The Utility of Ultrasound in the Assessment of Traumatic Peripheral Nerve Lesions: Report of 4 Cases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Schwann Cell Supplementation in Neurosurgical Procedures After Neurotrauma Santiago R
ll Scienc Ce e f & o T l h a e Unda, J Cell Sci Ther 2018, 9:2 n r a r a p p u u DOI: 10.4172/2157-7013.1000281 y y o o J J Journal of Cell Science & Therapy ISSN: 2157-7013 Review Open Access Schwann Cell Supplementation in Neurosurgical Procedures after Neurotrauma Santiago R. Unda* Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina *Corresponding author: Santiago R. Unda, Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina, Tel: 3804277348; E-mail: [email protected] Rec Date: January 12, 2018, Acc Date: March 13, 2018, Pub Date: March 16, 2018 Copyright: © 2018 Santiago R. Unda. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Nerve trauma is a common cause of quality of life decline, especially in young people. Causing a high impact in personal, psychological and economic issues. The Peripheral Nerve Injury (PNI) with a several grade of axonotmesis and neurotmesis represents a real challenge for neurosurgeons. However, the basic science has greatly contribute to axonal degeneration and regeneration knowledge, making possible to implement in new protocols with molecular and cellular techniques for improve nerve re-growth and to restore motor and sensitive function. The Schwann cell transplantation from different stem cells origins is one of the potential tools for new therapies. In this briefly review is included the recent results of animal and human neurosurgery protocols of Schwann cells transplantation for nerve recovery after a PNI. -

Types and Classification of Nerve Injury: a Review
Indian Journal of Clinical Practice, Vol. 31, No. 5, October 2020 REVIEW ARTICLE Types and Classification of Nerve Injury: A Review R JAYASRI KRUPAA*, KMK MASTHAN†, ARAVINTHA BABU N‡, SONA B# ABSTRACT Nerve injuries are the most common conditions with varying symptoms, depending on the severity, intensity and nerves involved. Though much information is available on the mechanisms of injury and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve injuries and their classification. Keywords: Axonotmesis, neurotmesis, neurapraxia, Wallerian degeneration erve injuries are the most common conditions bundles of fibers called fascicles, which are covered with varying symptoms depending on the by perineurium. severity, intensity and nerves involved. N Â Epineurium: Finally, groups of fascicles are bundled Recovery after any nerve injury is variable. Though together to form the peripheral nerve (such as the much information exists on the mechanisms of injury median nerve), which is covered by epineurium. and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve CLASSIFICATION injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve Classification by Type of Nerve Injury injuries and classification of nerve injuries, which is There are three types of nerve injuries: useful in understanding their pathological basis, and to evaluate the prognosis for recovery. Nerve section Understanding the basic nerve anatomy is important Nerve section can be partial or complete, sharp or for the classification and also essential to evaluate blunt. -
Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography
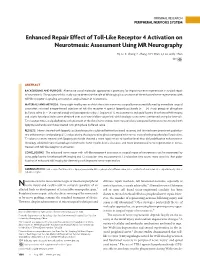
ORIGINAL RESEARCH PERIPHERAL NERVOUS SYSTEM Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography H.J. Li, X. Zhang, F. Zhang, X.H. Wen, L.J. Lu, and J. Shen ABSTRACT BACKGROUND AND PURPOSE: Alternative use of molecular approaches is promising for improving nerve regeneration in surgical repair of neurotmesis. The purpose of this study was to determine the role of MR imaging in assessment of the enhanced nerve regeneration with toll-like receptor 4 signaling activation in surgical repair of neurotmesis. MATERIALS AND METHODS: Forty-eight healthy rats in which the sciatic nerve was surgically transected followed by immediate surgical coaptation received intraperitoneal injection of toll-like receptor 4 agonist lipopolysaccharide (n ϭ 24, study group) or phosphate buffered saline (n ϭ 24, control group) until postoperative day 7. Sequential T2 measurements and gadofluorine M-enhanced MR imaging and sciatic functional index were obtained over an 8-week follow-up period, with histologic assessments performed at regular intervals. T2 relaxation times and gadofluorine enhancement of the distal nerve stumps were measured and compared between nerves treated with lipopolysaccharide and those treated with phosphate buffered saline. RESULTS: Nerves treated with lipopolysaccharide injection achieved better functional recovery and showed more prominent gadofluo- rine enhancement and prolonged T2 values during the degenerative phase compared with nerves treated with phosphate buffered saline. T2 values in nerves treated with lipopolysaccharide showed a more rapid return to baseline level than did gadofluorine enhancement. Histology exhibited more macrophage recruitment, faster myelin debris clearance, and more pronounced nerve regeneration in nerves treated with toll-like receptor 4 activation. -

Examination of the Shoulder Bruce S
Examination of the Shoulder Bruce S. Wolock, MD Towson Orthopaedic Associates 3 Joints, 1 Articulation 1. Sternoclavicular 2. Acromioclavicular 3. Glenohumeral 4. Scapulothoracic AC Separation Bony Landmarks 1. Suprasternal notch 2. Sternoclavicular joint 3. Coracoid 4. Acromioclavicular joint 5. Acromion 6. Greater tuberosity of the humerus 7. Bicipital groove 8. Scapular spine 9. Scapular borders-vertebral and lateral Sternoclavicular Dislocation Soft Tissues 1. Rotator Cuff 2. Subacromial bursa 3. Axilla 4. Muscles: a. Sternocleidomastoid b. Pectoralis major c. Biceps d. Deltoid Congenital Absence of Pectoralis Major Pectoralis Major Rupture Soft Tissues (con’t) e. Trapezius f. Rhomboid major and minor g. Latissimus dorsi h. Serratus anterior Range of Motion: Active and Passive 1. Abduction - 90 degrees 2. Adduction - 45 degrees 3. Extension - 45 degrees 4. Flexion - 180 degrees 5. Internal rotation – 90 degrees 6. External rotation – 45 degrees Muscle Testing 1. Flexion a. Primary - Anterior deltoid (axillary nerve, C5) - Coracobrachialis (musculocutaneous nerve, C5/6 b. Secondary - Pectoralis major - Biceps Biceps Rupture- Longhead Muscle Testing 2. Extension a. Primary - Latissimus dorsi (thoracodorsal nerve, C6/8) - Teres major (lower subscapular nerve, C5/6) - Posterior deltoid (axillary nerve, C5/6) b. Secondary - Teres minor - Triceps Abduction Primary a. Middle deltoid (axillary nerve, C5/6) b. Supraspinatus (suprascapular nerve, C5/6) Secondary a. Anterior and posterior deltoid b. Serratus anterior Deltoid Ruputure Axillary Nerve Palsy Adduction Primary a. Pectoralis major (medial and lateral pectoral nerves, C5-T1 b. Latissimus dorsi (thoracodorsal nerve, C6/8) Secondary a. Teres major b. Anterior deltoid External Rotation Primary a. Infraspinatus (suprascapular nerve, C5/6) b. Teres minor (axillary nerve, C5) Secondary a. -

Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know
Anaesthesia & Critical Care Medicine Journal ISSN: 2577-4301 Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know Kamel I* and Huck E Review Article Lewis Katz School of Medicine at Temple University, USA Volume 4 Issue 3 Received Date: June 20, 2019 *Corresponding author: Ihab Kamel, Lewis Katz School of Medicine at Temple Published Date: August 01, 2019 University, MEHP 3401 N. Broad street, 3rd floor outpatient building ( Zone-B), DOI: 10.23880/accmj-16000155 Philadelphia, United States, Tel: 2158066599; Email: [email protected] Abstract Peripheral nerve injury is a rare but significant perioperative complication. Despite a variety of investigations that include observational, experimental, human cadaveric and animal studies, we have an incomplete understanding of the etiology of PPNI and the means to prevent it. In this article we reviewed current knowledge pertinent to perioperative upper extremity peripheral nerve injury and optimal intraoperative patient positioning. Keywords: Nerve Fibers; Proprioception; Perineurium; Epineurium; Endoneurium; Neurapraxia; Ulnar Neuropathy Abbreviations: PPNI: Perioperative Peripheral Nerve 2018.The most common perioperative peripheral nerve Injury; MAP: Mean Arterial Pressure; ASA CCP: American injuries involve the upper extremity with ulnar Society of Anesthesiology Closed Claims Project; SSEP: neuropathy and brachial plexus injury being the most Somato Sensory Evoked Potentials frequent [3,4]. In this article we review upper extremity PPNI with regards to anatomy and physiology, Introduction mechanisms of injury, risk factors, and prevention of upper extremity PPNI. Perioperative peripheral nerve injury (PPNI) is a rare complication with a reported incidence of 0.03-0.1% [1,2]. Anatomy and Physiology of Peripheral PPNI is a significant source of patient disability and is the Nerves second most common cause of anesthesia malpractice claims [3,4]. -

Stichting Voor Ooglijders Prof. Dr. HJ
De publicatie van dit proefschrift werd mede mogelijk gemaakt met fmanciele steun van: Stichting voor Ooglijders Prof. Dr. H.J. Flieringa Stichting Medical Workshop BV Kabi Pharmacia Bournonville-Pharma BV Ter herinnering aan mijn vader Omslag: Henry Cannon I Ebbo Clerlo: CLINICAL ASPECTS AND ETIOLOGY OF FUCHS' HETEROCHROMIC CYCLITIS (KLINISCHE ASPECTEN EN ETIOLOGIE VAN DE HETEROCHROME CYCLITIS VAN FUCHS) proefschrift Ter verkrijging van de graad van doctor aan de Erasmus Universiteit Rotterdam op gezag van de Rector Magnificus Prof. dr. P.W.C. Akkermans M. Lit. en volgens besluit van het College van Dekanen. De openbare verdediding zal plaatsvinden op woensdag 3 November 1993 om 15.45 uur. door Ellen Carolien La Heij geboren te Arnstelveen PROMOTIE-COMMISSIE PROMOTORES' Prof. dr. P.T.V.M. de Jong Prof. dr. A. Kijlstra OVERIGE LEDEN, Prof. dr. F.T. Bosman Prof. dr. H.A. Drexhage CONTENTS Chapter 1 1.1 General Introduction ........................ 7 1. 2 Aim of the Thesis_ ................... __ ...... 8 Chapter 2 Fuchs' Heterochromic Cyclitis: Review of the Literature (submitted for publication) 2.1 Historical Background ........................ 9 2.2 Terminology and Classification ............... 9 2. 3 Epidemiology. .11 2. 4 Clinical Features ........................... 11. 2.5 Histopathology of the Iris ................. 22 2. 6 Etiologic Mechanisms ........................ 25 2.7 Therapy and Prognosis .................... ... 37 Chapter 3 Clin~c~l analysis of Fuchs' heterochromic cycl1t1s ........................................ 49 (Doc Ophthalmol. 1991;78:225-235). Chapter 4 Treatment and prognosis of secondary glaucoma in Fuchs' heterochromic cyclitis ............... .... 61 (Am J Ophthalmol. 1993, in press) Chapter 5 Quantitative analysis of iris translucency in Fuchs' heterochromic cyclitis ................. .. 83 (Invest Ophthalmol & Vis Sci. -

Orphanet Report Series Rare Diseases Collection
Marche des Maladies Rares – Alliance Maladies Rares Orphanet Report Series Rare Diseases collection DecemberOctober 2013 2009 List of rare diseases and synonyms Listed in alphabetical order www.orpha.net 20102206 Rare diseases listed in alphabetical order ORPHA ORPHA ORPHA Disease name Disease name Disease name Number Number Number 289157 1-alpha-hydroxylase deficiency 309127 3-hydroxyacyl-CoA dehydrogenase 228384 5q14.3 microdeletion syndrome deficiency 293948 1p21.3 microdeletion syndrome 314655 5q31.3 microdeletion syndrome 939 3-hydroxyisobutyric aciduria 1606 1p36 deletion syndrome 228415 5q35 microduplication syndrome 2616 3M syndrome 250989 1q21.1 microdeletion syndrome 96125 6p subtelomeric deletion syndrome 2616 3-M syndrome 250994 1q21.1 microduplication syndrome 251046 6p22 microdeletion syndrome 293843 3MC syndrome 250999 1q41q42 microdeletion syndrome 96125 6p25 microdeletion syndrome 6 3-methylcrotonylglycinuria 250999 1q41-q42 microdeletion syndrome 99135 6-phosphogluconate dehydrogenase 67046 3-methylglutaconic aciduria type 1 deficiency 238769 1q44 microdeletion syndrome 111 3-methylglutaconic aciduria type 2 13 6-pyruvoyl-tetrahydropterin synthase 976 2,8 dihydroxyadenine urolithiasis deficiency 67047 3-methylglutaconic aciduria type 3 869 2A syndrome 75857 6q terminal deletion 67048 3-methylglutaconic aciduria type 4 79154 2-aminoadipic 2-oxoadipic aciduria 171829 6q16 deletion syndrome 66634 3-methylglutaconic aciduria type 5 19 2-hydroxyglutaric acidemia 251056 6q25 microdeletion syndrome 352328 3-methylglutaconic -
Development of a Z-Stack Projection Imaging Protocol for a Nerve Allograft
DEVELOPMENT OF A Z-STACK PROJECTION IMAGING PROTOCOL FOR A NERVE ALLOGRAFT by SELVAANISH SELVAM Submitted in partial fulfillment of the requirements for the degree of Master of Science Dissertation Advisor: Dr. George F. Muschler Department of Biomedical Engineering CASE WESTERN RESERVE UNIVERSITY August 2018 CASE WESTERN RESERVE UNIVERSITY SCHOOL OF GRADUATE STUDIES We hereby approve the thesis of Selvaanish Selvam candidate for the degree of (Master of Science) *. Committee Chair Dr. George F. Muschler Committee Member Dr. Eben Alsberg Committee Member Dr. Robert Kirsch Committee Member Cynthia Boehm Date of Defense May 4th 2018 *we also certify that written approval has been obtained For any proprietary material contained therein 2 Table of Contents List of Tables……………………………………………………………………..4 Figures List……………………………………………………………………….5 Acknowledgments………………………………………………………………..6 List of Abbreviations………………………………………………………….....7 Abstract…………………………………………………………………………...8 Introduction……………………………………………………………………..10 Methods………………………………………………………………………….21 Data and Analysis………………………………………………………………31 Conclusions and Future Directions……………………………………………51 References……………………………………………………………………….53 3 List of Tables Table 1: Overall summary of ratios and retention rates……………………..31 Table 2: Selection Ratio for grafts (3X – 10-minute rinse) ………………….35 Table 3: Selection Ratio for grafts (15-minute soak) ………………………...35 4 List of Figures: Figure 1: 2D 10X DAPI stained image using current techniques…….……….9 Figure 2: Peripheral Nerve Anatomy………………………………………….10 -

Restoration of Neurological Function Following Peripheral Nerve Trauma
International Journal of Molecular Sciences Review Restoration of Neurological Function Following Peripheral Nerve Trauma Damien P. Kuffler 1,* and Christian Foy 2 1 Institute of Neurobiology, Medical Sciences Campus, University of Puerto Rico, 201 Blvd. del Valle, San Juan, PR 00901, USA 2 Section of Orthopedic Surgery, Medical Sciences Campus, University of Puerto Rico, San Juan, PR 00901, USA; [email protected] * Correspondence: dkuffl[email protected] Received: 12 January 2020; Accepted: 3 March 2020; Published: 6 March 2020 Abstract: Following peripheral nerve trauma that damages a length of the nerve, recovery of function is generally limited. This is because no material tested for bridging nerve gaps promotes good axon regeneration across the gap under conditions associated with common nerve traumas. While many materials have been tested, sensory nerve grafts remain the clinical “gold standard” technique. This is despite the significant limitations in the conditions under which they restore function. Thus, they induce reliable and good recovery only for patients < 25 years old, when gaps are <2 cm in length, and when repairs are performed <2–3 months post trauma. Repairs performed when these values are larger result in a precipitous decrease in neurological recovery. Further, when patients have more than one parameter larger than these values, there is normally no functional recovery. Clinically, there has been little progress in developing new techniques that increase the level of functional recovery following peripheral nerve injury. This paper examines the efficacies and limitations of sensory nerve grafts and various other techniques used to induce functional neurological recovery, and how these might be improved to induce more extensive functional recovery. -

Dorsal Scapular Nerve Neuropathy: a Narrative Review of the Literature Brad Muir, Bsc.(Hons), DC, FRCCSS(C)1
ISSN 0008-3194 (p)/ISSN 1715-6181 (e)/2017/128–144/$2.00/©JCCA 2017 Dorsal scapular nerve neuropathy: a narrative review of the literature Brad Muir, BSc.(Hons), DC, FRCCSS(C)1 Objective: The purpose of this paper is to elucidate Objectif : Ce document a pour objectif d’élucider this little known cause of upper back pain through a cette cause peu connue de douleur dans le haut du narrative review of the literature and to discuss the dos par un examen narratif de la littérature, ainsi que possible role of the dorsal scapular nerve (DSN) in de discuter du rôle possible du nerf scapulaire dorsal the etiopathology of other similar diagnoses in this (NSD) dans l’étiopathologie d’autres diagnostics area including cervicogenic dorsalgia (CD), notalgia semblables dans ce domaine, y compris la dorsalgie paresthetica (NP), SICK scapula and a posterolateral cervicogénique (DC), la notalgie paresthésique (NP), arm pain pattern. l’omoplate SICK et un schéma de douleur postéro- Background: Dorsal scapular nerve (DSN) latérale au bras. neuropathy has been a rarely thought of differential Contexte : La neuropathie du nerf scapulaire dorsal diagnosis for mid scapular, upper to mid back and (NSD) constitue un diagnostic différentiel rare pour la costovertebral pain. These are common conditions douleur mi-scapulaire, costo-vertébrale et au bas/haut presenting to chiropractic, physiotherapy, massage du dos. Il s’agit de troubles communs qui surgissent therapy and medical offices. dans les cabinets de chiropratique, de physiothérapie, de Methods: The methods used to gather articles for this massothérapie et de médecin. paper included: searching electronic databases; and Méthodologie : Les méthodes utilisées pour hand searching relevant references from journal articles rassembler les articles de ce document comprenaient la and textbook chapters. -

Painful Abdominal Wall Nerves
CASE REPORT Reconstructive Treatment of Painful Nerves in the Abdominal Wall Using Processed Nerve Allografts Andrew Bi, BS Eugene Park, MD Summary: Neuromas can be a debilitating cause of pain and often negatively af- Gregory A. Dumanian, MD fect patients’ quality of life. One effective method of treatment involves surgical resection of the painful neuroma and use of a processed nerve allograft to repair the injured nerve segment. Giving the nerve “somewhere to go and something to do” has been shown to effectively alleviate pain in upper and lower extremities. We present the first report of this concept to treat a painful neuroma of the ab- dominal wall that developed following a laparoscopic gastric bypass. The neuroma was excised, and the affected nerve was reconstructed using a processed nerve allograft as an interposition graft, with resolution of pain and gradual return of normal sensation. Patient-reported outcomes were measured using the Patient Reported Outcomes Measurement Information System. Neuroma excision with concurrent interposition grafting using processed nerve allografts may be a promising method of treatment for postsurgical painful neuromas of the trunk. Bi et al. (Plast Reconstr Surg Glob Open 2018;6:e1670; doi: 10.1097/GOX.0000000000001670; Published online 6 March 2018.) INTRODUCTION and unacceptable repeat surgical rates.2 And while wrap- Painful neuromas can form following any surgery when ping the distal point of a painful nerve postneuroma exci- nerves are injured due to cautery or traction. Nerve injury sion -

Board Review for Anatomy
Board Review for Anatomy John A. McNulty, Ph.D. Spring, 2005 . LOYOLA UNIVERSITY CHICAGO Stritch School of Medicine Key Skeletal landmarks • Head - mastoid process, angle of mandible, occipital protuberance • Neck – thyroid cartilage, cricoid cartilage • Thorax - jugular notch, sternal angle, xiphoid process, coracoid process, costal arch • Back - vertebra prominence, scapular spine (acromion), iliac crest • UE – epicondyles, styloid processes, carpal bones. • Pelvis – ant. sup. iliac spine, pubic tubercle • LE – head of fibula, malleoli, tarsal bones Key vertebral levels • C2 - angle of mandible • C4 - thyroid notch • C6 - cricoid cartilage - esophagus, trachea begin • C7 - vertebra prominence • T2 - jugular notch; scapular spine • T4/5 - sternal angle - rib 2 articulates, trachea divides • T9 - xiphisternum • L1/L2 - pancreas; spinal cord ends. • L4 - iliac crest; umbilicus; aorta divides • S1 - sacral promontory Upper limb nerve lesions Recall that any muscle that crosses a joint, acts on that joint. Also recall that muscles innervated by individual nerves within compartments tend to have similar actions. • Long thoracic n. - “winged” scapula. • Upper trunk (C5,C6) - Erb Duchenne - shoulder rotators, musculocutaneous • Lower trunk (C8, T1) - Klumpke’s - ulnar nerve (interossei muscle) • Radial nerve – (Saturday night palsy) - wrist drop • Median nerve (recurrent median) – thenar compartment - thumb • Ulnar nerve - interossei muscles. Lower limb nerve lesions Review actions of the various compartments. • Lumbosacral lesions - usually