Gram-Negative Bacterial Toe Web Intertrigo
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Hyperhidrosis: Sweating out the Details
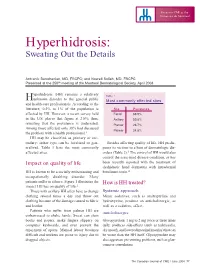
Focus on CME at the Université de Montréal Hyperhidrosis: Sweating Out the Details Antranik Benohanian, MD, FRCPC; and Nowell Solish, MD, FRCPC Presented at the 250th meeting of the Montreal Dermatological Society, April 2003 yperhidrosis (HH) remains a relatively Table 1 Hunknown disorder to the general public Most commonly affected sites and health-care professionals. According to the literature, 0.5% to 1% of the population is Site Prevalence affected by HH. However, a recent survey held Facial 68.9% in the U.S. places that figure at 2.8%; thus, Axillary 50.8% revealing that the prevalence is underrated. Plantar 28.7% Among those affected, only 38% had discussed Palmar 24.8% the problem with a health professional.1 HH may be classified as primary or sec- ondary; either type can be localized or gen- Besides affecting quality of life, HH predis- eralized. Table 1 lists the most commonly poses its victims to a host of dermatologic dis- affected sites. orders (Table 2).3 The control of HH would also control the associated disease condition, as has Impact on quality of life been recently reported with the treatment of dyshidrotic hand dermatitis with intradermal HH is known to be a socially embarrassing and botulinum toxin.4 occupationally disabling disorder. Many patients suffer in silence. Figure 1 illustrates the How is HH treated? impact HH has on quality of life.2 Those with axillary HH often have to change Systemic approach clothing several times a day and throw out Minor sedatives, such as amitriptyline and clothing because of the damage caused to fabric hydroxyzine, produce an anticholinergic, as and leather. -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -

“The Red Face” and More Clinical Pearls
“The Red Face” and More Clinical Pearls Courtney R. Schadt, MD, FAAD Assistant Professor Residency Program Director University of Louisville Associates in Dermatology I have no disclosures or conflicts of interest Part 1: The Red Face: Objectives • Distinguish and diagnose common eruptions of the face • Recognize those with potential implications for internal disease • Learn basic treatment options Which patient(s) has an increased risk of hypertension and hyperlipidemia? A B C Which patient(s) has an increased risk of hypertension and hyperlipidemia? A Seborrheic Dermatitis B C Psoriasis Seborrheic Dermatitis Goodheart HP. Goodheart's photoguide of common skin disorders, 2nd ed, Lippincott Williams & Wilkins, Philadelphia 2003. Copyright © 2003 Lippincott Williams & Wilkins. Seborrheic Dermatitis • Erythematous scaly eruption • Infants= “Cradle Cap” • Reappear in adolescence or later in life • Chronic, remissions and flares; worse with stress, cold weather • Occurs on areas of body with increased sebaceous glands • Unclear role of Malassezia; could be immune response; no evidence of overgrowth Seborrheic Dermatitis Severe Seb Derm: THINK: • HIV (can also be more diffuse on trunk) • Parkinson’s (seb derm improves with L-dopa therapy) • Other neurologic disorders • Neuroleptic agents • Unclear etiology 5MinuteClinicalConsult Clinical Exam • Erythema/fine scale • Scalp • Ears • Nasolabial folds • Beard/hair bearing areas Goodheart HP. Goodheart's photoguide of common skin disorders, 2nd ed, Lippincott • Ill-defined Williams & Wilkins, Philadelphia -

Therapies for Common Cutaneous Fungal Infections
MedicineToday 2014; 15(6): 35-47 PEER REVIEWED FEATURE 2 CPD POINTS Therapies for common cutaneous fungal infections KENG-EE THAI MB BS(Hons), BMedSci(Hons), FACD Key points A practical approach to the diagnosis and treatment of common fungal • Fungal infection should infections of the skin and hair is provided. Topical antifungal therapies always be in the differential are effective and usually used as first-line therapy, with oral antifungals diagnosis of any scaly rash. being saved for recalcitrant infections. Treatment should be for several • Topical antifungal agents are typically adequate treatment weeks at least. for simple tinea. • Oral antifungal therapy may inea and yeast infections are among the dermatophytoses (tinea) and yeast infections be required for extensive most common diagnoses found in general and their differential diagnoses and treatments disease, fungal folliculitis and practice and dermatology. Although are then discussed (Table). tinea involving the face, hair- antifungal therapies are effective in these bearing areas, palms and T infections, an accurate diagnosis is required to ANTIFUNGAL THERAPIES soles. avoid misuse of these or other topical agents. Topical antifungal preparations are the most • Tinea should be suspected if Furthermore, subsequent active prevention is commonly prescribed agents for dermatomy- there is unilateral hand just as important as the initial treatment of the coses, with systemic agents being used for dermatitis and rash on both fungal infection. complex, widespread tinea or when topical agents feet – ‘one hand and two feet’ This article provides a practical approach fail for tinea or yeast infections. The pharmacol- involvement. to antifungal therapy for common fungal infec- ogy of the systemic agents is discussed first here. -

Or Moisture-Associated Skin Damage, Due to Perspiration: Expert Consensus on Best Practice
A Practical Approach to the Prevention and Management of Intertrigo, or Moisture-associated Skin Damage, due to Perspiration: Expert Consensus on Best Practice Consensus panel R. Gary Sibbald MD Professor, Medicine and Public Health University of Toronto Toronto, ON Judith Kelley RN, BSN, CWON Henry Ford Hospital – Main Campus Detroit, MI Karen Lou Kennedy-Evans RN, FNP, APRN-BC KL Kennedy LLC Tucson, AZ Chantal Labrecque RN, BSN, MSN CliniConseil Inc. Montreal, QC Nicola Waters RN, MSc, PhD(c) Assistant Professor, Nursing Mount Royal University A supplement of Calgary, AB The development of this consensus document has been supported by Coloplast. Editorial support was provided by Joanna Gorski of Prescriptum Health Care Communications Inc. This supplement is published by Wound Care Canada and is available at www.woundcarecanada.ca. All rights reserved. Contents may not be reproduced without written permission of the Canadian Association of Wound Care. © 2013. 2 Wound Care Canada – Supplement Volume 11, Number 2 · Fall 2013 Contents Introduction ................................................................... 4 Complications of Intertrigo ......................................11 Moisture-associated skin damage Secondary skin infection ...................................11 and intertrigo ................................................................. 4 Organisms in intertrigo ..............................11 Consensus Statements ................................................ 5 Specific types of infection .................................11 -

Diaper Dermatitis in Infant Skin: Causes and Mitigation
Diaper Dermatitis in Infant Skin: Causes and Mitigation Josh Gregorio, PhD, and Karien Rodriguez, PhD Introduction Classifications of Diaper Dermatitis Infants under the age of two, especially preterm neonates, are Diaper dermatitis can be classified as mild, moderate, or vulnerable to developing skin irritation in the diapered region. severe, and is dependent on skin involvement and the degree Overhydration or prolonged skin contact with urine and feces of inflammation (Figure 1). Characteristics of mild diaper can result in breakdown of the skin barrier (the protective outer dermatitis include shiny erythema with or without scales, layer of the skin), leading to irritation and the appearance of a whereas more severe cases have intense erythema, ulcerations, rash. This event is known as diaper rash or diaper dermatitis, and pustule and vesicle eruptions. general terms describing skin inflammation in the diaper region. A B Diaper dermatitis is among the most common skin disorders of infancy. It accounts for 10-20% of all skin disorders treated by pediatricians and the highest incidence occurs in children between 9 and 12 months of age.1,2 If left untreated, progressive skin irritation in the diapered region can lead to secondary infections, including Candida albicans (candida dermatosis) and bacterial infections, that require additional treatment by a C D physician. Types of Diaper Dermatitis Although there are many types of diaper dermatoses (Table 1), most incidences arise from a nonallergic rash resulting from chemical, physical, or mechanical irritation called irritant contact dermatitis. Figure 1. Representative images of diaper dermatitis severity range: (A) healthy skin, (B) slight, (C) mild, (D) severe. -

Superficial Fungal Infections Faculty Version
Superficial Fungal Infections Pinar Oray-Schrom, MD Week 14 Educational Objectives: 1. Describe the different cutaneous infections associated with intertrigo 2. Review the differential diagnosis and treatment of tinea capitis 3. Understand the etiology and treatment of dandruff and seborrheic dermatitis Editor’s Note: Preceptors- As with any derm topic, a picture is worth a thousand words. You may want to have a color atlas of clinical dermatology handy (marked to the relevant pages) to pass around while you discuss the following cases. CASE ONE: A 55-year-old female presents to your office complaining of a rash underneath her breasts for the last two weeks. “I always have a mild rash in that area, since I sweat a lot. I use baby powder on a daily basis, but recently it has gotten very red and raw. It was itchy initially, but now it is more like a burning pain.” Her PMH includes morbid obesity with a BMI of 43 and IDDM. Your exam is significant for a maculopapular, intensely erythematous, sharply demarcated rash in both inframammary folds. Some areas appear macerated and you notice erythematous pustules and papules in the periphery of the rash. Your preceptor describes these as “satellite lesions.” Questions: 1. What is your diagnosis? Discuss the infectious and noninfectious causes of this condition. Your patient has intertrigo, which is a clinical description of an inflammatory skin reaction that occurs on opposing skin surfaces of body folds. It is primarily caused by skin on skin friction in areas that harbor moisture or have poor air circulation. Typical locations include the inner thighs, the inframammary region, axillae, skin folds of a pannus, the perineal area, the intergluteal cleft, and between toes and fingers. -

GRAM-NEGATIVE BACTERIAL TOE WEB INTERTRIGO *Laura Atzori, Myriam Zucca, Michela Lai, Monica Pau
GRAM-NEGATIVE BACTERIAL TOE WEB INTERTRIGO *Laura Atzori, Myriam Zucca, Michela Lai, Monica Pau Department of Dermatology, University of Cagliari, Cagliari, Italy *Correspondence to [email protected] Disclosure: No potential conflict of interest. Received: 28.04.14 Accepted: 22.08.14 Citation: EMJ Dermatol. 2014;2:106-111. ABSTRACT Gram-negative infection of the toe web space is less frequent than dermatophytes and yeasts, but it is more challenging, especially with the involvement of Pseudomonas aeruginosa in relation to antibiotic resistance and the increased risk of potentially lethal complications. Many conditions, other than infections, might initially present with the same clinical features, recognising the common initial damage (intertrigo), due to skin-on-skin rubbing in a moist environment with air entrapment, which is typical of interdigital spaces. Conditions such as contact eczema, atopic dermatitis, and inverse psoriasis, frequently predispose to, and are maintained by, the intertrigo, triggering a vicious circle. The dermatologist is in a lead position to address the correct assessment and management. A careful screening for predisposing factors is necessary: overweight, diabetic, but also athletes or people attending swimming pools, gyms, public showers/dressing rooms, and thermal baths are also at an increased risk of intertrigo of the toe web spaces. Occupational activities other than recreational might be relevant, such as the use of safety shoes or working in wet warm conditions. Incongruous therapy for tinea pedis or contact dermatitis, frequently auto-prescribed, might be among promoting factors altering the microbial ecosystem balance. The aim of this review is to evaluate the main epidemiologic and clinical features of Gram-negative bacteria intertrigo, the role of promoting factors, and the measures taken to treat and prevent this disorder. -

Derm World: a Journey Through a "Rash" of Clinical Presentations
Derm World: A Journey Through a "Rash" of Clinical Presentations Rob Danoff, DO, MS, FACOFP, FAAFP Derm World: + A Journey Through a “Rash” of Clinical Presentations Rob Danoff DO, MS, FACOFP, FAAFP OMED 2015 + Cutaneous findings in the Newborn Or, what is this? 1 + What is this? + Cutis Marmorata Mottling of skin Transient phenomena Vascular response to cold with immature nervous system Superficial small blood vessels in the skin dilating (red color) and contracting (pale color) at the same time May persist for months Re-warming usually restores the skin to its normal appearance Occurs in about 50% of infants Generally resolves with increasing age and of no significance for most infants 2 + In the Beginning Proof that babies are delivered by storks + What’s the Diagnosis? 3 + Nevus simplex = Stork bite= Salmon patch Red dilitation of blood vessels often on eyelid, face, or nape of neck (stork bite) They are usually small flat patches of pink or red skin with poorly defined borders These exanthems are very common and occur in over 40% of all newborns The facial patches are sometimes referred to as an “angel's kiss” and tend to fade over the first year of life + Nevus simplex = Stork bite= Salmon patch Often deepen in color with crying, straining with defecation, breath holding or with changes in ambient temperature Not painful or itchy Benign course, reassurance, lighten with age Those on the eyelids and below towards the nose usually disappear by 2 to 3 years of age Salmon patches are rarely detected after age 6 years -

A New Proposal for a Clinical-Oriented Subclassifi- Cation of Baboon Syndrome and a Review of Baboon Syndrome
Original article A new proposal for a clinical-oriented subclassifi- cation of baboon syndrome and a review of baboon syndrome Atsushi Miyahara1, 2, Hisashi Kawashima2, Yukari Okubo3 and Akinori Hoshika2 drug-related intertriginous and flexural exanthema Summary (SDRIFE), classical baboon syndrome, topical Objective: To review baboon syndrome (BS). drug-induced baboon syndrome, systemic drug- Data Sources: Date sources were obtained from induced baboon syndrome, recall phenomenon, p-i PubMed and Google Scholar: Photographs of (pharmacologic interaction with immuno-receptors) baboon syndrome were obtained from our concept. patient. Study Selections: PubMed and Google Scholar Introduction were searched up to June 30, 2010. The search The term “baboon syndrome”(BS) was terms were “baboon syndrome”, “SDRIFE” and introduced in 1984 to describe a mercury-induced “thimerosal allergy”. Reverse references from characteristic eruption with previous sensitization to relevant articles and Google Scholar were also mercury1. It presents with a diffuse symmetrical used. As BS is a classical disease and cases of erythema, predominantly on major flexural areas, offending agents were relatively old, some and an inverted triangular or V-shaped erythema on references were more than five years old. In both upper antero-medial thighs1. BS was named order to gather as many cases of offending agents after the red bottomed baboon1. as possible, more than 50 references were Recently it has been revealed that an eruption collected. which resembles mercury-induced BS was due not Results and Conclusion: We divided BS into as 4 only to mercury but also other metals, drugs and groups; classical baboon syndrome, topical drug- natural products, with or without previous induced baboon syndrome, systemic drug- sensitization to offending or related drug(s). -

Presenters: Philip R
UC Davis Dermatology Online Journal Title Zoledronic acid-associated symmetrical drug-related intertriginous and flexural exanthema (SDRIFE): report of baboon syndrome in a woman with recurrent metastatic breast cancer after receiving zoledronic acid Permalink https://escholarship.org/uc/item/5kk0g864 Journal Dermatology Online Journal, 21(8) Author Cohen, Philip R Publication Date 2015 DOI 10.5070/D3218028425 License https://creativecommons.org/licenses/by-nc-nd/4.0/ 4.0 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Volume 21 Number 8 August 2015 Case report Zoledronic acid-associated symmetrical drug-related intertriginous and flexural exanthema (SDRIFE): report of baboon syndrome in a woman with recurrent metastatic breast cancer after receiving zoledronic acid Philip R Cohen MD Dermatology Online Journal 21 (8): 2 Department of Dermatology, University of California San Diego, San Diego, California. Correspondence: Philip R. Cohen, MD 10991 Twinleaf Court San Diego, CA 92131-3643 [email protected] Abstract Background: Baboon syndrome is a distinctive skin reaction in which the patient typically develops erythematous buttocks that appear similar to those of a baboon. The non-contact allergenic variant of baboon syndrome is also referred to as symmetrical drug-related intertriginous and flexural exanthema (SDRIFE). Zoledronic acid is a bisphosphonate that is used in patients with metastatic cancer to prevent bone complications. Purpose: Zoledronic acid-associated baboon syndrome is described in a woman with recurrent metastatic breast cancer. Methods: PubMed was used to search the following terms, separately and in combination: baboon syndrome, breast cancer, symmetrical drug-related intertriginous and flexural exanthema, and zoledronic acid. -

Intertrigo of Streptococcal Aetiology: a Different Kind of Diaper Dermatitis Susana Castilho, Sofia Ferreira, Fabiana Fortunato, Sara Santos
Images in… BMJ Case Reports: first published as 10.1136/bcr-2018-224179 on 20 March 2018. Downloaded from Intertrigo of streptococcal aetiology: a different kind of diaper dermatitis Susana Castilho, Sofia Ferreira, Fabiana Fortunato, Sara Santos Department of Pediatrics, Centro DESCRIPTION Hospitalar do Oeste, Caldas da A 3-month-old infant presented with a 3-day history Rainha, Portugal of an intertriginous eruption. His previous history was irrelevant and his last vaccination was at 2 months old Correspondence to according to the Portuguese immunisation schedule. Dr Sofia Ferreira, sofia. su. ferreira@ gmail. com No other family members were affected and the child was otherwise well. Physical examination Accepted 1 March 2018 revealed an exuberant area of erythema and macer- ation of the inguinal folds and genitals (figures 1 and 2). This rash was bright red in colour and had well-de- fined borders. No satellite lesions were present. Bacterial culture of the affected region was obtained by a skin swab, and empirical treatment with oral flucloxacillin was started, admitting probable bacte- rial aetiology. The culture yielded a growth of group Figure 2 Intertriginous eruption on the third day after A beta-haemolytic streptococci sensitive to penicillin. initial appearance. Since the eruption had already started improving, treatment with flucloxacillin was continued with complete resolution of the intertrigo. differentiate it. Antibiotic therapy is generally cura- Intertrigo is an inflammatory dermatitis of the tive. Cutaneous group A