Large Vestibular Aqueduct and Congenital Sensorineural Hearing Loss
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Imaging of Nontraumatic Temporal Bone Emergencies Nitesh Shekhrajka, MD and Gul Moonis, MD
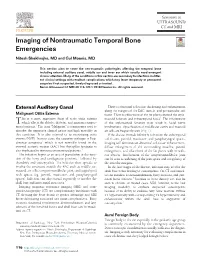
Imaging of Nontraumatic Temporal Bone Emergencies Nitesh Shekhrajka, MD and Gul Moonis, MD This section aims to cover the non-traumatic pathologies affecting the temporal bone including external auditory canal, middle ear and inner ear which usually need emergent clinical attention. Many of the conditions in this section are secondary to infections in differ- ent clinical settings with resultant complications which may leave temporary or permanent sequelae if not suspected, timely diagnosed or treated. Semin Ultrasound CT MRI 40:116-124 © 2018 Elsevier Inc. All rights reserved. External Auditory Canal There is abnormal soft tissue thickening and enhancement along the margins of the EAC, auricle, and periauricular soft Malignant Otitis Externa tissue. There is effacement of the fat planes around the stylo- his is a more aggressive form of acute otitis externa mastoid foramen and infratemporal fossa5. The involvement T which affects the elderly, diabetic, and immunocompro- of the stylomastoid foramen may result in facial nerve mised patients.1 The term “Malignant” is a misnomer used to involvement. Opacification of middle ear cavity and mastoid describe the aggressive clinical nature and high mortality in air cells are frequently seen (Fig. 1). this condition. It is also referred to as necrotizing otitis If the disease extends inferiorly to involve the subtemporal externa (NOE). In most cases, the causative pathogen is Pseu- soft tissues, parotid, masticator, and parapharyngeal spaces, domonas aeruginosa2 which is not normally found in the imaging will demonstrate abnormal soft tissue enhancement, external acoustic meatus (EAC) but Aspergillus fumigatus is diffuse enlargement of the surrounding muscles, parotid also implicated in immunocompromised patients.3 enlargement, and effacement of the fat planes with or with- The infection begins as an area of granulation at the junc- out abscess. -

Sound and the Ear Chapter 2
© Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION Chapter© Jones & Bartlett 2 Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION Sound and the Ear © Jones Karen &J. Kushla,Bartlett ScD, Learning, CCC-A, FAAA LLC © Jones & Bartlett Learning, LLC Lecturer NOT School FOR of SALE Communication OR DISTRIBUTION Disorders and Deafness NOT FOR SALE OR DISTRIBUTION Kean University © Jones & Bartlett Key Learning, Terms LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR Acceleration DISTRIBUTION Incus NOT FOR SALE OR Saccule DISTRIBUTION Acoustics Inertia Scala media Auditory labyrinth Inner hair cells Scala tympani Basilar membrane Linear scale Scala vestibuli Bel Logarithmic scale Semicircular canals Boyle’s law Malleus Sensorineural hearing loss Broca’s area © Jones & Bartlett Mass Learning, LLC Simple harmonic© Jones motion (SHM) & Bartlett Learning, LLC Brownian motion Membranous labyrinth Sound Cochlea NOT FOR SALE OR Mixed DISTRIBUTION hearing loss Stapedius muscleNOT FOR SALE OR DISTRIBUTION Compression Organ of Corti Stapes Condensation Osseous labyrinth Tectorial membrane Conductive hearing loss Ossicular chain Tensor tympani muscle Decibel (dB) Ossicles Tonotopic organization © Jones Decibel & hearing Bartlett level (dB Learning, HL) LLC Outer ear © Jones Transducer & Bartlett Learning, LLC Decibel sensation level (dB SL) Outer hair cells Traveling wave theory NOT Decibel FOR sound SALE pressure OR level DISTRIBUTION -

Direct Sagittal CT in the Evaluation of Temporal Bone Disease
371 Direct Sagittal CT in the Evaluation of Temporal Bone Disease 1 Mahmood F. Mafee The human temporal bone is an extremely complex structure. Direct axial and coronal Arvind Kumar2 CT sections are quite satisfactory for imaging the anatomy of the temporal bone; Christina N. Tahmoressi1 however, many relationships of the normal and pathologic anatomic detail of the Barry C. Levin2 temporal bone are better seen with direct sagittal CT sections. The sagittal projection Charles F. James1 is of interest to surgeons, as it has the advantage of following the plane of surgical approach. This article describes the advantages of using direct sagittal sections for Robert Kriz 1 1 studying various diseases of the temporal bone. The CT sections were obtained with Vlastimil Capek the aid of a new headholder added to our GE CT 9800 scanner. The direct sagittal projection was found to be extremely useful for evaluating diseases involving the vertical segment of the facial nerve canal, vestibular aqueduct, tegmen tympani, sigmoid sinus plate, sinodural angle, carotid canal, jugular fossa, external auditory canal, middle ear cavity, infra- and supra labyrinthine air cells, and temporo mandibular joint. CT has contributed greatly to an understanding of the complex anatomy and spatial relationship of the minute structures of the hearing and balance organs, which are packed into a small pyramid-shaped petrous temporal bone [1 , 2]. In the past 6 years, high-resolution CT scanning has been rapidly replacing standard tomography and has proved to be the diagnostic imaging method of choice for studying the normal and pathologic details of the temporal bone [3-14]. -

Vocabulario De Morfoloxía, Anatomía E Citoloxía Veterinaria
Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) Servizo de Normalización Lingüística Universidade de Santiago de Compostela COLECCIÓN VOCABULARIOS TEMÁTICOS N.º 4 SERVIZO DE NORMALIZACIÓN LINGÜÍSTICA Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) 2008 UNIVERSIDADE DE SANTIAGO DE COMPOSTELA VOCABULARIO de morfoloxía, anatomía e citoloxía veterinaria : (galego-español- inglés) / coordinador Xusto A. Rodríguez Río, Servizo de Normalización Lingüística ; autores Matilde Lombardero Fernández ... [et al.]. – Santiago de Compostela : Universidade de Santiago de Compostela, Servizo de Publicacións e Intercambio Científico, 2008. – 369 p. ; 21 cm. – (Vocabularios temáticos ; 4). - D.L. C 2458-2008. – ISBN 978-84-9887-018-3 1.Medicina �������������������������������������������������������������������������veterinaria-Diccionarios�������������������������������������������������. 2.Galego (Lingua)-Glosarios, vocabularios, etc. políglotas. I.Lombardero Fernández, Matilde. II.Rodríguez Rio, Xusto A. coord. III. Universidade de Santiago de Compostela. Servizo de Normalización Lingüística, coord. IV.Universidade de Santiago de Compostela. Servizo de Publicacións e Intercambio Científico, ed. V.Serie. 591.4(038)=699=60=20 Coordinador Xusto A. Rodríguez Río (Área de Terminoloxía. Servizo de Normalización Lingüística. Universidade de Santiago de Compostela) Autoras/res Matilde Lombardero Fernández (doutora en Veterinaria e profesora do Departamento de Anatomía e Produción Animal. -
Nervous System Week 5
NERVOUS SYSTEM WEEK 5 Doç. Dr. Yasemin SALGIRLI DEMİRBAŞ Neural Pathways in Sensory Systems • A single afferent neuron with all its receptor endings is a sensory unit. • a. Afferent neurons, which usually have more than one receptor of the same type, are the first neurons in sensory pathways. • b. The area of the body that, when stimulated, causes activity in a sensory unit or other neuron in the ascending pathway of that unit is called the receptive field for that neuron. Neural Pathways in Sensory Systems • Neurons in the specific ascending pathways convey information to specific primary receiving areas of the cerebral cortex about only a single type of stimulus. • Nonspecific ascending pathways convey information from more than one type of sensory unit to the brainstem, reticular formation and regions of the thalamus that are not part of the specific ascending pathways. Association Cortex and Perceptual Processing • Information from the primary sensory cortical areas is elaborated after it is relayed to a cortical association area. • The primary sensory cortical area and the region of association cortex closest to it process the information in fairly simple ways and serve basic sensory-related functions. • Regions of association cortex farther from the primary sensory areas process the sensory information in more complicated ways. • Processing in the association cortex includes input from areas of the brain serving other sensory modalities, arousal, attention, memory, language, and emotions. Comparison of General and Special Senses General Senses Special Senses • Include somatic sensations (tactile, • Include smell, taste, vision, hearing thermal, pain, and proprioceptive) and equilibrium. and visceral sensations. -

Bachmann.Pdf
Pediatric Vestibular Dysfunction: More Than a Balancing Act Kay Bachmann, PhD 1 2 Introduction Childhood Hearing Loss 1. The learner will be able to identify 3 causes of vestibular • 1.4 in 1,000 newborns have hearing loss (CDC) disorders in children. • 5 in 1,000 children have hearing loss ages 3-17 yrs (CDC) 2. The learner will be able to identify at least 3 common symptoms of vestibular dysfunction in children. 3. The learner will be able to administer a short screening to assess balance function in children. 3 4 1 Childhood Vestibular Loss • Balance disorders may make up .45% of chief complaints per chart review in a Pediatric ENT department. (O’Reilly et al 2010) • Children with hearing impairment are twice as likely to have vestibular loss than healthy children • Studies show vestibular loss in 30-79% of children with HL • There is 10% increase in vestibular loss as a result of trauma from receiving a CI (Jacot et al, 2009) 5 6 Common Disorders with Hearing Loss and Vestibular Abnormalities • Syndromes What Does a Typically Functioning Vestibular System Do? – Usher Syndrome Type 1 – Pendred Syndrome (also non syndromic Enlarged vestibular Aqueduct Syndrome) Two Main Reflexes: – Branchio-oto-renal Syndrome Vestibular Ocular Reflex- Helps hold an object – CHARGE association steady when the head/body are in motion. • Cochlear Malformations • VIII Nerve Defects • Cytomegalovirus (CMV) Vestibular Spinal Reflex- Helps keep our posture • Meningitis • Cochlear implant patients and body steady when it senses movement. 7 8 2 What Does an -

Entrapment Neuropathy of the Central Nervous System. Part II. Cranial
Entrapment neuropathy of the Cranial nerves central nervous system. Part II. Cranial nerves 1-IV, VI-VIII, XII HAROLD I. MAGOUN, D.O., F.A.A.O. Denver, Colorado This article, the second in a series, significance because of possible embarrassment considers specific examples of by adjacent structures in that area. The same entrapment neuropathy. It discusses entrapment can occur en route to their desti- nation. sources of malfunction of the olfactory nerves ranging from the The first cranial nerve relatively rare anosmia to the common The olfactory nerves (I) arise from the nasal chronic nasal drip. The frequency of mucosa and send about twenty central proces- ocular defects in the population today ses through the cribriform plate of the ethmoid bone to the inferior surface of the olfactory attests to the vulnerability of the optic bulb. They are concerned only with the sense nerves. Certain areas traversed by of smell. Many normal people have difficulty in each oculomotor nerve are pointed out identifying definite odors although they can as potential trouble spots. It is seen perceive them. This is not of real concern. The how the trochlear nerves are subject total loss of smell, or anosmia, is the significant to tension, pressure, or stress from abnormality. It may be due to a considerable variety of causes from arteriosclerosis to tu- trauma to various bony components morous growths but there is another cause of the skull. Finally, structural which is not usually considered. influences on the abducens, facial, The cribriform plate fits within the ethmoid acoustic, and hypoglossal nerves notch between the orbital plates of the frontal are explored. -

Mudr. Kaliariková Seminar for Medical Students 2019/20
MUDr. Kaliariková Seminar for medical students 2019/20 Deformity of shape, cosmetic defect Therapy: plastic correction – otoplasty: Children from the age of 6 years Congenital defect of auricle development (microtia) or missing auricle (anotia) is often combined with the congenital defect of the EAC (stenosis, atresia) Auditory canal stenosis means that it is narrower than 4 mm Dg: CT, objective hearing examination (exclusion of congenital defect of the middle and inner ear or the auditory track) Conductive hearing loss HRCT of the Temporal Bone Right side – stenosis of EAC Left side – atresia of EAC It depends on examination results and on hearing affliction extent (unilateral or bilateral affliction) Aim: provide communication Hearingaid devices (BAHA) Surgery: tympanoplasty, plastic of external auditory canal or auricle External opening is placed near the tragus and the inner opening between cartilaginous and bone part of the EAC Complication – inflammation (secretion, swelling or erythema) Th: Exstirpation, ATB (inflammation) Usually connected with atresia of EAC and anomalies of auricle Isolated / part of syndroms (more common, e.g. Treacher Collins) Usually unilateral Hearing-impairment Dg: CT, objective hearing examination Th: hearing-aid devices, tympanoplasty 20% of children with SNHL (sensorineural hearing loss) have CT anomalies of inner ear Cochlear anomalies Enlarged vestibular aqueduct (EVA) Semicircular canal dysplasia Michel deformity or complete labyrinthine aplasia (cochlea + vestibulum) Cochlear aplasia Common cavity malformation to the cochlea and vestibule Cochlear hypoplasia Cochlear incomplete partition type I (including cystic cochleovestibular anomaly) Cochlear incomplete partition type II (Mondini dysplasia) 1,5 screw of cochlea, dilated aqueductus Normal cochlea 2,5-2,75 screw Dilated vestibulum Normal vestibulum Ø 60% congenital • Damage of auditory organ during development (1. -

Fallen in a Dead Ear: Intralabyrinthine Preservation of Stapes in Fossil Artiodactyls Maeva Orliac, Guillaume Billet
Fallen in a dead ear: intralabyrinthine preservation of stapes in fossil artiodactyls Maeva Orliac, Guillaume Billet To cite this version: Maeva Orliac, Guillaume Billet. Fallen in a dead ear: intralabyrinthine preservation of stapes in fossil artiodactyls. Palaeovertebrata, 2016, 40 (1), 10.18563/pv.40.1.e3. hal-01897786 HAL Id: hal-01897786 https://hal.archives-ouvertes.fr/hal-01897786 Submitted on 17 Oct 2018 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/297725060 Fallen in a dead ear: intralabyrinthine preservation of stapes in fossil artiodactyls Article · March 2016 DOI: 10.18563/pv.40.1.e3 CITATIONS READS 2 254 2 authors: Maeva Orliac Guillaume Billet Université de Montpellier Muséum National d'Histoire Naturelle 76 PUBLICATIONS 745 CITATIONS 103 PUBLICATIONS 862 CITATIONS SEE PROFILE SEE PROFILE Some of the authors of this publication are also working on these related projects: The ear region of Artiodactyla View project Origin, evolution, and dynamics of Amazonian-Andean ecosystems View project All content following this page was uploaded by Maeva Orliac on 14 March 2016. -

CONGENITAL MALFORMATIONS of the INNER EAR Malformaciones Congénitas Del Oído Interno
topic review CONGENITAL MALFORMATIONS OF THE INNER EAR Malformaciones congénitas del oído interno. Revisión de tema Laura Vanessa Ramírez Pedroza1 Hernán Darío Cano Riaño2 Federico Guillermo Lubinus Badillo2 Summary Key words (MeSH) There are a great variety of congenital malformations that can affect the inner ear, Ear with a diversity of physiopathologies, involved altered structures and age of symptom Ear, inner onset. Therefore, it is important to know and identify these alterations opportunely Hearing loss Vestibule, labyrinth to lower the risks of all the complications, being of great importance, among others, Cochlea the alterations in language development and social interactions. Magnetic resonance imaging Resumen Existe una gran variedad de malformaciones congénitas que pueden afectar al Palabras clave (DeCS) oído interno, con distintas fisiopatologías, diferentes estructuras alteradas y edad Oído de aparición de los síntomas. Por lo anterior, es necesario conocer e identificar Oído interno dichas alteraciones, con el fin de actuar oportunamente y reducir el riesgo de las Pérdida auditiva Vestíbulo del laberinto complicaciones, entre otras —de gran importancia— las alteraciones en el área del Cóclea lenguaje y en el ámbito social. Imagen por resonancia magnética 1. Epidemiology • Hyperbilirubinemia Ear malformations occur in 1 in 10,000 or 20,000 • Respiratory distress from meconium aspiration cases (1). One in every 1,000 children has some degree • Craniofacial alterations (3) of sensorineural hearing impairment, with an average • Mechanical ventilation for more than five days age at diagnosis of 4.9 years. The prevalence of hearing • TORCH Syndrome (4) impairment in newborns with risk factors has been determined to be 9.52% (2). -

Cochlear Partition Anatomy and Motion in Humans Differ from The
Cochlear partition anatomy and motion in humans differ from the classic view of mammals Stefan Raufera,b,1, John J. Guinan Jra,b,c, and Hideko Heidi Nakajimaa,b,c aEaton-Peabody Laboratories, Massachusetts Eye and Ear, Boston, MA 02114; bSpeech and Hearing Bioscience and Technology Program, Harvard University, Cambridge, MA 02138; and cDepartment of Otolaryngology, Harvard Medical School, Boston, MA 02115 Edited by Christopher A. Shera, University of Southern California, Los Angeles, CA, and accepted by Editorial Board Member Thomas D. Albright June 6, 2019 (received for review January 16, 2019) Mammals detect sound through mechanosensitive cells of the assume there is no OSL motion (10–13). Additionally, the attach- cochlear organ of Corti that rest on the basilar membrane (BM). ment of the OSL to the BM and the attachment of the TM to Motions of the BM and organ of Corti have been studied at the spiral limbus (which sits above the OSL) are also consid- the cochlear base in various laboratory animals, and the assump- ered stationary. In contrast to this view, there have been reports tion has been that the cochleas of all mammals work similarly. of sound-induced OSL movement, but these reports have been In the classic view, the BM attaches to a stationary osseous spi- largely ignored in overviews of cochlear mechanics and the for- ral lamina (OSL), the tectorial membrane (TM) attaches to the mation of cochlear models (10–13). Von B´ek´esy (14), using static limbus above the stationary OSL, and the BM is the major mov- pressure, found that the CP “bent like an elastic rod that was free ing element, with a peak displacement near its center. -

ANATOMY of EAR Basic Ear Anatomy
ANATOMY OF EAR Basic Ear Anatomy • Expected outcomes • To understand the hearing mechanism • To be able to identify the structures of the ear Development of Ear 1. Pinna develops from 1st & 2nd Branchial arch (Hillocks of His). Starts at 6 Weeks & is complete by 20 weeks. 2. E.A.M. develops from dorsal end of 1st branchial arch starting at 6-8 weeks and is complete by 28 weeks. 3. Middle Ear development —Malleus & Incus develop between 6-8 weeks from 1st & 2nd branchial arch. Branchial arches & Development of Ear Dev. contd---- • T.M at 28 weeks from all 3 germinal layers . • Foot plate of stapes develops from otic capsule b/w 6- 8 weeks. • Inner ear develops from otic capsule starting at 5 weeks & is complete by 25 weeks. • Development of external/middle/inner ear is independent of each other. Development of ear External Ear • It consists of - Pinna and External auditory meatus. Pinna • It is made up of fibro elastic cartilage covered by skin and connected to the surrounding parts by ligaments and muscles. • Various landmarks on the pinna are helix, antihelix, lobule, tragus, concha, scaphoid fossa and triangular fossa • Pinna has two surfaces i.e. medial or cranial surface and a lateral surface . • Cymba concha lies between crus helix and crus antihelix. It is an important landmark for mastoid antrum. Anatomy of external ear • Landmarks of pinna Anatomy of external ear • Bat-Ear is the most common congenital anomaly of pinna in which antihelix has not developed and excessive conchal cartilage is present. • Corrections of Pinna defects are done at 6 years of age.