CMA Analysis Identifies Homozygous Deletion of MCPH1 in 2 Brothers with Primary Microcephaly-1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mutations in CDK5RAP2 Cause Seckel Syndrome Go¨ Khan Yigit1,2,3,A, Karen E
ORIGINAL ARTICLE Mutations in CDK5RAP2 cause Seckel syndrome Go¨ khan Yigit1,2,3,a, Karen E. Brown4,a,Hu¨ lya Kayserili5, Esther Pohl1,2,3, Almuth Caliebe6, Diana Zahnleiter7, Elisabeth Rosser8, Nina Bo¨ gershausen1,2,3, Zehra Oya Uyguner5, Umut Altunoglu5, Gudrun Nu¨ rnberg2,3,9, Peter Nu¨ rnberg2,3,9, Anita Rauch10, Yun Li1,2,3, Christian Thomas Thiel7 & Bernd Wollnik1,2,3 1Institute of Human Genetics, University of Cologne, Cologne, Germany 2Center for Molecular Medicine Cologne (CMMC), University of Cologne, Cologne, Germany 3Cologne Excellence Cluster on Cellular Stress Responses in Aging-Associated Diseases (CECAD), University of Cologne, Cologne, Germany 4Chromosome Biology Group, MRC Clinical Sciences Centre, Imperial College School of Medicine, Hammersmith Hospital, London, W12 0NN, UK 5Department of Medical Genetics, Istanbul Medical Faculty, Istanbul University, Istanbul, Turkey 6Institute of Human Genetics, Christian-Albrechts-University of Kiel, Kiel, Germany 7Institute of Human Genetics, Friedrich-Alexander University Erlangen-Nuremberg, Erlangen, Germany 8Department of Clinical Genetics, Great Ormond Street Hospital for Children, London, WC1N 3EH, UK 9Cologne Center for Genomics, University of Cologne, Cologne, Germany 10Institute of Medical Genetics, University of Zurich, Schwerzenbach-Zurich, Switzerland Keywords Abstract CDK5RAP2, CEP215, microcephaly, primordial dwarfism, Seckel syndrome Seckel syndrome is a heterogeneous, autosomal recessive disorder marked by pre- natal proportionate short stature, severe microcephaly, intellectual disability, and Correspondence characteristic facial features. Here, we describe the novel homozygous splice-site Bernd Wollnik, Center for Molecular mutations c.383+1G>C and c.4005-9A>GinCDK5RAP2 in two consanguineous Medicine Cologne (CMMC) and Institute of families with Seckel syndrome. CDK5RAP2 (CEP215) encodes a centrosomal pro- Human Genetics, University of Cologne, tein which is known to be essential for centrosomal cohesion and proper spindle Kerpener Str. -

Par6c Is at the Mother Centriole and Controls Centrosomal Protein
860 Research Article Par6c is at the mother centriole and controls centrosomal protein composition through a Par6a-dependent pathway Vale´rian Dormoy, Kati Tormanen and Christine Su¨ tterlin* Department of Developmental and Cell Biology, University of California, Irvine, Irvine, CA 92697-2300, USA *Author for correspondence ([email protected]) Accepted 3 December 2012 Journal of Cell Science 126, 860–870 ß 2013. Published by The Company of Biologists Ltd doi: 10.1242/jcs.121186 Summary The centrosome contains two centrioles that differ in age, protein composition and function. This non-membrane bound organelle is known to regulate microtubule organization in dividing cells and ciliogenesis in quiescent cells. These specific roles depend on protein appendages at the older, or mother, centriole. In this study, we identified the polarity protein partitioning defective 6 homolog gamma (Par6c) as a novel component of the mother centriole. This specific localization required the Par6c C-terminus, but was independent of intact microtubules, the dynein/dynactin complex and the components of the PAR polarity complex. Par6c depletion resulted in altered centrosomal protein composition, with the loss of a large number of proteins, including Par6a and p150Glued, from the centrosome. As a consequence, there were defects in ciliogenesis, microtubule organization and centrosome reorientation during migration. Par6c interacted with Par3 and aPKC, but these proteins were not required for the regulation of centrosomal protein composition. Par6c also associated with Par6a, which controls protein recruitment to the centrosome through p150Glued. Our study is the first to identify Par6c as a component of the mother centriole and to report a role of a mother centriole protein in the regulation of centrosomal protein composition. -

Supplemental Information Proximity Interactions Among Centrosome
Current Biology, Volume 24 Supplemental Information Proximity Interactions among Centrosome Components Identify Regulators of Centriole Duplication Elif Nur Firat-Karalar, Navin Rauniyar, John R. Yates III, and Tim Stearns Figure S1 A Myc Streptavidin -tubulin Merge Myc Streptavidin -tubulin Merge BirA*-PLK4 BirA*-CEP63 BirA*- CEP192 BirA*- CEP152 - BirA*-CCDC67 BirA* CEP152 CPAP BirA*- B C Streptavidin PCM1 Merge Myc-BirA* -CEP63 PCM1 -tubulin Merge BirA*- CEP63 DMSO - BirA* CEP63 nocodazole BirA*- CCDC67 Figure S2 A GFP – + – + GFP-CEP152 + – + – Myc-CDK5RAP2 + + + + (225 kDa) Myc-CDK5RAP2 (216 kDa) GFP-CEP152 (27 kDa) GFP Input (5%) IP: GFP B GFP-CEP152 truncation proteins Inputs (5%) IP: GFP kDa 1-7481-10441-1290218-1654749-16541045-16541-7481-10441-1290218-1654749-16541045-1654 250- Myc-CDK5RAP2 150- 150- 100- 75- GFP-CEP152 Figure S3 A B CEP63 – – + – – + GFP CCDC14 KIAA0753 Centrosome + – – + – – GFP-CCDC14 CEP152 binding binding binding targeting – + – – + – GFP-KIAA0753 GFP-KIAA0753 (140 kDa) 1-496 N M C 150- 100- GFP-CCDC14 (115 kDa) 1-424 N M – 136-496 M C – 50- CEP63 (63 kDa) 1-135 N – 37- GFP (27 kDa) 136-424 M – kDa 425-496 C – – Inputs (2%) IP: GFP C GFP-CEP63 truncation proteins D GFP-CEP63 truncation proteins Inputs (5%) IP: GFP Inputs (5%) IP: GFP kDa kDa 1-135136-424425-4961-424136-496FL Ctl 1-135136-424425-4961-424136-496FL Ctl 1-135136-424425-4961-424136-496FL Ctl 1-135136-424425-4961-424136-496FL Ctl Myc- 150- Myc- 100- CCDC14 KIAA0753 100- 100- 75- 75- GFP- GFP- 50- CEP63 50- CEP63 37- 37- Figure S4 A siCtl -

Supplementary Data
SUPPLEMENTARY DATA A cyclin D1-dependent transcriptional program predicts clinical outcome in mantle cell lymphoma Santiago Demajo et al. 1 SUPPLEMENTARY DATA INDEX Supplementary Methods p. 3 Supplementary References p. 8 Supplementary Tables (S1 to S5) p. 9 Supplementary Figures (S1 to S15) p. 17 2 SUPPLEMENTARY METHODS Western blot, immunoprecipitation, and qRT-PCR Western blot (WB) analysis was performed as previously described (1), using cyclin D1 (Santa Cruz Biotechnology, sc-753, RRID:AB_2070433) and tubulin (Sigma-Aldrich, T5168, RRID:AB_477579) antibodies. Co-immunoprecipitation assays were performed as described before (2), using cyclin D1 antibody (Santa Cruz Biotechnology, sc-8396, RRID:AB_627344) or control IgG (Santa Cruz Biotechnology, sc-2025, RRID:AB_737182) followed by protein G- magnetic beads (Invitrogen) incubation and elution with Glycine 100mM pH=2.5. Co-IP experiments were performed within five weeks after cell thawing. Cyclin D1 (Santa Cruz Biotechnology, sc-753), E2F4 (Bethyl, A302-134A, RRID:AB_1720353), FOXM1 (Santa Cruz Biotechnology, sc-502, RRID:AB_631523), and CBP (Santa Cruz Biotechnology, sc-7300, RRID:AB_626817) antibodies were used for WB detection. In figure 1A and supplementary figure S2A, the same blot was probed with cyclin D1 and tubulin antibodies by cutting the membrane. In figure 2H, cyclin D1 and CBP blots correspond to the same membrane while E2F4 and FOXM1 blots correspond to an independent membrane. Image acquisition was performed with ImageQuant LAS 4000 mini (GE Healthcare). Image processing and quantification were performed with Multi Gauge software (Fujifilm). For qRT-PCR analysis, cDNA was generated from 1 µg RNA with qScript cDNA Synthesis kit (Quantabio). qRT–PCR reaction was performed using SYBR green (Roche). -

Supplementary Table S1. Correlation Between the Mutant P53-Interacting Partners and PTTG3P, PTTG1 and PTTG2, Based on Data from Starbase V3.0 Database
Supplementary Table S1. Correlation between the mutant p53-interacting partners and PTTG3P, PTTG1 and PTTG2, based on data from StarBase v3.0 database. PTTG3P PTTG1 PTTG2 Gene ID Coefficient-R p-value Coefficient-R p-value Coefficient-R p-value NF-YA ENSG00000001167 −0.077 8.59e-2 −0.210 2.09e-6 −0.122 6.23e-3 NF-YB ENSG00000120837 0.176 7.12e-5 0.227 2.82e-7 0.094 3.59e-2 NF-YC ENSG00000066136 0.124 5.45e-3 0.124 5.40e-3 0.051 2.51e-1 Sp1 ENSG00000185591 −0.014 7.50e-1 −0.201 5.82e-6 −0.072 1.07e-1 Ets-1 ENSG00000134954 −0.096 3.14e-2 −0.257 4.83e-9 0.034 4.46e-1 VDR ENSG00000111424 −0.091 4.10e-2 −0.216 1.03e-6 0.014 7.48e-1 SREBP-2 ENSG00000198911 −0.064 1.53e-1 −0.147 9.27e-4 −0.073 1.01e-1 TopBP1 ENSG00000163781 0.067 1.36e-1 0.051 2.57e-1 −0.020 6.57e-1 Pin1 ENSG00000127445 0.250 1.40e-8 0.571 9.56e-45 0.187 2.52e-5 MRE11 ENSG00000020922 0.063 1.56e-1 −0.007 8.81e-1 −0.024 5.93e-1 PML ENSG00000140464 0.072 1.05e-1 0.217 9.36e-7 0.166 1.85e-4 p63 ENSG00000073282 −0.120 7.04e-3 −0.283 1.08e-10 −0.198 7.71e-6 p73 ENSG00000078900 0.104 2.03e-2 0.258 4.67e-9 0.097 3.02e-2 Supplementary Table S2. -

Genomic Discovery of an Evolutionarily Programmed Modality for Small-Molecule Targeting of an Intractable Protein Surface
Genomic discovery of an evolutionarily programmed modality for small-molecule targeting of an intractable protein surface Uddhav K. Shigdela,1,2, Seung-Joo Leea,1,3, Mathew E. Sowaa,1,4, Brian R. Bowmana,1,5, Keith Robisona,6, Minyun Zhoua,7, Khian Hong Puaa,8, Dylan T. Stilesa,6, Joshua A. V. Blodgetta,9, Daniel W. Udwarya,10, Andrew T. Rajczewskia,11, Alan S. Manna,12, Siavash Mostafavia,13, Tara Hardyb, Sukrat Aryab,14, Zhigang Wenga,15, Michelle Stewarta,16, Kyle Kenyona,6, Jay P. Morgensterna,6, Ende Pana,17, Daniel C. Graya,6, Roy M. Pollocka,4, Andrew M. Fryb, Richard D. Klausnerc,18, Sharon A. Townsona,19, and Gregory L. Verdinea,d,e,f,2,18,20 Contributed by Richard D. Klausner, April 21, 2020 (sent for review April 8, 2020; reviewed by Chuan He and Ben Shen) The vast majority of intracellular protein targets are refractory toward small-molecule therapeutic engagement, and additional Author contributions: U.K.S., S.-J.L., M.E.S., B.R.B., K.R., Z.W., M.S., D.C.G., R.M.P., A.M.F., R.D.K., S.A.T., and G.L.V. designed research; U.K.S., S.-J.L., M.E.S., K.R., M.Z., K.H.P., D.T.S., therapeutic modalities are needed to overcome this deficiency. J.A.V.B., D.W.U., A.T.R., A.S.M., S.M., T.H., S.A., K.K., J.P.M., E.P., R.D.K., and G.L.V. performed Here, the identification and characterization of a natural product, research; M.E.S., D.T.S., and A.M.F. -

Polo-Like Kinase 1 Regulates Nlp, a Centrosome Protein Involved in Microtubule Nucleation
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Developmental Cell, Vol. 5, 113–125, July, 2003, Copyright 2003 by Cell Press Polo-like Kinase 1 Regulates Nlp, a Centrosome Protein Involved in Microtubule Nucleation Martina Casenghi,1,2 Patrick Meraldi,1,2,3 Rieder, 1999; Palazzo et al., 2000). Although centrosome Ulrike Weinhart,1 Peter I. Duncan,1,4 maturation is important for mitotic spindle formation, the Roman Ko¨ rner,1 and Erich A. Nigg1,* underlying mechanisms remain largely unknown. Two 1Department of Cell Biology protein kinases, Polo-like kinase 1 (Plk1; Lane and Nigg, Max Planck Institute of Biochemistry 1996; Sunkel and Glover, 1988) and Aurora-A (Berdnik Am Klopferspitz 18a and Knoblich, 2002; Hannak et al., 2001), as well as D-82152 Martinsried protein phosphatase 4 (Helps et al., 1998; Sumiyoshi Germany et al., 2002), have been implicated in the regulation of centrosome maturation, but the substrates of these en- zymes await identification. Also acting at the G2/M tran- sition, the protein kinase Nek2 and a member of the Summary phosphatase 1 family contribute to regulate centrosome separation, in part through phosphorylation of the centri- In animal cells, most microtubules are nucleated at ole-associated protein C-Nap1 (Fry et al., 1998b; Helps centrosomes. At the onset of mitosis, centrosomes et al., 2000; Mayor et al., 2000). undergo a structural reorganization, termed matura- The discovery of ␥-tubulin and ␥-tubulin-containing tion, which leads to increased microtubule nucleation multiprotein complexes has greatly advanced our un- activity. -

Centrosome Impairment Causes DNA Replication Stress Through MLK3
bioRxiv preprint doi: https://doi.org/10.1101/2020.01.09.898684; this version posted January 10, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Centrosome impairment causes DNA replication stress through MLK3/MK2 signaling and R-loop formation Zainab Tayeh 1, Kim Stegmann 1, Antonia Kleeberg 1, Mascha Friedrich 1, Josephine Ann Mun Yee Choo 1, Bernd Wollnik 2, and Matthias Dobbelstein 1* 1) Institute of Molecular Oncology, Göttingen Center of Molecular Biosciences (GZMB), University Medical Center Göttingen, Göttingen, Germany 2) Institute of Human Genetics, University Medical Center Göttingen, Göttingen, Germany *Lead Contact. Correspondence and requests for materials should be addressed to M. D. (e-mail: [email protected]; ORCID 0000-0001-5052-3967) Running title: Centrosome integrity supports DNA replication Key words: Centrosome, CEP152, CCP110, SASS6, CEP152, Polo-like kinase 4 (PLK4), DNA replication, DNA fiber assays, R-loops, MLK3, MK2 alias MAPKAPK2, Seckel syndrome, microcephaly. Highlights: • Centrosome defects cause replication stress independent of mitosis. • MLK3, p38 and MK2 (alias MAPKAPK2) are signalling between centrosome defects and DNA replication stress through R-loop formation. • Patient-derived cells with defective centrosomes display replication stress, whereas inhibition of MK2 restores their DNA replication fork progression and proliferation. 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.01.09.898684; this version posted January 10, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. -

CENTROSOME NUMBER HOMEOSTASIS: LESSONS from CEP135 ISOFORM DYSREGULATION in BREAST CANCER by DIVYA GANAPATHI SANKARAN Bachelor
CENTROSOME NUMBER HOMEOSTASIS: LESSONS FROM CEP135 ISOFORM DYSREGULATION IN BREAST CANCER By DIVYA GANAPATHI SANKARAN Bachelor of Technology, Anna University, India, 2013 A thesis submitted to the Faculty of the Graduate School of the University of Colorado in partial fulfillment of the requirements for the degree of Doctor of Philosophy Cancer Biology Program 2019 This thesis for the Doctor of Philosophy degree by Divya Ganapathi Sankaran has been approved for the Cancer Biology Program By Rytis Prekeris, Chair Jeffrey Moore David Bentley Heide Ford Mary Reyland Chad G Pearson, Advisor Date: 05/17/2019 ii Ganapathi Sankaran, Divya (Ph.D., Cancer Biology) Centrosome Number Homeostasis: Lessons from CEP135 Isoform Dysregulation in Breast Cancer Thesis Directed by Associate Professor Chad G. Pearson ABSTRACT The centrosome, comprised of two centrioles surrounded by pericentriolar material, is the cell’s central microtubule organizing center. Centrosome duplication is coupled with the cell cycle such that centrosomes duplicate once in S phase. Loss of such coupling produces supernumerary centrosomes, a condition called centrosome amplification (CA). CA can promote hallmarks of tumorigenesis. In this thesis, I investigate the contribution of centriole overduplication to CA and its consequences on microtubule organization and genomic stability in breast cancer cells. CEP135, a centriole assembly protein, is dysregulated in some breast cancers. We previously identified a short isoform of CEP135, CEP135mini that represses centriole duplication. CEP135mini represses centriole duplication by limiting the localization of essential proteins required for centriole duplication. Interestingly, the relative level of CEP135full to CEP135mini (the CEP135full:mini ratio) is higher in centrosome amplified breast cancer cell lines. -

Characterization of NIP2/Centrobin, a Novel Substrate of Nek2, and Its Potential Role in Microtubule Stabilization
2106 Research Article Characterization of NIP2/centrobin, a novel substrate of Nek2, and its potential role in microtubule stabilization Yeontae Jeong, Jungmin Lee, Kyeongmi Kim, Jae Cheal Yoo and Kunsoo Rhee* Department of Biological Sciences and Research Center for Functional Cellulomics, Seoul National University, Seoul 151-742, Korea *Author for correspondence (e-mail: [email protected]) Accepted 11 April 2007 Journal of Cell Science 120, 2106-2116 Published by The Company of Biologists 2007 doi:10.1242/jcs.03458 Summary Nek2 is a mitotic kinase whose activity varies during the associated with microtubules. Knockdown of NIP2 showed cell cycle. It is well known that Nek2 is involved in significant reduction of microtubule organizing activity, centrosome splitting, and a number of studies have cell shrinkage, defects in spindle assembly and abnormal indicated that Nek2 is crucial for maintaining the integrity nuclear morphology. Based on our results, we propose that of centrosomal structure and microtubule nucleation NIP2 has a role in stabilizing the microtubule structure. activity. In the present study, we report that NIP2, Phosphorylation may be crucial for mobilization of the previously identified as centrobin, is a novel substrate of protein to a new microtubule and stabilizing it. Nek2. NIP2 was daughter-centriole-specific, but was also found in association with a stable microtubule network of cytoplasm. Ectopic NIP2 formed aggregates but was Key words: NIP2, Centrobin, Nek2, Centrosome, Mitosis, dissolved by Nek2 into small pieces and eventually Microtubule Introduction through the phosphorylation-induced displacement of C-Nap1 Phosphorylation is one of major control mechanisms used from the centriolar ends (reviewed in Fry, 2002). -
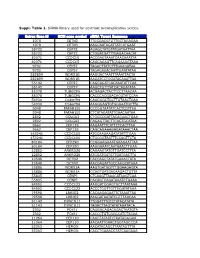
Suppl. Table 1
Suppl. Table 1. SiRNA library used for centriole overduplication screen. Entrez Gene Id NCBI gene symbol siRNA Target Sequence 1070 CETN3 TTGCGACGTGTTGCTAGAGAA 1070 CETN3 AAGCAATAGATTATCATGAAT 55722 CEP72 AGAGCTATGTATGATAATTAA 55722 CEP72 CTGGATGATTTGAGACAACAT 80071 CCDC15 ACCGAGTAAATCAACAAATTA 80071 CCDC15 CAGCAGAGTTCAGAAAGTAAA 9702 CEP57 TAGACTTATCTTTGAAGATAA 9702 CEP57 TAGAGAAACAATTGAATATAA 282809 WDR51B AAGGACTAATTTAAATTACTA 282809 WDR51B AAGATCCTGGATACAAATTAA 55142 CEP27 CAGCAGATCACAAATATTCAA 55142 CEP27 AAGCTGTTTATCACAGATATA 85378 TUBGCP6 ACGAGACTACTTCCTTAACAA 85378 TUBGCP6 CACCCACGGACACGTATCCAA 54930 C14orf94 CAGCGGCTGCTTGTAACTGAA 54930 C14orf94 AAGGGAGTGTGGAAATGCTTA 5048 PAFAH1B1 CCCGGTAATATCACTCGTTAA 5048 PAFAH1B1 CTCATAGATATTGAACAATAA 2802 GOLGA3 CTGGCCGATTACAGAACTGAA 2802 GOLGA3 CAGAGTTACTTCAGTGCATAA 9662 CEP135 AAGAATTTCATTCTCACTTAA 9662 CEP135 CAGCAGAAAGAGATAAACTAA 153241 CCDC100 ATGCAAGAAGATATATTTGAA 153241 CCDC100 CTGCGGTAATTTCCAGTTCTA 80184 CEP290 CCGGAAGAAATGAAGAATTAA 80184 CEP290 AAGGAAATCAATAAACTTGAA 22852 ANKRD26 CAGAAGTATGTTGATCCTTTA 22852 ANKRD26 ATGGATGATGTTGATGACTTA 10540 DCTN2 CACCAGCTATATGAAACTATA 10540 DCTN2 AACGAGATTGCCAAGCATAAA 25886 WDR51A AAGTGATGGTTTGGAAGAGTA 25886 WDR51A CCAGTGATGACAAGACTGTTA 55835 CENPJ CTCAAGTTAAACATAAGTCAA 55835 CENPJ CACAGTCAGATAAATCTGAAA 84902 CCDC123 AAGGATGGAGTGCTTAATAAA 84902 CCDC123 ACCCTGGTTGTTGGATATAAA 79598 LRRIQ2 CACAAGAGAATTCTAAATTAA 79598 LRRIQ2 AAGGATAATATCGTTTAACAA 51143 DYNC1LI1 TTGGATTTGTCTATACATATA 51143 DYNC1LI1 TAGACTTAGTATATAAATACA 2302 FOXJ1 CAGGACAGACAGACTAATGTA -

Spink2 Modulates Apoptotic Susceptibility and Is a Candidate Gene in the Rgcs1 QTL That Affects Retinal Ganglion Cell Death After Optic Nerve Damage
Spink2 Modulates Apoptotic Susceptibility and Is a Candidate Gene in the Rgcs1 QTL That Affects Retinal Ganglion Cell Death after Optic Nerve Damage Joel A. Dietz1., Margaret E. Maes1., Shuang Huang2, Brian S. Yandell2, Cassandra L. Schlamp1, Angela D. Montgomery1, R. Rand Allingham3, Michael A. Hauser3, Robert W. Nickells1* 1 Department of Ophthalmology and Visual Sciences, University of Wisconsin, Madison, Wisconsin, United States of America, 2 Department of Biostatistics, University of Wisconsin, Madison, Wisconsin, United States of America, 3 Center for Human Genetics, Department of Medicine, Duke University Medical Center, Durham, North Carolina, United States of America Abstract The Rgcs1 quantitative trait locus, on mouse chromosome 5, influences susceptibility of retinal ganglion cells to acute damage of the optic nerve. Normally resistant mice (DBA/2J) congenic for the susceptible allele from BALB/cByJ mice exhibit susceptibility to ganglion cells, not only in acute optic nerve crush, but also to chronic inherited glaucoma that is characteristic of the DBA/2J strain as they age. SNP mapping of this QTL has narrowed the region of interest to 1 Mb. In this region, a single gene (Spink2) is the most likely candidate for this effect. Spink2 is expressed in retinal ganglion cells and is increased after optic nerve damage. This gene is also polymorphic between resistant and susceptible strains, containing a single conserved amino acid change (threonine to serine) and a 220 bp deletion in intron 1 that may quantitatively alter endogenous expression levels between strains. Overexpression of the different variants of Spink2 in D407 tissue culture cells also increases their susceptibility to the apoptosis-inducing agent staurosporine in a manner consistent with the differential susceptibility between the DBA/2J and BALB/cByJ strains.