Master Thesis Project and Is Described in the Next Section
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Artificial Intelligence, China, Russia, and the Global Order Technological, Political, Global, and Creative Perspectives
AIR UNIVERSITY LIBRARY AIR UNIVERSITY PRESS Artificial Intelligence, China, Russia, and the Global Order Technological, Political, Global, and Creative Perspectives Shazeda Ahmed (UC Berkeley), Natasha E. Bajema (NDU), Samuel Bendett (CNA), Benjamin Angel Chang (MIT), Rogier Creemers (Leiden University), Chris C. Demchak (Naval War College), Sarah W. Denton (George Mason University), Jeffrey Ding (Oxford), Samantha Hoffman (MERICS), Regina Joseph (Pytho LLC), Elsa Kania (Harvard), Jaclyn Kerr (LLNL), Lydia Kostopoulos (LKCYBER), James A. Lewis (CSIS), Martin Libicki (USNA), Herbert Lin (Stanford), Kacie Miura (MIT), Roger Morgus (New America), Rachel Esplin Odell (MIT), Eleonore Pauwels (United Nations University), Lora Saalman (EastWest Institute), Jennifer Snow (USSOCOM), Laura Steckman (MITRE), Valentin Weber (Oxford) Air University Press Muir S. Fairchild Research Information Center Maxwell Air Force Base, Alabama Opening remarks provided by: Library of Congress Cataloging-in- Publication Data Brig Gen Alexus Grynkewich (JS J39) Names: TBD. and Lawrence Freedman (King’s College, Title: Artificial Intelligence, China, Russia, and the Global Order : Techno- London) logical, Political, Global, and Creative Perspectives / Nicholas D. Wright. Editor: Other titles: TBD Nicholas D. Wright (Intelligent Biology) Description: TBD Identifiers: TBD Integration Editor: Subjects: TBD Mariah C. Yager (JS/J39/SMA/NSI) Classification: TBD LC record available at TBD AIR UNIVERSITY PRESS COLLABORATION TEAM Published by Air University Press in October -

Preprint Version Page 1 of 11 IAC-19,A5,3-B3.6,2,X52923
70th International Astronautical Congress (IAC), Washington D.C., United States, 21-25 October 2019. Copyright ©2019 by the International Astronautical Federation (IAF). All rights reserved. IAC-19,A5,3-B3.6,2,x52923 Deployment of the SOLEX Environment for Analog Space Telerobotics Validation Ralph Bayera*, Peter Schmausa, Martin Pfaua, Benedikt Pleintingera, Daniel Leidnera, Fabian Wapplera, Annika Maiera, Thomas Kruegerb, Neal Y. Liia a Institute of Robotics and Mechatronics, German Aerospace Center (DLR) Oberpfaffenhofen, 82234 Wessling, Germany, [email protected] b European Space Research and Technology Centre (ESTEC), European Space Agency (ESA), Keplerlaan 1, 2201 AZ Noordwijk, The Netherlands * Corresponding Author Abstract Lunar and planetary surface operations and eventual colonization are gaining increasing interest in the space community exemplified by ESA’s Lunar Village Initiative. Consequently, larger and more complex infrastructure would be necessary to support these endeavors. As the assembly, repair, and maintenance tasks grow in correspondence to the infrastructure, robotic teams can serve as viable solution to meeting these needs. In order to test and verify the robotic capabilities necessary for surface operations, analog proving grounds on earth should be designed to simulate surface assets that should be operated by the deployed robots. This paper presents DLR’s effort to develop one of such proving grounds: the SOLar farm EXperimental (SOLEX) environment, equipped with a wide array of assets expected in a surface habitat. First utilized for the METERON SUPVIS Justin space-to-ground telerobotic experiment in 2017-2018, it is continuously being further developed with the aim of supporting the validation and verification of different modalities of future space robotic operations. -

Emerging Technology and America's National Security.Indd
1 GOVERNANCE IN AN EMERGING NEW WORLD Convened by George P. Shultz with James Cunningham, David Fedor, and James Timbie 3 Table of Contents WINTER SERIES, ISSUE 319 Introduction ..........................................................................................................................................................................5 Emerging Technologies and National Security: Russia, NATO, & the European Theater Philip Breedlove and Margaret E. Kosal .................................................................................................................................................8 Technology Converges; Non-State Actors Benefi t T.X. Hammes ...............................................................................................................................................................................................40 Information: The New Pacifi c Coin of the Realm Gary Roughead, Emelia Spencer Probasco, and Ralph Semmel ................................................................................................ 50 Observations from the Roundtable James O. Ellis, Jr. and George P. Shultz ............................................................................................................................................. 62 GOVERNANCE IN AN EMERGING NEW WORLD Emerging Technology and America’s National Security A Letter from the Conveners Sharp changes are afoot throughout the globe. Demographics are shifting, technology is advancing at unprecedented rates, and these changes are being -

Russian Humanoid Robot Boards Space Station After Delay 27 August 2019, by Maxime Popov
Russian humanoid robot boards space station after delay 27 August 2019, by Maxime Popov The robot sat in the commander's seat of an unmanned Soyuz spaceship that blasted off Thursday from a Russian spaceport in southern Kazakhstan. "Let's go. Let's go," the robot was heard saying during the launch, repeating the phrase used by the first man in space, Yuri Gagarin. Soyuz capsules are normally manned on such trips, but this time no humans were travelling in order to test a new emergency rescue system. The ship was carrying scientific and medical equipment and components for the space station's The lifesize robot is due to stay on the International life-support system, as well as food, medicines and Space Station until September 7, learning to assist personal hygiene products for crew members, astronauts there Russia's Roscosmos space agency said. It was second time lucky on Tuesday as an unmanned spacecraft carrying Russia's first humanoid robot docked at the International Space Station following a failed attempt over the weekend. "Sorry for the delay. Got stuck in traffic. Am ready to carry on with work," the robot's Twitter account said in a jokey first tweet from space. Copying human movements and designed to help with high-risk tasks, the lifesize robot, Fedor, is due to stay on the ISS until September 7. Speaking to Russian cosmonauts on the ISS via a video link-up, President Vladimir Putin lavished The robot can be operated manually by ISS astronauts praise on them for the way they handled the glitch. -
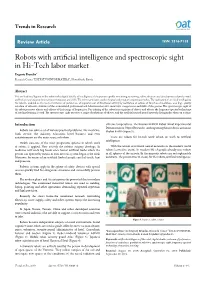
Robots with Artificial Intelligence and Spectroscopic Sight in Hi-Tech Labor Market Evgeniy Bryndin* Research Center "ESTESTVOINFORMATIKA", Novosibirsk, Russia
Trends in Research Review Article ISSN: 2516-7138 Robots with artificial intelligence and spectroscopic sight in Hi-Tech labor market Evgeniy Bryndin* Research Center "ESTESTVOINFORMATIKA", Novosibirsk, Russia Abstract The artificial intelligence of the robot is the digital double of intelligence of the person capable to training, retraining, self-realization and development of professional and behavioural creative innovative competences and skills. The robot represents a technological and program cognitive complex. The realization of artificial intelligence the robot is enabled on the basis of criterion of preferences of improvement of functional activity by realization of actions of function of usefulness and high-quality selection of extensive statistics of the accumulated professional and behavioural creative innovative competences and skills of the person. The spectroscopic sight of the robot perceives objects and objects of their range of frequencies. For training of the robot in recognition of objects and objects the frequency spectral technology of machine learning is used. The spectroscopic sight perceives a range of radiations of objects, and the artificial trained neural network distinguishes them on a range. Introduction extreme temperatures. The Russian FEDOR Robot (Final Experimental Demonstration Object Research)-anthropomorphous robot is astronaut Robots can solve a set of various practical problems. The medicine, Skybot F-850 (Figure5). bank service, the industry, education, hotel business and even entertainments are the main scopes of robots. There are robots for hi-tech work which on teeth to artificial intelligence. Health care-one of the most progressive spheres in which work of robots is applied. Now actively the robotic surgery develops. In With the advent of artificial neural networks in the modern world medicine will reach big break since bionic artificial limbs which the robots learned to create. -
The-Recitals-January-2020-Vajiram.Pdf
INDEX Message From The Desk Of Director 1 1. Feature Article 2-25 a. Budget 2020-21 b. India-Brazil Relation c. Blockchain Technology 2. Mains Q&A 26-49 3. Prelims Q&A 50-91 4. Bridging Gaps 92-132 1. Kolkata Port Renamed 2. National Start-up Advisory Council 3. State Energy Efficiency Index 2019 4. Guidelines To Check Illegal Sand Mining 5. Global Talent Competitiveness Index 6. Mission Purvodaya 7. Integrated Road Accident Database 8. 9. North East Gas Grid Project 10. Henley Passport Index 11. Andhra Pradesh Assembly Passes Bill For Three State Capitals 12. Crime In India Report 2018 13. Women, Business and Law 2020 14. Bru Agreement VAJIRAM AND RAVI The Recitals (January 2020) 15. Levels And Trends In Child Mortality Report 16. MHA Inaugurates Indian Cyber Crime Coordination Centre 17. Indian Data Relay Satellite System 18. Indian Science Congress 19. GSAT 30 Launched 20. Zo Kutpui 21. Nagoba Jatara 22. World Hindi Day 23. Ujjwala Inspires Ghana 24. India To Place Restrictions on Non-essential Imports 25. Hormuz Peace Initiative 26. First Session Of India-Norway Dialogue On Trade & Investment 27. 28. US Signs 'Phase One' Trade Deal with China 29. Myanmar-China Deal Under Belt and Road Initiative 30. Russian Government Resigns 31. Pakistan Nuclear Smuggling Activity Caught 32. Iran Fully Withdraws from Nuclear Deal 33. Nuclear-Capable K-4 Ballistic Missile 34. IAF Inducts Its First Squadron Of Sukhoi-30 MKI Aircraft 35. War Memorial in Nagaland for 357 Martyrs 36. Bodo Accord 2020 37. UP Government Introduces Police Commissionerate System 38. -

PRELIM SNIPPETS 23Rd AUGUST 2019 1. OP-BLUE
PRELIM SNIPPETS 23rd AUGUST 2019 1. OP-BLUE FREEDOM Context: Sports Minister Kiren Rijiju and former India football captain Baichung Bhutia flagged off the Delhi leg of Op-Blue Freedom. About Op-Blue Freedom: Op-Blue Freedom is a nation-wide adaptive scuba diving programme for people with disabilities as well as the able bodied. The program aims to train adventure enthusiasts in special forces skills like survival techniques, emergency first response skills, unarmed combat, endurance and fitness. 2. FEDOR ROBOT Context: Russia launched an unmanned rocket carrying a life-size humanoid robot named on the International Space Station. About FEDOR Robot: Name: Final Experimental Demonstration Object Research (FEDOR) It is the first ever robot sent by Russia to space. This life-size humanoid robot will spend 10 days learning to assist astronauts on the International Space Station. Fedor copies human movements, a key skill that allows it to remotely help astronauts or even people on Earth to carry out tasks while the humans are strapped into an exoskeleton. The Soyuz capsule was used to launch the rocket from the Russia-leased launch pad in Kazakhstan. Fedor is travelling in order to test a new emergency rescue system. Fedor, also known as Skybot F850 was strapped into a specially adapted pilot’s seat, with a small Russian flag in hand. Fedor is not the first robot to go into space. In 2011, NASA, sent up Robonaut 2, a humanoid robot developed with General Motors and a similar aim of working in high – risk environments. It was flown back to Earth in 2018 After experiencing technical problems. -
Disruptive Technologies
McKinsey Global Institute McKinsey Global Institute Disruptive technologies: Advances that will transform business, life, and the global economy May 2013 Disruptive technologies: Advances that will transform life, business, and the global economy The McKinsey Global Institute The McKinsey Global Institute (MGI), the business and economics research arm of McKinsey & Company, was established in 1990 to develop a deeper understanding of the evolving global economy. Our goal is to provide leaders in the commercial, public, and social sectors with the facts and insights on which to base management and policy decisions. MGI research combines the disciplines of economics and management, employing the analytical tools of economics with the insights of business leaders. Our “micro-to-macro” methodology examines microeconomic industry trends to better understand the broad macroeconomic forces affecting business strategy and public policy. MGI’s in-depth reports have covered more than 20 countries and 30 industries. Current research focuses on four themes: productivity and growth, the evolution of global financial markets, the economic impact of technology and innovation, and urbanization. Recent reports have assessed job creation, resource productivity, cities of the future, and the impact of the Internet. MGI is led by McKinsey & Company directors Richard Dobbs and James Manyika. Yougang Chen, Michael Chui, Susan Lund, and Jaana Remes serve as MGI principals. Project teams are led by a group of senior fellows and include consultants from McKinsey’s offices around the world. These teams draw on McKinsey’s global network of partners and industry and management experts. In addition, leading economists, including Nobel laureates, act as research advisers. -

Non-Signatories
NON-SIGNATORIES AFGHANISTAN Key developments since May 2001: Afghanistan has experienced dramatic political, military, and humanitarian changes. The cabinet approved Afghanistan’s accession to the Mine Ban Treaty on 29 July 2002 and the following day the Minister of Foreign Affairs signed the instrument of accession on behalf of the Transitional Islamic State of Afghanistan. Mine action operations were virtually brought to a halt following 11 September 2001. The mine action infrastructure suffered greatly during the subsequent military conflict, as some warring factions looted offices, seized vehicles and equipment, and assaulted local staff. Four deminers and two mine detection dogs were killed in errant U.S. air strikes. Military operations created additional threats to the population, especially unexploded U.S. cluster bomblets and ammunition scattered from storage depots hit by air strikes, as well as newly laid mines and booby-traps by Northern Alliance, Taliban, and Al-Qaeda fighters. A funding shortfall for the mine action program in Afghanistan prior to 11 September 2001 had threatened to again curtail mine action operations. But since October 2001, about $64 million has been pledged to mine action in Afghanistan. By March 2002, mine clearance, mine survey, and mine risk education operations had returned to earlier levels, and have since expanded beyond 2001 levels. In 2001, mine action NGOs surveyed approximately 14.7 million square meters of mined areas and 80.8 million square meters of former battlefield area, and cleared nearly 15.6 million square meters of mined area and 81.2 million square meters of former battlefields. Nearly 730,000 civilians received mine risk education. -

Iasbaba's 60 DAY PLAN 2021 SCIENCE & TECHNOLOGY
IASbaba’s 60 DAY PLAN 2021 UPSC SCIENCE & TECHNOLOGY [DAY 23] 2021 Q.1) It is a method of inquiry in artificial intelligence for determining whether a computer is capable of thinking like a human being or not. Which method is being referred here? a) Ebert Test b) ELIZA c) Feigenbaum test d) Turing Test Q.1) Solution (d) Basic Information: Statement 1: The Ebert test gauges whether a computer-based synthesized voice can tell a joke with sufficient skill to cause people to laugh. It was proposed by film critic Roger Ebert at the 2011 TED conference as a challenge to software developers to have a computerized voice master the inflections, delivery, timing, and intonations of a speaking human. Statement 2: ELIZA is an early natural language processing computer program created from 1964 to 1966 at the MIT Artificial Intelligence Laboratory by Joseph Weizenbaum. Created to demonstrate the superficiality of communication between humans and machines, Eliza simulated conversation by using a "pattern matching" and substitution methodology that gave users an illusion of understanding on the part of the program, but had no built in framework for contextualizing events. Statement 3: Feigenbaum test is also known as subject matter expert Turing test, here an computer system attempts to replicate an expert in a given field such as chemistry or marketing. it was proposed by Edward Feigenbaum in 2003. Statement 4: there are probabilities that very soon one might fail to distinguish between a robot and a human being. The form of robot that has reached this level can be tested through a method called ‘Turing Test’. -

Technologies Underlying Weapons of Mass Destruction
Technologies Underlying Weapons of Mass Destruction December 1993 OTA-BP-ISC-115 NTIS order #PB94-126984 GPO stock #052-003-01361-4 Recommended Citation: U.S. Congress, Office of Technology Assessment, Technologies Underlying Weapons of Mass Destruction, OTA-BP-ISC-115 (Washington, DC: U.S. Government Printing Office, December 1993). Foreword ontrolling the spread of weapons of mass destruction depends on how hard it is to manufacture them and on how easy such weapon programs are to detect. This background paper, a companion volume to OTA’s report Proliferation of Weapons of Mass Destruction: Assessing the Risks,cl reviews the technical requirements for countries to develop and build nuclear, chemical, and biological weapons, along with the systems most capable of delivering these weapons to distant or defended targets: ballistic missiles, combat aircraft, and cruise missiles. It identities evidence that might indicate the production of weapons of mass destruction, and technical hurdles that might provide opportunities to control their spread. Of the weapons considered here, nuclear weapons are the most difficult and expensive to develop-primarily due to the difficulty of producing the required nuclear materials. These materials, and the equipment needed to produce them, have quite limited civilian applications and are tightly controlled. States have produced nuclear weapon materials indigenously by evading international controls, but at great cost and with substantial opportunity for detection. For chemical and biological weapon materials, in contrast, most of the equipment needed also has civilian applications and has become widely available, making the capability to produce such weapons much more difficult to monitor and control. -

Supplementary Appendix This Appendix Formed Part of the Original Submission and Has Been Peer Reviewed
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: GlobalSurg Collaborative and National Institute for Health Research Global Health Research Unit on Global Surgery. Global variation in postoperative mortality and complications after cancer surgery: a multicentre, prospective cohort study in 82 countries. Lancet 2021; published online Jan 21. http://dx.doi.org/10.1016/ S0140-6736(21)00001-5. Online supplementary appendix Global variation in postoperative mortality and complications following cancer surgery: A multicentre, prospective cohort study in 82 countries GlobalSurg Collaborative and NIHR Global Health Research Unit on Global Surgery* * Investigators listed in online supplementary appendix. Table of Contents Supplementary tables and figures ....................................................................................................................................................... 2 Table S1. Patient and operative characteristics by country income group stratified by cancer type, including missing data. .......... 2 Figure S1. Missing values map. Missing values for main explanatory and dependent variables by observation. ............................. 3 Figure S2. Stage of presentation, 30-day mortality, and 30-day complications by cancer and country income group. .................... 4 Figure S3. Proportion of all patients who sustained specific complications, stratified by cancer-type and country income group. 5 Figure