Reflux Esophagitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mouth Esophagus Stomach Rectum and Anus Large Intestine Small
1 Liver The liver produces bile, which aids in digestion of fats through a dissolving process known as emulsification. In this process, bile secreted into the small intestine 4 combines with large drops of liquid fat to form Healthy tiny molecular-sized spheres. Within these spheres (micelles), pancreatic enzymes can break down fat (triglycerides) into free fatty acids. Pancreas Digestion The pancreas not only regulates blood glucose 2 levels through production of insulin, but it also manufactures enzymes necessary to break complex The digestive system consists of a long tube (alimen- 5 carbohydrates down into simple sugars (sucrases), tary canal) that varies in shape and purpose as it winds proteins into individual amino acids (proteases), and its way through the body from the mouth to the anus fats into free fatty acids (lipase). These enzymes are (see diagram). The size and shape of the digestive tract secreted into the small intestine. varies in each individual (e.g., age, size, gender, and disease state). The upper part of the GI tract includes the mouth, throat (pharynx), esophagus, and stomach. The lower Gallbladder part includes the small intestine, large intestine, The gallbladder stores bile produced in the liver appendix, and rectum. While not part of the alimentary 6 and releases it into the duodenum in varying canal, the liver, pancreas, and gallbladder are all organs concentrations. that are vital to healthy digestion. 3 Small Intestine Mouth Within the small intestine, millions of tiny finger-like When food enters the mouth, chewing breaks it 4 protrusions called villi, which are covered in hair-like down and mixes it with saliva, thus beginning the first 5 protrusions called microvilli, aid in absorption of of many steps in the digestive process. -

Multiple Epithelia Are Required to Develop Teeth Deep Inside the Pharynx
Multiple epithelia are required to develop teeth deep inside the pharynx Veronika Oralováa,1, Joana Teixeira Rosaa,2, Daria Larionovaa, P. Eckhard Wittena, and Ann Huysseunea,3 aResearch Group Evolutionary Developmental Biology, Biology Department, Ghent University, B-9000 Ghent, Belgium Edited by Irma Thesleff, Institute of Biotechnology, University of Helsinki, Helsinki, Finland, and approved April 1, 2020 (received for review January 7, 2020) To explain the evolutionary origin of vertebrate teeth from closure of the gill slits (15). Consequently, previous studies have odontodes, it has been proposed that competent epithelium spread stressed the importance of gill slits for pharyngeal tooth formation into the oropharyngeal cavity via the mouth and other possible (12, 13). channels such as the gill slits [Huysseune et al., 2009, J. Anat. 214, Gill slits arise in areas where ectoderm meets endoderm. In 465–476]. Whether tooth formation deep inside the pharynx in ex- vertebrates, the endodermal epithelium of the developing pharynx tant vertebrates continues to require external epithelia has not produces a series of bilateral outpocketings, called pharyngeal been addressed so far. Using zebrafish we have previously demon- pouches, that eventually contact the skin ectoderm at corre- strated that cells derived from the periderm penetrate the oropha- sponding clefts (16). In primary aquatic osteichthyans, most ryngeal cavity via the mouth and via the endodermal pouches and pouch–cleft contacts eventually break through to create openings, connect to periderm-like cells that subsequently cover the entire or gill slits (17–19). In teleost fishes, such as the zebrafish, six endoderm-derived pharyngeal epithelium [Rosa et al., 2019, Sci. -

Traveler's Diarrhea
Traveler’s Diarrhea JOHNNIE YATES, M.D., CIWEC Clinic Travel Medicine Center, Kathmandu, Nepal Acute diarrhea affects millions of persons who travel to developing countries each year. Food and water contaminated with fecal matter are the main sources of infection. Bacteria such as enterotoxigenic Escherichia coli, enteroaggregative E. coli, Campylobacter, Salmonella, and Shigella are common causes of traveler’s diarrhea. Parasites and viruses are less common etiologies. Travel destination is the most significant risk factor for traveler’s diarrhea. The efficacy of pretravel counseling and dietary precautions in reducing the incidence of diarrhea is unproven. Empiric treatment of traveler’s diarrhea with antibiotics and loperamide is effective and often limits symptoms to one day. Rifaximin, a recently approved antibiotic, can be used for the treatment of traveler’s diarrhea in regions where noninvasive E. coli is the predominant pathogen. In areas where invasive organisms such as Campylobacter and Shigella are common, fluoroquinolones remain the drug of choice. Azithromycin is recommended in areas with qui- nolone-resistant Campylobacter and for the treatment of children and pregnant women. (Am Fam Physician 2005;71:2095-100, 2107-8. Copyright© 2005 American Academy of Family Physicians.) ILLUSTRATION BY SCOTT BODELL ▲ Patient Information: cute diarrhea is the most com- mised and those with lowered gastric acidity A handout on traveler’s mon illness among travelers. Up (e.g., patients taking histamine H block- diarrhea, written by the 2 author of this article, is to 55 percent of persons who ers or proton pump inhibitors) are more provided on page 2107. travel from developed countries susceptible to traveler’s diarrhea. -

Immune Functions of the Vermiform Appendix
The Proceedings of the International Conference on Creationism Volume 3 Print Reference: Pages 335-342 Article 30 1994 Immune Functions of the Vermiform Appendix Frank Maas Follow this and additional works at: https://digitalcommons.cedarville.edu/icc_proceedings DigitalCommons@Cedarville provides a publication platform for fully open access journals, which means that all articles are available on the Internet to all users immediately upon publication. However, the opinions and sentiments expressed by the authors of articles published in our journals do not necessarily indicate the endorsement or reflect the views of DigitalCommons@Cedarville, the Centennial Library, or Cedarville University and its employees. The authors are solely responsible for the content of their work. Please address questions to [email protected]. Browse the contents of this volume of The Proceedings of the International Conference on Creationism. Recommended Citation Maas, Frank (1994) "Immune Functions of the Vermiform Appendix," The Proceedings of the International Conference on Creationism: Vol. 3 , Article 30. Available at: https://digitalcommons.cedarville.edu/icc_proceedings/vol3/iss1/30 IMMUNE FUNCTIONS OF THE VERMIFORM APPENDIX FRANK MAAS, M.S. 320 7TH STREET GERVAIS, OR 97026 KEYWORDS Mucosal immunology, gut-associated lymphoid tissues. immunocompetence, appendix (human and rabbit), appendectomy, neoplasm, vestigial organs. ABSTRACT The vermiform appendix Is purported to be the classic example of a vestigial organ, yet for nearly a century it has been known to be a specialized organ highly infiltrated with lymphoid tissue. This lymphoid tissue may help protect against local gut infections. As the vertebrate taxonomic scale increases, the lymphoid tissue of the large bowel tends to be concentrated In a specific region of the gut: the cecal apex or vermiform appendix. -
Appendicitis
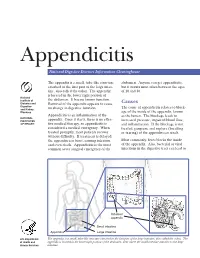
Appendicitis National Digestive Diseases Information Clearinghouse The appendix is a small, tube-like structure abdomen. Anyone can get appendicitis, attached to the first part of the large intes- but it occurs most often between the ages tine, also called the colon. The appendix of 10 and 30. is located in the lower right portion of National Institute of the abdomen. It has no known function. Diabetes and Removal of the appendix appears to cause Causes Digestive The cause of appendicitis relates to block- and Kidney no change in digestive function. Diseases age of the inside of the appendix, known Appendicitis is an inflammation of the as the lumen. The blockage leads to NATIONAL INSTITUTES appendix. Once it starts, there is no effec- increased pressure, impaired blood flow, OF HEALTH tive medical therapy, so appendicitis is and inflammation. If the blockage is not considered a medical emergency. When treated, gangrene and rupture (breaking treated promptly, most patients recover or tearing) of the appendix can result. without difficulty. If treatment is delayed, the appendix can burst, causing infection Most commonly, feces blocks the inside and even death. Appendicitis is the most of the appendix. Also, bacterial or viral common acute surgical emergency of the infections in the digestive tract can lead to Inflamed appendix Small intestine Appendix Large intestine U.S. Department The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The of Health and appendix is located in the lower right portion of the abdomen, near where the small intestine attaches to the large Human Services intestine. -

Appendix B: Muscles of the Speech Production Mechanism
Appendix B: Muscles of the Speech Production Mechanism I. MUSCLES OF RESPIRATION A. MUSCLES OF INHALATION (muscles that enlarge the thoracic cavity) 1. Diaphragm Attachments: The diaphragm originates in a number of places: the lower tip of the sternum; the first 3 or 4 lumbar vertebrae and the lower borders and inner surfaces of the cartilages of ribs 7 - 12. All fibers insert into a central tendon (aponeurosis of the diaphragm). Function: Contraction of the diaphragm draws the central tendon down and forward, which enlarges the thoracic cavity vertically. It can also elevate to some extent the lower ribs. The diaphragm separates the thoracic and the abdominal cavities. 2. External Intercostals Attachments: The external intercostals run from the lip on the lower border of each rib inferiorly and medially to the upper border of the rib immediately below. Function: These muscles may have several functions. They serve to strengthen the thoracic wall so that it doesn't bulge between the ribs. They provide a checking action to counteract relaxation pressure. Because of the direction of attachment of their fibers, the external intercostals can raise the thoracic cage for inhalation. 3. Pectoralis Major Attachments: This muscle attaches on the anterior surface of the medial half of the clavicle, the sternum and costal cartilages 1-6 or 7. All fibers come together and insert at the greater tubercle of the humerus. Function: Pectoralis major is primarily an abductor of the arm. It can, however, serve as a supplemental (or compensatory) muscle of inhalation, raising the rib cage and sternum. (In other words, breathing by raising and lowering the arms!) It is mentioned here chiefly because it is encountered in the dissection. -

Eosinophilic Enteritis, a Rare Dissease
Case Report Adv Res Gastroentero Hepatol Volume 16 Issue 1 - October 2020 DOI: 10.19080/ARGH.2020.16.555930 Copyright © All rights are reserved by Andy Gabriel Rivera Flores Eosinophilic Enteritis, A Rare Dissease Andy Rivera*, Roberto Délano, Jose de Jesús Herrera Esquivel and Carlos Valenzuela Salazar Endoscopy Unit, Hospital General, Manuel Gea González, México Submission: October 10, 2020; Published: October 22, 2020 *Corresponding author: Andy Gabriel Rivera Flores, Endoscopy Unit, Hospital General, Dr Manuel Gea González, México City, México Abstract Eosinophilic enteritis is a rare disease characterized by eosinophilic infiltration in the small intestine; In the absence of non-gastrointestinal diseasesKeywords: that cause eosinophilia or causes known as parasites, medications, or malignancies. Eosinophilic enteritis; Endoscopy; Treatment Introduction Eosinophilic enteritis is a rare disease characterized by physical examination revealed slight dryness of the mucosa, the rest without abnormalities. The results of the laboratory tests were eosinophilic infiltration of the small intestine; In the absence of within normal parameters (hematic biometry, 35-element blood non-gastrointestinal diseases that cause eosinophilia [1]. It was chemistry, general urinalysis, thyroid profile). A Simple Complete described in 1937 by Kaijser. The pathophysiology of this entity Abdominal Computerized Axial Tomography was performed with is not well described. The symptoms are manifested according oral and intravenous contrast, which demonstrated thickening of to the affected small intestine layer, the mucosa being the most the proximal small intestine that does not occlude the intestinal common (25-100%) characterized by weight loss, anemia, intestinal obstruction; Subserosa presents with eosinophilic lumen. Panendoscopy is performed where duodenal ulcers are positive stool guaiac; The Muscular (13-70%) presents data of observed in the first and second portion of the duodenum (Figure 1), taking biopsies of the duodenum and the Sydney protocol. -

Crohn's Disease (Regional Enteritis) of the Large Intestine and Its Distinction from Ulcerative Colitis by H
Gut: first published as 10.1136/gut.1.2.87 on 1 June 1960. Downloaded from Gut, 1960, 1, 87. CROHN'S DISEASE (REGIONAL ENTERITIS) OF THE LARGE INTESTINE AND ITS DISTINCTION FROM ULCERATIVE COLITIS BY H. E. LOCKHART-MUMMERY and B. C. MORSON From the Research Department, St. Mark's Hospital, London Twenty-five cases of Crohn's disease (regional enteritis) of the large intestine are described and illustrated. The clinical and pathological criteria for this diagnosis are discussed with emphasis on the distinction from ulcerative colitis. Suggestions are made regarding the surgical treatment of these patients. The pathogenesis of many of the inflammatory to have the same disease as that described by diseases of the large intestine is imperfectly under- Crohn, Ginzburg, and Oppenheimer in 1932. In stood and the literature contains many conflicting order to avoid further confusion we have preferred views, and so no classification has been generally to use the eponymous term "Crohn's disease of the accepted. Apart from specific diseases such as large intestine", because our patients had the same diverticulitis, bacillary dysentery, amoebic dysen- characteristic pathology in the large intestinal tery, and lymphogranuloma venereum, there re- lesions as that described by Hadfield (1939) for the http://gut.bmj.com/ mains to be considered a group of conditions which disease as it affects the small intestine. The fact have been given an abundant and confusing that Crohn's disease could affect the colon was first nomenclature. These include such expressions as mentioned by Colp in 1934 and noted by Crohn "regional colitis", "right-sided colitis", "segmental and Rosenak in 1936. -

Peptic Ulceration in Crohn's Disease (Regional Gut: First Published As 10.1136/Gut.11.12.998 on 1 December 1970
Gut, 1970, 11, 998-1000 Peptic ulceration in Crohn's disease (regional Gut: first published as 10.1136/gut.11.12.998 on 1 December 1970. Downloaded from enteritis) J. F. FIELDING AND W. T. COOKE From the Nutritional and Intestinal Unit, The General Hospital, Birmingham 4 SUMMARY The incidence of peptic ulceration in a personal series of 300 patients with Crohn's disease was 8%. Resection of 60 or more centimetres of the small intestine was associated with significantly increased acid output, both basally and following pentagastrin stimulation. Only five (4 %) of the 124 patients who received steroid therapy developed peptic ulceration. It is suggested that resection of the distal small bowel may be a factor in the probable increase of peptic ulceration in Crohn's disease. Peptic ulceration was observed in 4% of 600 1944 and 1969 for a mean period of 11-7 years patients with Crohn's disease by van Patter, with a mean duration of the disorder of 13.7 Bargen, Dockerty, Feldman, Mayo, and Waugh years. Fifty-one of these patients had Crohn's http://gut.bmj.com/ in 1954. Cooke (1955) stated that 11 of 90 patients colitis. Diagnosis in this series was based on with Crohn's disease had radiological evidence of macroscopic or histological criteria in 273 peptic ulceration whilst Chapin, Scudamore, patients, on clinical and radiological data in 25 Bagenstoss, and Bargen (1956) noted duodenal patients, and on clinical data together with minor ulceration in five of 39 (12.8%) successive radiological features in two patients with colonic patients with the disease who came to necropsy. -

Coeliac Disease Under a Microscope Histological Diagnostic Features And
Computers in Biology and Medicine 104 (2019) 335–338 Contents lists available at ScienceDirect Computers in Biology and Medicine journal homepage: www.elsevier.com/locate/compbiomed Coeliac disease under a microscope: Histological diagnostic features and confounding factors T ∗ Giulia Gibiinoa, , Loris Lopetusoa, Riccardo Riccib, Antonio Gasbarrinia, Giovanni Cammarotaa a Internal Medicine and, Gastroenterology and Hepatic Diseases Unit, IRCCS Fondazione Policlinico Universitario A. Gemelli, Università Cattolica del Sacro Cuore, Rome, Italy b Institute of Pathology, IRCCS Fondazione Policlinico Universitario A. Gemelli, Università Cattolica del Sacro Cuore, Rome, Italy ARTICLE INFO ABSTRACT Keywords: Coeliac disease (CD) and gluten-related disorders represent an important cornerstone of the daily practice of Gluten gastroenterologists, endoscopists and dedicated histopathologists. Despite the knowledge of clinical, serological Intraepithelial lymphocyte (IEL) and histological typical lesions, there are some conditions to consider for differential diagnosis. From the first Microscopic enteritis description of histology of CD, several studies were conducted to define similar findings suggestive for micro- Non-coeliac gluten-sensitivity scopic enteritis. Considering the establishment of early precursor lesions, the imbalance of gut microbiota is Gut microbiota another point still requiring a detailed definition. This review assesses the importance of a right overview in case of suspected gluten-related disorders and the several conditions mimicking -

Acute Gastroenteritis (AGE)
Acute Gastroenteritis (AGE) References: 1. Seattle Children’s Hospital, O’Callaghan J, Beardsley E, Black K, Drummond K, Foti J, Klee K, Leu MG, Ringer C. 2011 September. Acute Gastroenteritis (AGE) Pathway. 2. Diarrhoea and vomiting in children. Diarrhoea and vomiting caused by gastroenteritis: diagnosis, assessment and management in children younger than 5 years. National Collaborating Centre for Women's and Children's Health. http://www.ncbi.nlm.nih.gov/books/NBK63844/. Updated 2009. 3. National GC. Evidence-based care guideline for prevention and management of acute gastroenteritis (AGE) in children aged 2 months to 18 years. http://www.guideline.gov/content.aspx?id=35123&search=%22acute+gastroenteritis%22+and +(child*+or+pediatr*+or+paediatr*);. 4. Carter B, Fedorowicz Z. Antiemetic treatment for acute gastroenteritis in children: An updated cochrane systematic review with meta-analysis and mixed treatment comparison in a bayesian framework. BMJ Open. 2012;2(4). 5. National GC. Best evidence statement (BESt). Use of Lactobacillus rhamnosus GG in children with acute gastroenteritis. 6. Szajewska H, Skorka A, Ruszczynski M, Gieruszczak-Bialek D. Meta-analysis: Lactobacillus GG for treating acute gastroenteritis in children--updated analysis of randomised controlled trials. Aliment Pharmacol Ther. 2013;38(5):467-476. 7. Fedorowicz Z, Jagannath VA, Carter B. Antiemetics for reducing vomiting related to acute gastroenteritis in children and adolescents. Cochrane Database of Systematic Reviews. 2011;9. 8. Freedman SB, Ali S, Oleszczuk M, Gouin S, Hartling L. Treatment of acute gastroenteritis in children: An overview of systematic reviews of interventions commonly used in developed countries. Evid Based Child Health. 2013;8(4):1123-1137. -
Appendicitis US Protocol
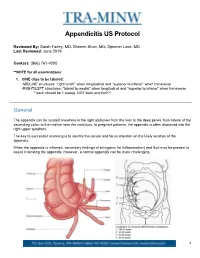
Appendicitis US Protocol Reviewed By: Sarah Farley, MD; Shireen Khan, MD; Spencer Lake, MD Last Reviewed: June 2019 Contact: (866) 761-4200 **NOTE for all examinations: 1. CINE clips to be labeled: -MIDLINE structures: “right to left” when longitudinal and “superior to inferior” when transverse -RIGHT/LEFT structures: “lateral to medial” when longitudinal and “superior to inferior” when transverse **each should be 1 sweep, NOT back and forth** General The appendix can be located anywhere in the right abdomen from the liver to the deep pelvis, from lateral of the ascending colon to the midline near the umbilicus. In pregnant patients, the appendix is often displaced into the right upper quadrant. The key to successful scanning is to identify the cecum and focus attention on the likely location of the appendix. When the appendix is inflamed, secondary findings of echogenic fat (inflammation) and fluid may be present to assist in locating the appendix. However, a normal appendix can be more challenging. 1 Strategies for finding the appendix include: 1. Review prior CT abdomen/pelvis or appendix US to see where appendix has been previously. 2. Scan in area of greatest pain (indicated by focal tenderness by 1 finger, not general pain). Label as such. 3. Localize cecum. 4. Localize ileocecal valve, if possible. Equipment: 1. Linear high frequency transducer is required, as this will best demonstrate anatomy of appendix. 2. In larger or obese patients, a curved lower frequency transducer may be used to obtain an overview and localize the cecum first. THEN, switch to the linear probe. a. When you locate the appendix, turn ON harmonics to better visualize the walls and appendiceal lumen together.