Appendix =(Sigmoid Pelvis)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Jemds.Com Case Report
Jemds.com Case Report RIGHT SIDED SIGMOID COLON AND REDUNDANT DESCENDING COLON ON CONVENTIONAL AND CT IMAGING Mandeep Singh1, Madhan Kumar2, Daisy Gupta3 1Junior Resident, Department of Radiodiagnosis, Government Medical College, Amritsar, Punjab, India. 2Junior Resident, Department of Radiodiagnosis, Government Medical College, Amritsar, Punjab, India. 3Assistant Professor, Department of Radiodiagnosis, Government Medical College, Amritsar, Punjab, India. HOW TO CITE THIS ARTICLE: Singh M, Kumar M, Gupta D. Right sided sigmoid colon and redundant descending colon on conventional and CT imaging. J. Evolution Med. Dent. Sci. 2018;7(44):5617-5620, DOI: 10.14260/jemds/2018/1073 CASE PRESENTATION Investigations A 62-year-old male presented with history of severe On Plain X-Ray Abdomen constipation, abdominal distension, haemorrhoids and blood No abnormal air-fluid levels were seen. There were no in stool in surgical OPD of Guru Nanak Dev Hospital, abnormal radio-opaque shadows seen. Bilateral psoas Amritsar. The patient was referred for barium studies of shadows and soft tissue shadows were identified as normal. colon, which showed a loop of colon in pelvic region (at normal location of ileal loops) and redundant and long On Barium Enema descending colon extending across midline to reach hepatic After filling the rectum, the contrast was identified as filling flexure on right and continuing as sigmoid colon on right side. the sigmoid colon, which was present anomalously towards Transverse colon and ascending colon were normal in length the right side. Filling of barium outlined the extension of and position. On CECT abdomen of the patient, a long colon from sigmoid on right side with coiling in right iliac segment of descending colon was identified. -

The Herbivore Digestive System Buffalo Zebra
The Herbivore Digestive System Name__________________________ Buffalo Ruminant: The purpose of the digestion system is to ______________________________ _____________________________. Bacteria help because they can digest __________________, a sugar found in the cell walls of________________. Zebra Non- Ruminant: What is the name for the largest section of Organ Color Key a ruminant’s Mouth stomach? Esophagus __________ Stomach Small Intestine Cecum Large Intestine Background Information for the Teacher Two Strategies of Digestion in Hoofed Mammals Ruminant Non‐ruminant Representative species Buffalo, cows, sheep, goats, antelope, camels, Zebra, pigs, horses, asses, hippopotamus, rhinoceros giraffes, deer Does the animal Yes, regurgitation No regurgitation regurgitate its cud to Grass is better prepared for digestion, as grinding Bacteria can not completely digest cell walls as chew material again? motion forms small particles fit for bacteria. material passes quickly through, so stool is fibrous. Where in the system do At the beginning, in the rumen Near the end, in the cecum you find the bacteria This first chamber of its four‐part stomach is In this sac between the two intestines, bacteria digest that digest cellulose? large, and serves to store food between plant material, the products of which pass to the rumination and as site of digestion by bacteria. bloodstream. How would you Higher Nutrition Lower Nutrition compare the nutrition Reaps benefits of immediately absorbing the The digestive products made by the bacteria are obtained via digestion? products of bacterial digestion, such as sugars produced nearer the end of the line, after the small and vitamins, via the small intestine. intestine, the classic organ of nutrient absorption. -

Mouth Esophagus Stomach Rectum and Anus Large Intestine Small
1 Liver The liver produces bile, which aids in digestion of fats through a dissolving process known as emulsification. In this process, bile secreted into the small intestine 4 combines with large drops of liquid fat to form Healthy tiny molecular-sized spheres. Within these spheres (micelles), pancreatic enzymes can break down fat (triglycerides) into free fatty acids. Pancreas Digestion The pancreas not only regulates blood glucose 2 levels through production of insulin, but it also manufactures enzymes necessary to break complex The digestive system consists of a long tube (alimen- 5 carbohydrates down into simple sugars (sucrases), tary canal) that varies in shape and purpose as it winds proteins into individual amino acids (proteases), and its way through the body from the mouth to the anus fats into free fatty acids (lipase). These enzymes are (see diagram). The size and shape of the digestive tract secreted into the small intestine. varies in each individual (e.g., age, size, gender, and disease state). The upper part of the GI tract includes the mouth, throat (pharynx), esophagus, and stomach. The lower Gallbladder part includes the small intestine, large intestine, The gallbladder stores bile produced in the liver appendix, and rectum. While not part of the alimentary 6 and releases it into the duodenum in varying canal, the liver, pancreas, and gallbladder are all organs concentrations. that are vital to healthy digestion. 3 Small Intestine Mouth Within the small intestine, millions of tiny finger-like When food enters the mouth, chewing breaks it 4 protrusions called villi, which are covered in hair-like down and mixes it with saliva, thus beginning the first 5 protrusions called microvilli, aid in absorption of of many steps in the digestive process. -

Crohn's Disease of the Colon
Gut, 1968, 9, 164-176 Gut: first published as 10.1136/gut.9.2.164 on 1 April 1968. Downloaded from Crohn's disease of the colon V. J. McGOVERN AND S. J. M. GOULSTON From the Royal Prince Alfred Hospital, Sydney, Australia The fact that Crohn's disease may involve the colon never affected unless there had been surgical inter- either initially or in association with small bowel ference. There was no overt manifestation of mal- disease is now firmly established due largely to the absorption in any of these patients. evidence presented by Lockhart-Mummery and In 18 cases the colon alone was involved. Five had Morson (1960, 1964) and Marshak, Lindner, and universal involvement, five total involvement with Janowitz (1966). This entity is clearly distinct from sparing of the rectum, two involvement of the ulcerative colitis and other forms of colonic disease. descending colon only, two the transverse colon only, Our own experience with this disorder reveals many and in the other four there was variable involvement similarities with that published from the U.K. and of areas of large bowel (Fig. 2). the U.S.A. Thirty patients with Crohn's disease involving the large bowel were seen at the Royal CLINICAL FEATURES Prince Alfred Hospital during the last decade, the majority during the past five years. The criteria for The age incidence varied from 6 to 69 years when the inclusion were based on histological examination of patient was first seen, the majority being between the operative specimens in 28 and on clinical and radio- ages of 11 and 50. -

Epithelial Control of Gut-Associated Lymphoid Tissue Formation Through P38α-Dependent Restraint of NF-Κb Signaling
Epithelial Control of Gut-Associated Lymphoid Tissue Formation through p38 α -Dependent Restraint of NF-κB Signaling This information is current as Celia Caballero-Franco, Monica Guma, Min-Kyung Choo, of September 27, 2021. Yasuyo Sano, Thomas Enzler, Michael Karin, Atsushi Mizoguchi and Jin Mo Park J Immunol 2016; 196:2368-2376; Prepublished online 20 January 2016; doi: 10.4049/jimmunol.1501724 Downloaded from http://www.jimmunol.org/content/196/5/2368 Supplementary http://www.jimmunol.org/content/suppl/2016/01/19/jimmunol.150172 Material 4.DCSupplemental http://www.jimmunol.org/ References This article cites 53 articles, 20 of which you can access for free at: http://www.jimmunol.org/content/196/5/2368.full#ref-list-1 Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision by guest on September 27, 2021 • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2016 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Epithelial Control of Gut-Associated Lymphoid Tissue Formation through p38a-Dependent Restraint of NF-kB Signaling Celia Caballero-Franco,* Monica Guma,†,‡ Min-Kyung Choo,* Yasuyo Sano,* Thomas Enzler,*,x Michael Karin,†,{ Atsushi Mizoguchi,‖ and Jin Mo Park* The protein kinase p38a mediates cellular responses to environmental and endogenous cues that direct tissue homeostasis and immune responses. -

Vestibule Lingual Frenulum Tongue Hyoid Bone Trachea (A) Soft Palate
Mouth (oral cavity) Parotid gland Tongue Sublingual gland Salivary Submandibular glands gland Esophagus Pharynx Stomach Pancreas (Spleen) Liver Gallbladder Transverse colon Duodenum Descending colon Small Jejunum Ascending colon intestine Ileum Large Cecum intestine Sigmoid colon Rectum Appendix Anus Anal canal © 2018 Pearson Education, Inc. 1 Nasopharynx Hard palate Soft palate Oral cavity Uvula Lips (labia) Palatine tonsil Vestibule Lingual tonsil Oropharynx Lingual frenulum Epiglottis Tongue Laryngopharynx Hyoid bone Esophagus Trachea (a) © 2018 Pearson Education, Inc. 2 Upper lip Gingivae Hard palate (gums) Soft palate Uvula Palatine tonsil Oropharynx Tongue (b) © 2018 Pearson Education, Inc. 3 Nasopharynx Hard palate Soft palate Oral cavity Uvula Lips (labia) Palatine tonsil Vestibule Lingual tonsil Oropharynx Lingual frenulum Epiglottis Tongue Laryngopharynx Hyoid bone Esophagus Trachea (a) © 2018 Pearson Education, Inc. 4 Visceral peritoneum Intrinsic nerve plexuses • Myenteric nerve plexus • Submucosal nerve plexus Submucosal glands Mucosa • Surface epithelium • Lamina propria • Muscle layer Submucosa Muscularis externa • Longitudinal muscle layer • Circular muscle layer Serosa (visceral peritoneum) Nerve Gland in Lumen Artery mucosa Mesentery Vein Duct oF gland Lymphoid tissue outside alimentary canal © 2018 Pearson Education, Inc. 5 Diaphragm Falciform ligament Lesser Liver omentum Spleen Pancreas Gallbladder Stomach Duodenum Visceral peritoneum Transverse colon Greater omentum Mesenteries Parietal peritoneum Small intestine Peritoneal cavity Uterus Large intestine Cecum Rectum Anus Urinary bladder (a) (b) © 2018 Pearson Education, Inc. 6 Cardia Fundus Esophagus Muscularis Serosa externa • Longitudinal layer • Circular layer • Oblique layer Body Lesser Rugae curvature of Pylorus mucosa Greater curvature Duodenum Pyloric Pyloric sphincter antrum (a) (valve) © 2018 Pearson Education, Inc. 7 Fundus Body Rugae of mucosa Pyloric Pyloric (b) sphincter antrum © 2018 Pearson Education, Inc. -

Multiple Epithelia Are Required to Develop Teeth Deep Inside the Pharynx
Multiple epithelia are required to develop teeth deep inside the pharynx Veronika Oralováa,1, Joana Teixeira Rosaa,2, Daria Larionovaa, P. Eckhard Wittena, and Ann Huysseunea,3 aResearch Group Evolutionary Developmental Biology, Biology Department, Ghent University, B-9000 Ghent, Belgium Edited by Irma Thesleff, Institute of Biotechnology, University of Helsinki, Helsinki, Finland, and approved April 1, 2020 (received for review January 7, 2020) To explain the evolutionary origin of vertebrate teeth from closure of the gill slits (15). Consequently, previous studies have odontodes, it has been proposed that competent epithelium spread stressed the importance of gill slits for pharyngeal tooth formation into the oropharyngeal cavity via the mouth and other possible (12, 13). channels such as the gill slits [Huysseune et al., 2009, J. Anat. 214, Gill slits arise in areas where ectoderm meets endoderm. In 465–476]. Whether tooth formation deep inside the pharynx in ex- vertebrates, the endodermal epithelium of the developing pharynx tant vertebrates continues to require external epithelia has not produces a series of bilateral outpocketings, called pharyngeal been addressed so far. Using zebrafish we have previously demon- pouches, that eventually contact the skin ectoderm at corre- strated that cells derived from the periderm penetrate the oropha- sponding clefts (16). In primary aquatic osteichthyans, most ryngeal cavity via the mouth and via the endodermal pouches and pouch–cleft contacts eventually break through to create openings, connect to periderm-like cells that subsequently cover the entire or gill slits (17–19). In teleost fishes, such as the zebrafish, six endoderm-derived pharyngeal epithelium [Rosa et al., 2019, Sci. -

Sporadic (Nonhereditary) Colorectal Cancer: Introduction
Sporadic (Nonhereditary) Colorectal Cancer: Introduction Colorectal cancer affects about 5% of the population, with up to 150,000 new cases per year in the United States alone. Cancer of the large intestine accounts for 21% of all cancers in the US, ranking second only to lung cancer in mortality in both males and females. It is, however, one of the most potentially curable of gastrointestinal cancers. Colorectal cancer is detected through screening procedures or when the patient presents with symptoms. Screening is vital to prevention and should be a part of routine care for adults over the age of 50 who are at average risk. High-risk individuals (those with previous colon cancer , family history of colon cancer , inflammatory bowel disease, or history of colorectal polyps) require careful follow-up. There is great variability in the worldwide incidence and mortality rates. Industrialized nations appear to have the greatest risk while most developing nations have lower rates. Unfortunately, this incidence is on the increase. North America, Western Europe, Australia and New Zealand have high rates for colorectal neoplasms (Figure 2). Figure 1. Location of the colon in the body. Figure 2. Geographic distribution of sporadic colon cancer . Symptoms Colorectal cancer does not usually produce symptoms early in the disease process. Symptoms are dependent upon the site of the primary tumor. Cancers of the proximal colon tend to grow larger than those of the left colon and rectum before they produce symptoms. Abnormal vasculature and trauma from the fecal stream may result in bleeding as the tumor expands in the intestinal lumen. -

Immune Functions of the Vermiform Appendix
The Proceedings of the International Conference on Creationism Volume 3 Print Reference: Pages 335-342 Article 30 1994 Immune Functions of the Vermiform Appendix Frank Maas Follow this and additional works at: https://digitalcommons.cedarville.edu/icc_proceedings DigitalCommons@Cedarville provides a publication platform for fully open access journals, which means that all articles are available on the Internet to all users immediately upon publication. However, the opinions and sentiments expressed by the authors of articles published in our journals do not necessarily indicate the endorsement or reflect the views of DigitalCommons@Cedarville, the Centennial Library, or Cedarville University and its employees. The authors are solely responsible for the content of their work. Please address questions to [email protected]. Browse the contents of this volume of The Proceedings of the International Conference on Creationism. Recommended Citation Maas, Frank (1994) "Immune Functions of the Vermiform Appendix," The Proceedings of the International Conference on Creationism: Vol. 3 , Article 30. Available at: https://digitalcommons.cedarville.edu/icc_proceedings/vol3/iss1/30 IMMUNE FUNCTIONS OF THE VERMIFORM APPENDIX FRANK MAAS, M.S. 320 7TH STREET GERVAIS, OR 97026 KEYWORDS Mucosal immunology, gut-associated lymphoid tissues. immunocompetence, appendix (human and rabbit), appendectomy, neoplasm, vestigial organs. ABSTRACT The vermiform appendix Is purported to be the classic example of a vestigial organ, yet for nearly a century it has been known to be a specialized organ highly infiltrated with lymphoid tissue. This lymphoid tissue may help protect against local gut infections. As the vertebrate taxonomic scale increases, the lymphoid tissue of the large bowel tends to be concentrated In a specific region of the gut: the cecal apex or vermiform appendix. -
Appendicitis
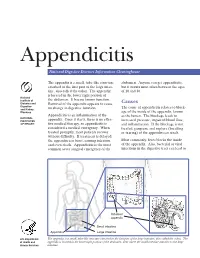
Appendicitis National Digestive Diseases Information Clearinghouse The appendix is a small, tube-like structure abdomen. Anyone can get appendicitis, attached to the first part of the large intes- but it occurs most often between the ages tine, also called the colon. The appendix of 10 and 30. is located in the lower right portion of National Institute of the abdomen. It has no known function. Diabetes and Removal of the appendix appears to cause Causes Digestive The cause of appendicitis relates to block- and Kidney no change in digestive function. Diseases age of the inside of the appendix, known Appendicitis is an inflammation of the as the lumen. The blockage leads to NATIONAL INSTITUTES appendix. Once it starts, there is no effec- increased pressure, impaired blood flow, OF HEALTH tive medical therapy, so appendicitis is and inflammation. If the blockage is not considered a medical emergency. When treated, gangrene and rupture (breaking treated promptly, most patients recover or tearing) of the appendix can result. without difficulty. If treatment is delayed, the appendix can burst, causing infection Most commonly, feces blocks the inside and even death. Appendicitis is the most of the appendix. Also, bacterial or viral common acute surgical emergency of the infections in the digestive tract can lead to Inflamed appendix Small intestine Appendix Large intestine U.S. Department The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The of Health and appendix is located in the lower right portion of the abdomen, near where the small intestine attaches to the large Human Services intestine. -

6-Physiology of Large Intestine.Pdf
LARGE INTESTINE COLON MOTILITY Color index • Important • Further explanation 1 Contents . Mind map.......................................................3 . Colon Function…………………………………4 . Physiology of Colon Regions……...…………6 . Absorption and Secretion…………………….8 . Types of motility………………………………..9 . Innervation and motility…………………….....11 . Defecation Reflex……………………………..13 . Fecal Incontinence……………………………15 Please check out this link before viewing the file to know if there are any additions/changes or corrections. The same link will be used for all of our work Physiology Edit 2 Mind map 3 COLON FUNCTIONS: Secretions of the Large Intestine: Mucus Secretion. • The mucosa of the large intestine has many crypts of 3 Colon consist of : Lieberkühn. • Absence of villi. • Ascending • Transverse • The epithelial cells contain almost no enzymes. • Descending • Presence of goblet cells that secrete mucus (provides an • Sigmoid adherent medium for holding fecal matter together). • Rectum • Anal canal • Stimulation of the pelvic nerves1 from the spinal cord can cause: Functions of the Large Intestine: o marked increase in mucus secretion. o This occurs along with increase in peristaltic motility 1. Reabsorb water and compact material of the colon. into feces. 2. Absorb vitamins produced by bacteria. • During extreme parasympathetic stimulation, so much 3. Store fecal matter prior to defecation. mucus can be secreted into the large intestine that the person has a bowel movement of ropy2 mucus as often as every 30 minutes; this mucus often contains little or no 1: considered a part of parasympathetic in large intestine . fecal material. 2: resembling a rope in being long, strong, and fibrous 3: anatomical division. 4 ILEOCECAL VALVE It prevents backflow of contents from colon into small intestine. -

Short Bowel Syndrome with Intestinal Failure Were Randomized to Teduglutide (0.05 Mg/Kg/Day) Or Placebo for 24 Weeks
Short Bowel (Gut) Syndrome LaTasha Henry February 25th, 2016 Learning Objectives • Define SBS • Normal function of small bowel • Clinical Manifestation and Diagnosis • Management • Updates Basic Definition • A malabsorption disorder caused by the surgical removal of the small intestine, or rarely it is due to the complete dysfunction of a large segment of bowel. • Most cases are acquired, although some children are born with a congenital short bowel. Intestinal Failure • SBS is the most common cause of intestinal failure, the state in which an individual’s GI function is inadequate to maintain his/her nutrient and hydration status w/o intravenous or enteral supplementation. • In addition to SBS, diseases or congenital defects that cause severe malabsorption, bowel obstruction, and dysmotility (eg, pseudo- obstruction) are causes of intestinal failure. Causes of SBS • surgical resection for Crohn’s disease • Malignancy • Radiation • vascular insufficiency • necrotizing enterocolitis (pediatric) • congenital intestinal anomalies such as atresias or gastroschisis (pediatric) Length as a Determinant of Intestinal Function • The length of the small intestine is an important determinant of intestinal function • Infant normal length is approximately 125 cm at the start of the third trimester of gestation and 250 cm at term • <75 cm are at risk for SBS • Adult normal length is approximately 400 cm • Adults with residual small intestine of less than 180 cm are at risk for developing SBS; those with less than 60 cm of small intestine (but with a