Guideline: Assessment & Treatment of Surgical Wounds
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Arterial Leg Ulcer Clinical Pathway
Waterloo Wellington Integrated Wound Care Program Evidence-Based Wound Care Arterial Leg Ulcer Clinical Pathway 0-7 Days Expected Outcomes Notes Most Responsible Physician(MRP)/Nurse Practitioner (NP) Refer patient to ‘Care Connects’ if no responsible practitioner currently involved with patient identified/informed Determine if MRP/NP is part of Family Health Team (FHT) or Community Health Centre (CHC) and consider additional supports available Medical/surgical history and co-morbidity management Risk factors include: Chronic renal disease considered within care plan Smoking Congestive heart failure Diabetes mellitus Impaired liver function Hyperlipidemia Use of systemic steroids, Hypertension immunosuppressive and chemotherapy Coronary artery disease >70 years of age History of cerebral vascular accident Age 50-69 years with history of diabetes (CVA) or smoking Low hemoglobin < 50 years with diabetes and one other Obesity atherosclerotic factor Poor nutrition History of vascular surgery or deep vein Decreased thyroid function thrombosis Psoriasis Bleeding disorders Autoimmune diseases Family history of arterial disease Medication reconciliation and their impact on wound healing Prescription, non-prescription, naturopathic and illicit drug use (including e-cigarettes, reviewed inhaled substances and nicotine replacement therapy) Medications that can affect healing include: chemotherapy, anticoagulants, antiplatelets, corticosteroids, vasoconstrictors, antihypertensives, diuretics and immunosepressive drugs Other -

Caring for Yourself After Surgery: Preventing Surgical Site Infections
CARE AT HOME SERIES CARE AT HOME SERIES Caring for Yourself After Surgery Caring for Yourself After Surgery Preventing Surgical Site Infections Preventing Surgical Site Infections Wounds Canada has developed this simple guide that can be used by patients and their care partners when they are looking after a surgical wound. It provides guidance on things to do before and after surgery to help prevent infections and recognize the signs of infections if they do occur. In the past, people stayed in hospital for days or weeks following surgery. In those days, many of the complications that can occur soon after surgery (like infections, heart problems or bleeding) were treated when patients were still recovering in hospital. Today, patients having surgery get home Uninfected, healed surgical incision site. (See page 4 for faster than ever, often even the same day. Surgical uninfected and infected surgical incision sites.) site infections (SSIs) that were once treated in hospital are now being managed by patients at home. The good news is that there are actions you can take before and after your surgery to reduce the chances of developing a serious SSI. What is a surgical site infection? A surgical site infection is a problem where there are too many bacteria or really dangerous, active bacteria in your surgical incision. SSIs cause pain and delay wound healing. In more severe cases, SSIs can spread into the bloodstream (a condition called sepsis), which can lead to tissue loss, organ failure and death. A surgical site infection can be on the surface or deep. How much damage it does depends on how healthy you are as well as how strongly the bacteria affect your tissues. -

Causes of Surgical Wound Dehiscence: a Multicenter Study
J Wound Manag Res 2018 September;14(2):74-79 pISSN 2586-0402 https://doi.org/10.22467/jwmr.2018.00374 eISSN 2586-0410 Journal of Wound Management and Research Causes of Surgical Wound Dehiscence: A Multicenter Study Jeong Jin Chun1, Seok Min Yoon1, Woo Jin Song1, Hyun Gyo Jeong1, Chang Yong Choi2, Syeo Young Wee1 1Department of Plastic and Reconstructive Surgery, College of Medicine, Soonchunhyang University, Gumi; 2Department of Plastic and Reconstructive Surgery, College of Medicine, Soonchunhyang University, Bucheon, Korea Abstract Surgical wound dehiscence is a postoperative complication involving breakdown of surgical incision site. Despite the in- creased knowledge of wound healing mechanism before and after surgery, wound dehiscence may increase the length of hospital stay, increase patient inconvenience and rates of re-operation. The purpose of this study was to analyze the causes of wound dehiscence in patients undergoing reoperation at 4 hospitals of Soonchunhyang Medical Center. The number of patients in each hospital and those operated previously were compared. In addition, other characteristics of patients were compared in patients who underwent reoperation. In 22 out of 1,026 patients consulted at the Seoul hos- pital, 32 cases out of 1,295 at Bucheon hospital, 14 cases out of 1,687 at Cheonan hospital and 15 cases out of 374 at Gumi hospital, wound revision was performed for wound dehiscence. Patients at the Department of Obstetrics and Gy- necology were the most common and included 33 patients (39.8%). The most common intervention before wound revi- sion was Cesarean section in 14 patients (19.3%). In this study, we retrospectively reviewed patients who underwent wound revision due to wound dehiscence and analyzed the underlying causes of the postoperative complication. -
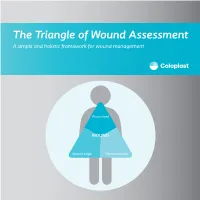
The Triangle of Wound Assessment a Simple and Holistic Framework for Wound Management
The Triangle of Wound Assessment A simple and holistic framework for wound management Wound bed WOUND Wound edge Periwound skin We asked healthcare professionals around the world about their priorities ? for wound care We found that most people Respondents said that treating wounds are not protecting the periwound specialists in a hospital1 skin is very important1 Approximately Up to 79% of wounds are 70% of being treated in wounds are the community2 surrounded by unhealthy skin3 2 ...none However, in a recent met all of the study of 14 wound criteria for assessment tools ... optimal wound assessment4 The Triangle of Wound Assessment is a holistic framework that allows practitioners üto assess and manage all areas of the wound, including the periwound skin. It is a simple and systematic approach that guides the user Wound bed from complete wound WOUND assessment to setting management goals, and Wound edge Periwound skin selecting the optimal treatment. 3 The Triangle of Wound Assessment offers a systematic approach to wound management Optimal wound management starts with a holistic wound assessment. This will help to more efficiently set management goals, which will increase the potential for better treatment outcomes. Assessment Management Goals Treatment 4 This is achieved through a holistic framework The Triangle of Wound Assessment provides a framework to assess all three areas of the wound while remembering the patient behind the wound within their social context. Patient Wound bed Social context WOUND Wound Wound edge Periwound skin 5 It’s not just about the wound but also the patient behind the wound Optimal management of the wound starts with assessing the patient behind the wound, and the social context in which the patient lives. -

Guideline: Wound Bed Preparation for Healable and Non Healable Wounds
British Columbia Provincial Nursing Skin and Wound Committee Guideline: Wound Bed Preparation for Healable and Non Healable Wounds Developed by the BC Provincial Nursing Skin and Wound Committee in collaboration with Wound Clinicians from: / TITLE Guideline: Wound Bed Preparation for Healable and Non-Healable Wounds in Adults & Children1 Practice Level Nurses in accordance with health authority and agency policy. Conservative sharp wound debridement (CSWD) is a restricted activity according to the Nurse’s (Registered) and Nurse Practitioner Regulation. 2 CRNBC states that registered nurses must successfully complete additional education and follow an established guideline when carrying out CSWD. Biological debridement therapy is a restricted activity according to the Nurse’s (Registered) and Nurse Practitioner Regulation. 3 CRNBC states that registered nurses must follow an established guideline when carrying out biological debridement. Clients 4 with wounds needing wound bed preparation require an interprofessional approach to provide comprehensive, evidence-based assessment and treatment. This clinical practice guideline focuses solely on the role of the nurse, as one member of the interprofessional team providing care to these clients. Background Factors affecting wound healability include the presence of adequate circulation in the area of the wound, wound related factors such as the size and duration of the wound, the ability to treat the cause of the wound and the presence of risk factors impacting wound healing. While many wounds heal, others are determined to be non-healing or slow-to-heal based on the presence or absence of these factors. Wound healability must be determined prior to debridement and moist wound healing. Although wound healing normally occurs in a predictable fashion, wound healing trajectories can be heterogeneous and non- uniform resulting is delayed wound healing for some clients. -

VII. Wound and Fracture Healing
Journal of Rehabilitation Research and Development Rehabilitation R & D Progress Reports 1986 VII. Wound and Fracture Healing VII . Wound and Fracture Healing Electrical Stimulation for Augmentation of Wound Healing Scott R. Crowgey, M.D., and Steven M. Sharpe Veterans Administration Research and Development, Decatur, GA 30033 Sponsor: VA Rehabilitation Research and Development Service Purpose—This project will attempt to identify ing that could be influenced by electrical stimu- aspects of the wound healing process that may lation. Efforts will then be directed toward de- be augmented by the exogenous influence of veloping mathematical models of the possible electromagnetic fields. A theoretical analysis of electrical interaction of electromagnetic fields the possible effects of electromagnetic fields on with cells and cell structures to determine how wound healing will include analyses of the these interactions could be optimized to im- interaction of electromagnetic fields with cellu- prove wound healing. It is anticipated that the lar structures and of the deposition of heat in literature will not contain all the information damaged tissue via exogenously applied energy necessary to develop these models . Any gaps in fields. This analysis will then be used as a basis necessary information and data will be filled, if for developing a plan for future investigations practical, using tissue phantom modeling mate- into the potential application of electrical stim- rials, blood, and possibly even primitive tissue ulation for the augmentation of wound healing. culture exposed to a variety of known electro- The initial research will involve a review of magnetic environments, using easily construct- the literature to identify aspects of wound heal- ed exposure chambers. -

3Rd Quarter 2001 Bulletin
In This Issue... Promoting Colorectal Cancer Screening Important Information and Documentaion on Promoting the Prevention of Colorectal Cancer ....................................................................................................... 9 Intestinal and Multi-Visceral Transplantation Coverage Guidelines and Requirements for Approval of Transplantation Facilities12 Expanded Coverage of Positron Emission Tomography Scans New HCPCS Codes and Coverage Guidelines Effective July 1, 2001 ..................... 14 Skilled Nursing Facility Consolidated Billing Clarification on HCPCS Coding Update and Part B Fee Schedule Services .......... 22 Final Medical Review Policies 29540, 33282, 67221, 70450, 76090, 76092, 82947, 86353, 93922, C1300, C1305, J0207, and J9293 ......................................................................................... 31 Outpatient Prospective Payment System Bulletin Devices Eligible for Transitional Pass-Through Payments, New Categories and Crosswalk C-codes to Be Used in Coding Devices Eligible for Transitional Pass-Through Payments ............................................................................................ 68 Features From the Medical Director 3 he Medicare A Bulletin Administrative 4 Tshould be shared with all General Information 5 health care practitioners and managerial members of the General Coverage 12 provider/supplier staff. Hospital Services 17 Publications issued after End Stage Renal Disease 19 October 1, 1997, are available at no-cost from our provider Skilled Nursing Facility -
Wound Care: the Basics
Wound Care: The Basics Suzann Williams-Rosenthal, RN, MSN, WOC, GNP Norma Branham, RN, MSN, WOC, GNP University of Virginia May, 2010 What Type of Wound is it? How long has it been there? Acute-generally heal in a couple weeks, but can become chronic: Surgical Trauma Chronic -do not heal by normal repair process-takes weeks to months: Vascular-venous stasis, arterial ulcers Pressure ulcers Diabetic foot ulcers (neuropathic) Chronic Wounds Pressure Ulcer Staging Where is it? Where is it located? Use anatomical location-heel, ankle, sacrum, coccyx, etc. Measurements-in centimeters Length X Width X Depth • Length = greatest length (head to toe) • Width = greatest width (side to side) • Depth = measure by marking the depth with a Q- Tip and then hold to a ruler Wound Characteristics: Describe by percentage of each type of tissue: Granulation tissue: • red, cobblestone appearance (healing, filling in) Necrotic: • Slough-yellow, tan dead tissue (devitalized) • Eschar-black/brown necrotic tissue, can be hard or soft Evaluating additional tissue damage: Undermining Separation of tissue from the surface under the edge of the wound • Describe by clock face with patients head at 12 (“undermining is 1 cm from 12 to 4 o’clock”) Tunneling Channel that runs from the wound edge through to other tissue • “tunneling at 9 o’clock, measuring 3 cm long” Wound Drainage and Odor Exudate Fluid from wound • Document the amount, type and odor • Light, moderate, heavy • Drainage can be clear, sanguineous (bloody), serosanguineous (blood-tinged), -

Risk Factors for Surgical Wound Dehiscence by Hazim Ibrahim DPM 1
! The Northern Ohio Foot and Ankle Journal Official Publication of the NOFA Foundation A Literature Review of Causes and Risk Factors for Surgical Wound Dehiscence by Hazim Ibrahim DPM 1 The Northern Ohio Foot and Ankle Journal 4(26): 1-5 Abstract: Postoperative wound healing plays a significant role in facilitating a patient’s recovery and rehabilitation. Surgical wound dehiscence (SWD) impacts mortality and morbidity rates and significantly contributes to prolonged hospital stays and associated psychosocial stressors on individuals and their families. Most common risk factors associated with SWD include obesity and wound infections, particularly in the case of orthopedic surgery. There is limited reporting of variables associated with SWD across other surgical domains and a lack of risk assessment tools. Furthermore, there was a lack of clarity in the definition of SWD in the literature. This review provides an overview of the available research and provides a basis for more rigorous analysis of factors that contribute to SWD. Key words: Dehiscence, wound infection, obesity This is an Open Access article distributed under the terms of the Creative Commons Attribution License. It permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ©The Northern Ohio Foot and Ankle Foundation Journal. (www.nofafoundation.org) 2016. All rights reserved. time. The third week after surgery the durability equals 20% of the initial strength, and after 6-12 Wound dehiscence is one of the most weeks it reaches 70-80% (1). Sutures placed during surgery allow the tissues the necessary time to regain common complications of surgical incision sites. -

Laparoscopic Surgery: a Cut Abov
Laparoscopic surgery: A cut abov 24 OR Nurse 2013 September www.ORNurseJournal.com Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. ve the rest? 2.5 ANCC CONTACT HOURS While laparoscopy continues to be the surgical technique of choice, there are complications, some fatal, you should know more about. By Ruth L. MacGregor, MBA, BSN, RN, RNFA, CNOR Since the 1990s, laparoscopic surgery has been the surgical technique of choice. There are many benefits for patients who undergo laparoscopic surgery com- pared with open surgical procedures, but it’s impor- tant to understand the complications that may occur, Sas with any surgical procedure. The OR nurse must be knowledgeable regarding the advantages and dis- advantages of laparoscopic surgery to properly antici- pate unintended complications and ensure patient safety and quality of outcomes. Definition of laparoscopy Laparoscopy is a surgical procedure that allows for visualization of the abdominal cavity through a small incision, typically through a trocar using a laparoscope that has a camera and a light source. The camera transmits the images via a computer system. The pic- ture is then displayed on one or more monitors for the surgeon, first assistant or resident, and OR staff to visu- alize.1 A trocar consists of a sheath or cannula and an obturator that has a three-sided pointed shaft that’s twisted to separate muscle to gain access to the surgical site. In laparoscopy, the trocar separates the muscle and fascia until it’s in the peritoneum. There’s an access port that allows the carbon dioxide to flow into the abdominal cavity, as well as the cannula portion that www.ORNurseJournal.com September OR Nurse 2013 25 Copyright © 2013 Lippincott Williams & Wilkins. -
Suturing with U-Technique Versus Un
Official Title of the Study: Suturing with U-Technique versus Un- Reapproximated wound Edges during removal of Closed Thoracostomy-tube drain - A single centre Open-label randomized prospective trial (SUTURE TRIAL) NCT NUMBER: Not Yet Assigned DATE OF DOCUMENT: January 16, 2019 1 STUDY SUMMARY Title: Suturing with U-Technique versus Un-Reapproximated wound Edges during removal of Closed Thoracostomy-tube drain - A single centre Open-label randomized prospective trial (SUTURE TRIAL) Background: Closed thoracostomy tube drainage or chest tube insertion is one of the most commonly performed procedures in thoracic surgery. There are several published evidence-based guidelines on safe performance of a chest tube insertion. However, there is absence of prospective controlled trials or systematic reviews indicating the safest technique of closing the wound created at the time of chest tube insertion and that best guarantees good wound and overall outcomes, post-chest tube removal. The use of a horizontal mattress non-absorbable suture or U- suture which is placed at the time of chest tube insertion and used to create a purse-string wound re-approximation at the time of tube removal has been an age-long and time-honored practice in most thoracic surgical settings. It has been established by a recent study that an occlusive adhesive-absorbent dressing can also be safely used to occlude the wound at the time of chest tube removal with good wound and overall outcomes though the study focused on tubes inserted during thoracic surgical operations. -

A Focus on the Triangle of Wound Assessment — Addressing the Gap Challenge and Identifying Suspected Biofilm in Clinical Practice
Clinical practice A focus on the Triangle of Wound Assessment — addressing the gap challenge and identifying suspected biofilm in clinical practice Authors: Wound assessment should be comprehensive, systematic and evidence- Caroline Dowsett, Terry Swanson and Tonny Karlsmark based (World Union of Wound Healing Societies [WUWHS], 2016a). The Triangle of Wound Assessment offers clinicians a framework to assess the patient and their wound, taking into consideration the wound bed, wound edge and periwound skin (Dowsett et al, 2015). The framework can be adapted to incorporate new developments and new challenges in wound care such as the ‘gap challenge’ and biofilm prevention and management. Using the framework can assist in determining the status of the wound bed and support clinical decision making to prevent problems associated with exudate pooling at the wound bed and the potential for biofilm formation. he Triangle of Wound Assessment This article will discuss how the Triangle of was established in 2014 and provides Wound Assessment identifies infection and T a systematic approach to wound biofilm, tackles the gap challenge, and how assessment and in setting management goals, this framework can be developed for new to guide optimal treatment choice (Dowsett et challenges in wound care. al, 2015), ensuring that the periwound skin is incorporated into the assessment. Periwound The importance of holistic assessment skin can be a significant problem in patients Wounds are a significant source of cost to with chronic wounds, with between 60–70% patients, as well as to the health economy. of wounds found to be surrounded by either Chronic wounds are often hard to heal problematic or unhealthy periwound skin resulting in a cycle of pain, anxiety and (Cartier et al, 2014).