-MINERAL MIXES DIFFERENTIALLY AFFECT SEROLOGICAL AND HEPATIC PARAMETERS OF GROWING BEEF STEERS GRAZING ENDOPHYTE- INFECTED TALL FESCUE" (2019). Theses and Dissertations--Animal and Food Sciences. 97. https://uknowledge.uky.edu/animalsci_etds/97 This Doctoral Dissertation is brought to you for free and open access by the Animal and Food Sciences at UKnowledge. It has been accepted for inclusion in Theses and Dissertations--Animal and Food Sciences by an authorized administrator of UKnowledge. For more information, please contact [email protected]. STUDENT AGREEMENT: I represent that my thesis or dissertation and abstract are my original work. Proper attribution has been given to all outside sources. I understand that I am solely responsible for obtaining any needed copyright permissions. I have obtained needed written permission statement(s) from the owner(s) of each third-party copyrighted matter to be included in my work, allowing electronic distribution (if such use is not permitted by the fair use doctrine) which will be submitted to UKnowledge as Additional File. I hereby grant to The University of Kentucky and its agents the irrevocable, non-exclusive, and royalty-free license to archive and make accessible my work in whole or in part in all forms of media, now or hereafter known. -
Normalized Expression Values *
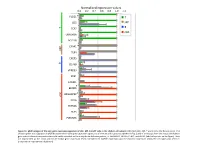
Normalized expression values 0.0 0.2 0.4 0.6 0.8 1.0 1.2 PLCG1 * T CD5 MP T B TCF7 cDC UBASH3A BCL11B C5AR1 * MP TLR4 CXCR5 B CD79B VPREB3 XCR1 CADM1 BEND5 * ARGHAP22 * cDC CIITA ZBTB46 FLT3 PLEKHA5 Figure S1. qPCR analysis of the core gene expression signature of cDC, MP, B and T cells in the chicken cell suBsets. RNA from cDC, MP, T and B cells of 2 disUnct pools of 4 chicken spleen was subjected to qPCR detecUon of the core gene expression signatures of immune cell subsets established in Fig. 3 and of transcripts from the mouse and human gene subset selected compendia that could not be detected on the array due to defecUve probes, i.e. ARGHAP22, BEND5, C5AR1, and PLCG1 (labeled by a star on the figure). Data are represented as the mean and SD of relave gene expression levels normalized to GAPDH expression and the maximal expression across the cell types was set to 1 (independent experimental duplicates). B cell T cell cDC Monocyte/MP Chicken Human Mouse Figure S2. Unsupervised hierarchical clustering of orthologous immune response genes across chicken, human and mouse reveals globally conserved clusters of lymphoïd- specific and myeloïd- specific genes. Heatmap of cross-normalized expression profiles for immune response genes present on all three species arrays and regulated at least 2 folds across all cell suBsets, including chicken B cells (c_B), T cells (c_CD3), MP (c_MP) and cDC (c_cDC), human B cells (h_B), T cells (h_CD4_T and h_CD8_T), monocyte-derived MP (h_MoMP), peripheral blood mononucleated cell-derived MP (h_PBMC_MP), non-classical monocytes (h_non- classical_MO), classical monocytes (h_classical_MO), BDCA3+ cDC (h_BDCA3), BDCA1+ cDC (h_BDCA1), murine B cells (m_B), T cells (m_CD4_T and m_CD8_T), peritoneal cavity MP (m_PC_MPII-480HI), lung MP (m_LU_MP), non-classical monocytes (m_non-classical_MO), classical monocytes (m_classical_MO), splenic CD8α+ cDC (m_SP_DC1), suBcutaneous lymph node CD8α+ cDC (m_LN_DC1), splenic CD11B+ cDC (m_SP_DC2), suBcutaneous lymph node CD11B+ cDC (m_LN_DC2). -

Lncrna and Mrna Expression Profile of Peripheral Blood Mononuclear
www.nature.com/scientificreports OPEN LncRNA and mRNA expression profle of peripheral blood mononuclear cells in primary Sjögren’s syndrome patients Yu Peng1,2,4, Xuan Luo1,2,4, Yingying Chen1,2, Linyi Peng1,2, Chuiwen Deng1,2, Yunyun Fei1,2,3*, Wen Zhang1,2,3* & Yan Zhao1,2,3* The aim of this study was to elucidate the expression profle and the potential role of long non- coding RNA (LncRNA) in the peripheral blood mononuclear cells of primary Sjögren’s syndrome (pSS) patients. RNA-seq technology was used to detect the diferentially expressed LncRNAs and mRNAs between fve age-and sex-matched paired pSS patients and healthy control PBMCs. The selected LncRNAs were detected in the validation study by RT-qPCR in 16 paired pSS patients and healthy controls. The GO, KEGG, co-localization, and co-expression analysis were performed to enrich the potential gene functions and pathways. In this study, 44 out of 1772 LncRNAs and 1034 out of 15,424 mRNAs were expressed diferentially in the PBMCs of pSS patients. LINC00426, TPTEP1-202, CYTOR, NRIR, and BISPR were validated as aberrantly expressed, and these LncRNAs strongly correlated with disease activity of pSS. GO and KEGG pathway analysis revealed the signifcant enrichment of biological processes, cellular components, and molecular function of the up and down-regulated mRNAs, which were mainly concentrated in the immune response and immune system processes. Co-localization and co-expression analysis also revealed that diferentially expressed LncRNAs in the PBMCs of pSS were strongly correlated to the mRNA functioning associated with immune response and cell metastasis. -

Lineage-Specific Effector Signatures of Invariant NKT Cells Are Shared Amongst Δγ T, Innate Lymphoid, and Th Cells
Downloaded from http://www.jimmunol.org/ by guest on September 26, 2021 δγ is online at: average * The Journal of Immunology , 10 of which you can access for free at: 2016; 197:1460-1470; Prepublished online 6 July from submission to initial decision 4 weeks from acceptance to publication 2016; doi: 10.4049/jimmunol.1600643 http://www.jimmunol.org/content/197/4/1460 Lineage-Specific Effector Signatures of Invariant NKT Cells Are Shared amongst T, Innate Lymphoid, and Th Cells You Jeong Lee, Gabriel J. Starrett, Seungeun Thera Lee, Rendong Yang, Christine M. Henzler, Stephen C. Jameson and Kristin A. Hogquist J Immunol cites 41 articles Submit online. Every submission reviewed by practicing scientists ? is published twice each month by Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts http://jimmunol.org/subscription http://www.jimmunol.org/content/suppl/2016/07/06/jimmunol.160064 3.DCSupplemental This article http://www.jimmunol.org/content/197/4/1460.full#ref-list-1 Information about subscribing to The JI No Triage! Fast Publication! Rapid Reviews! 30 days* Why • • • Material References Permissions Email Alerts Subscription Supplementary The Journal of Immunology The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2016 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. This information is current as of September 26, 2021. The Journal of Immunology Lineage-Specific Effector Signatures of Invariant NKT Cells Are Shared amongst gd T, Innate Lymphoid, and Th Cells You Jeong Lee,* Gabriel J. -

Table S1. 103 Ferroptosis-Related Genes Retrieved from the Genecards
Table S1. 103 ferroptosis-related genes retrieved from the GeneCards. Gene Symbol Description Category GPX4 Glutathione Peroxidase 4 Protein Coding AIFM2 Apoptosis Inducing Factor Mitochondria Associated 2 Protein Coding TP53 Tumor Protein P53 Protein Coding ACSL4 Acyl-CoA Synthetase Long Chain Family Member 4 Protein Coding SLC7A11 Solute Carrier Family 7 Member 11 Protein Coding VDAC2 Voltage Dependent Anion Channel 2 Protein Coding VDAC3 Voltage Dependent Anion Channel 3 Protein Coding ATG5 Autophagy Related 5 Protein Coding ATG7 Autophagy Related 7 Protein Coding NCOA4 Nuclear Receptor Coactivator 4 Protein Coding HMOX1 Heme Oxygenase 1 Protein Coding SLC3A2 Solute Carrier Family 3 Member 2 Protein Coding ALOX15 Arachidonate 15-Lipoxygenase Protein Coding BECN1 Beclin 1 Protein Coding PRKAA1 Protein Kinase AMP-Activated Catalytic Subunit Alpha 1 Protein Coding SAT1 Spermidine/Spermine N1-Acetyltransferase 1 Protein Coding NF2 Neurofibromin 2 Protein Coding YAP1 Yes1 Associated Transcriptional Regulator Protein Coding FTH1 Ferritin Heavy Chain 1 Protein Coding TF Transferrin Protein Coding TFRC Transferrin Receptor Protein Coding FTL Ferritin Light Chain Protein Coding CYBB Cytochrome B-245 Beta Chain Protein Coding GSS Glutathione Synthetase Protein Coding CP Ceruloplasmin Protein Coding PRNP Prion Protein Protein Coding SLC11A2 Solute Carrier Family 11 Member 2 Protein Coding SLC40A1 Solute Carrier Family 40 Member 1 Protein Coding STEAP3 STEAP3 Metalloreductase Protein Coding ACSL1 Acyl-CoA Synthetase Long Chain Family Member 1 Protein -

Us 2018 / 0305689 A1
US 20180305689A1 ( 19 ) United States (12 ) Patent Application Publication ( 10) Pub . No. : US 2018 /0305689 A1 Sætrom et al. ( 43 ) Pub . Date: Oct. 25 , 2018 ( 54 ) SARNA COMPOSITIONS AND METHODS OF plication No . 62 /150 , 895 , filed on Apr. 22 , 2015 , USE provisional application No . 62/ 150 ,904 , filed on Apr. 22 , 2015 , provisional application No. 62 / 150 , 908 , (71 ) Applicant: MINA THERAPEUTICS LIMITED , filed on Apr. 22 , 2015 , provisional application No. LONDON (GB ) 62 / 150 , 900 , filed on Apr. 22 , 2015 . (72 ) Inventors : Pål Sætrom , Trondheim (NO ) ; Endre Publication Classification Bakken Stovner , Trondheim (NO ) (51 ) Int . CI. C12N 15 / 113 (2006 .01 ) (21 ) Appl. No. : 15 /568 , 046 (52 ) U . S . CI. (22 ) PCT Filed : Apr. 21 , 2016 CPC .. .. .. C12N 15 / 113 ( 2013 .01 ) ; C12N 2310 / 34 ( 2013. 01 ) ; C12N 2310 /14 (2013 . 01 ) ; C12N ( 86 ) PCT No .: PCT/ GB2016 /051116 2310 / 11 (2013 .01 ) $ 371 ( c ) ( 1 ) , ( 2 ) Date : Oct . 20 , 2017 (57 ) ABSTRACT The invention relates to oligonucleotides , e . g . , saRNAS Related U . S . Application Data useful in upregulating the expression of a target gene and (60 ) Provisional application No . 62 / 150 ,892 , filed on Apr. therapeutic compositions comprising such oligonucleotides . 22 , 2015 , provisional application No . 62 / 150 ,893 , Methods of using the oligonucleotides and the therapeutic filed on Apr. 22 , 2015 , provisional application No . compositions are also provided . 62 / 150 ,897 , filed on Apr. 22 , 2015 , provisional ap Specification includes a Sequence Listing . SARNA sense strand (Fessenger 3 ' SARNA antisense strand (Guide ) Mathew, Si Target antisense RNA transcript, e . g . NAT Target Coding strand Gene Transcription start site ( T55 ) TY{ { ? ? Targeted Target transcript , e . -

Supplementary Information
Supplementary information FTO intronic SNP strongly influences human neck adipocyte browning determined by tissue and PPARγ specific regulation: a transcriptome analysis Beáta B. Tóth, Rini Arianti, Abhirup Shaw, Attila Vámos, Zoltán Veréb, Szilárd Póliska, Ferenc Győry, Zsolt Bacso, László Fésüs*, Endre Kristóf* Supplementary Figure 1. A B C Supplementary Figure 1. Functional features of the primary SC and DN adipocytes differentiated for two weeks to white or brown. (A) Basal, cAMP stimulated and oligomycin inhibited oxygen consumption (OC) levels (as compared to basal OCR of SC white adipocytes) n=4. (B) Basal and cAMP-stimulated extracellular acidification levels (as compared to basal ECAR of SC white adipocytes) n=4. (C) The proportion of creatine kinase futile cycle related OC at basal and cAMP-stimulated n=4. SC: Subcutaneous, DN: Deep-neck, W: white differentiation protocol, B: brown differentiation protocol. Statistics: In comparison of two groups two-tailed paired Student’s t-test was used. *p<0.05. In multi-factor comparision we used two- way ANOVA and post hoc Tukey’s test. *p<0.05. **p<0.01. n=4 Supplementary Figure 2. Expression of ProFAT brown markers Z-score by donor -2.7 2.7 Supplementary Figure 2. Expression profile of ProFAT marker genes. Heat map shows the expression profile of browning (44) and white (6) characteristic marker genes from ProFAT database in SC and DN adipose progenitors and differentiated samples. Supplementary Figure 3. UCP1 CPT1B EHHADH AKAP1 SOD2 ACSL5 ZIC1 PRDM16 CKMT1A CKMT1B CIDEA PM20D1 Supplementary Figure 3. Gene-expression of key browning marker genes based on RNAseq data. -

Supplementary Data
Figure S1 A B NCI-Nature pathways : upregulated genes MDA-MB-231 MCF-7 MCF-7 C Casp3 -/- Casp3 +/+ D Casp3 -/- Casp3 +/+ NT DTX NT DTX NT DTX NT DTX NS c-Casp9 25 35 c-Casp3 70 HSC70 70 HSC70 MCF-7 MCF-7 Casp3 -/- Casp3 +/+ Casp3 -/- Casp3 +/+ E NT DTX NT DTX F NT DTX NT DTX c-Casp8 c-Casp7 15 15 70 HSC70 70 HSC70 G Not treated Docetaxel Casp3 -/- Casp3 H MCF-7 7AAD Casp3 +/+ Casp3 Annexin V Figure S1: A. In vivo treatment of MDA-MB-231 tumors with docetaxel induces angiogenic pathways. ClueGEO software was used to analyze angiogenic pathways activation in MDA-MB-231 tumors treated with docetaxel. B. In vivo treatment of MDA-MB-231 tumors with docetaxel induces angiogenic pathways. RNA sequencing analysis of MDA-MB-231 tumors treated with docetaxel upregulated genes with Enrichr NCI-Nature pathway database. C-F. In vitro treatment of Caspase-3 +/+ MCF-7 cells with docetaxel induces Caspase-3, Caspase-9 and Capsase-8 cleavage, and no differences on Caspase-7 cleavage. Immunoblot analysis of cleaved Caspase-3 (C), cleaved Caspase-9 (D), Caspase-7 (E) and Caspase-8 in Caspase-3 -/- and +/+ MCF-7 cells at 0 and 72h after docetaxel (10 nM) treatment start. G. No differences in apoptosis between Caspase-3 -/- or +/+ MCF-7 cells treated with docetaxel. Annexin V/7AAD staining of Capase-3 -/- or +/+ MCF-7 cells after 72 h of treatment with docetaxel (10 nM). H. No cell growth differences between Caspase-3 -/- or +/+ MCF- 7 cells treated with docetaxel.