Aboriginal Health and Wellness Plan 2002/03 – 2005/06
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Annex 4.C.4 Terms of Reference for the IAMC for Trans Mountain Project TRANS MOUNTAIN INDIGENOUS ADVISORY and MONITORING COMMITTEE TERMS of REFERENCE
Annex 4.C.4 Terms of Reference for the IAMC for Trans Mountain Project TRANS MOUNTAIN INDIGENOUS ADVISORY AND MONITORING COMMITTEE TERMS OF REFERENCE DEFINITIONS 1. Defined terms in these Terms of Reference have the following meanings, which also include their singular and plural forms: “Committee” means the Trans Mountain Indigenous Advisory and Monitoring Committee established by these Terms of Reference as detailed in section 24, as may be amended from time to time; “Committee Members” means the Indigenous Caucus and the Government Committee Members; “CPCN” means the new Certificate of Public Convenience and Necessity, Instrument No. OC-064 issued to Kinder Morgan in relation to the Project on 1 December 2016; “DFO” means Fisheries and Oceans Canada; “Government” means the Government of Canada, including its departments and agencies; “Government Committee Members” are the representatives of federal government departments and agencies as contemplated by section 24(b); “Indigenous Caucus” means the members of the Committee appointed by the Indigenous Communities; “Indigenous Communities” are those Indigenous communities and groups to which the federal Crown determined it owes a duty to consult in relation to the Project, as set out in Appendix A; “Kinder Morgan” means Trans Mountain Pipeline ULC or the company that currently holds the CPCN, NEB Certificates of Public Convenience and Necessity OC-49 and OC-2 for the existing NEB-regulated Trans Mountain pipeline, together with all related Amending Orders, authorizations and exemptions -

Nicola Watershed Governance Project Indigenous Laws Research
Nicola Watershed Governance Project Indigenous Laws Research First Nations Fisheries Council of BC 2019 Annual General Assembly Memorandum of Understanding March 2018 the five Nicola Chiefs agreed to work collaboratively with the Province of British Columbia to co-lead a new approach to water stewardship throughout the Nicola watershed. This project is grounded in the commitment of these parties to implement the United Nations Declaration on the rights of Indigenous Peoples. (UNDRIP) Nicola Watershed Nicola Valley Two Nations: syilx and Nłeʔkepmx Five Bands Coldwater Indian Band Lower Nicola Indian Band Nooaitch Indian Band Shackan Indian Band Upper Nicola Indian Band Watershed Governance Staff Eva Tom, Indigenous Laws Research Liaison Jessica Dan, Indigenous Laws & Research Technician Crystal McMaster, Communications and Engagement Manager Nadia Joe, Nicola Forum Coordinator Alex Etchell, Project Associate Lee Failing, Facilitator and Strategic Advisor The Nicola Chiefs have commissioned the University of Victoria’s Indigenous Laws Research Unit to begin research into Nłeʔkepmx and syilx laws as they relate to water. University of Victoria Indigenous Laws Research Unit Team Dr. Val Napoleon, Director/Law Foundation Research Chair in Aboriginal Justice & Governance Dr. Rebecca Johnson, Associate Director Brooke Edmonds, ILRU Coordinator Jessica Asch, Research Director Simon Owen, Senior Researcher Lindsay Borrows, Tara Williamson, Researchers: Contact Information: Telephone: 250-721-8914 Email: [email protected] Website: www.uvic.ca/ilru Facebook: https://www.facebook.com/groups/indigenouslawresearchunit/ The Work Plan has five phase: 1. Planning and Building the Research Relationship o Refine goals of the project, research questions and resources 2. Knowledge Gathering Indigenous o Analyze narrative resources and draft overview material. -

2017-2018 Annual Report
COMMUNITY FUTURES SUN COUNTRY 2017 ANNUAL REPORT 2018 CELEBRATING MISSION STATEMENT To plan and initiate development of our area through promotion and facilitation of cooperative activities dedicated to the social, environmental and economic well-being of our citizens. Community Futures Sun Country TABLE OF CONTENTS Mission Statement Our Service Area Message from the Board Chair and General Manager ........................................... 1 About Community Futures Sun Country ................................................................ 2 Meet Our Team ..................................................................................................... 3 Board of Directors ............................................................................................ 3 Management and Finance ................................................................................ 8 Our Accomplishments ......................................................................................... 10 Strategic Priorities ............................................................................................... 11 Celebrating 30 Years ........................................................................................... 12 Loans Program ................................................................................................... 21 Community Economic Development ................................................................... 26 Wildfire Business Transition Project ......................................................................29 -

Nlaka'pamux Decision (2011)
COURT OF APPEAL FOR BRITISH COLUMBIA Citation: Nlaka’pamux Nation Tribal Council v. British Columbia (Environmental Assessment Office), 2011 BCCA 78 Date: 20110218 Docket: CA037570 Between: Nlaka’pamux Nation Tribal Council Appellant (Petitioner) 2011 BCCA 78 (CanLII) And Derek Griffin in his capacity as Project Assessment Director, Environmental Assessment Office, Belkorp Environmental Services Inc. and Village of Cache Creek Respondents (Respondents) Before: The Honourable Madam Justice Rowles The Honourable Madam Justice D. Smith The Honourable Mr. Justice Groberman On appeal from: the Supreme Court of British Columbia, September 17, 2009, (Nlaka’pamux Nation Tribal Council v. Griffin, 2009 BCSC 1275, Vancouver Registry No. S092162) Counsel for the Appellant: Reidar Mogerman Mark G. Underhill Counsel for the Respondent Griffin: Patrick G. Foy, QC Erin K. Christie Counsel for the Respondent Belkorp: Stephen M. Fitterman Place and Date of Hearing: Vancouver, British Columbia March 31, 2010 Place and Date of Judgment: Vancouver, British Columbia February 18, 2011 Written Reasons by: The Honourable Mr. Justice Groberman Nlaka’pamux Nation Tribal Council v. British Columbia (Environmental Assessment Office) Page 2 Concurred in by: The Honourable Madam Justice Rowles The Honourable Madam Justice D. Smith 2011 BCCA 78 (CanLII) Nlaka’pamux Nation Tribal Council v. British Columbia (Environmental Assessment Office) Page 3 Reasons for Judgment of the Honourable Mr. Justice Groberman: [1] This appeal arises out of a proposal to extend a landfill near Cache Creek by about 40 hectares. The landfill extension would occupy land over which the Nlaka’pamux First Nation claims Aboriginal rights and title. [2] The appellant (which I will refer to as the NNTC) is a tribal council incorporated in 1981. -
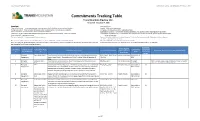
Commitments Tracking Table Trans Mountain Pipeline ULC Version 20 - December 7, 2018
Trans Mountain Expansion Project Commitment Tracking Table (Condition 6), December 7, 2018 Commitments Tracking Table Trans Mountain Pipeline ULC Version 20 - December 7, 2018 Project Stage Commitment Status "Prior to Construction" - To be completed prior to construction of specific facility or relevant section of pipeline "Scoping" - Work has not commenced "During Construction" - To be completed during construction of specific facility or relevant section of pipeline "In Progress - Work has commenced or is partially complete "Prior to Operations" - To be completed prior to commencing operations "Superseded by Condition" - Commitment has been superseded by NEB, BC EAO condition, legal/regulatory requirement "Operations" - To be completed after operations have commenced, including post-construction monitoring conditions "Superseded by Management Plan" - Addressed by Trans Mountain Policy or plans, procedures, documents developed for Project "Project Lifecycle" - Ongoing commitment design and execution "No Longer Applicable" - Change in project design or execution "Superseded by TMEP Notification Task Force Program" - Addressed by the project specific Notification Task Force Program "Complete" - Commitment has been met Note: Red text indicates a change in Commitment Status or a new Commitment, from the previously filed version. "No Longer Applicable" - Change in project design or execution Note: As of August 31, 2018, Kinder Morgan ceased to be an owner of Trans Mountain. References to Kinder Morgan Canada or KMC in the table below have -

Language List 2019
First Nations Languages in British Columbia – Revised June 2019 Family1 Language Name2 Other Names3 Dialects4 #5 Communities Where Spoken6 Anishnaabemowin Saulteau 7 1 Saulteau First Nations ALGONQUIAN 1. Anishinaabemowin Ojibway ~ Ojibwe Saulteau Plains Ojibway Blueberry River First Nations Fort Nelson First Nation 2. Nēhiyawēwin ᓀᐦᐃᔭᐍᐏᐣ Saulteau First Nations ALGONQUIAN Cree Nēhiyawēwin (Plains Cree) 1 West Moberly First Nations Plains Cree Many urban areas, especially Vancouver Cheslatta Carrier Nation Nak’albun-Dzinghubun/ Lheidli-T’enneh First Nation Stuart-Trembleur Lake Lhoosk’uz Dene Nation Lhtako Dene Nation (Tl’azt’en, Yekooche, Nadleh Whut’en First Nation Nak’azdli) Nak’azdli Whut’en ATHABASKAN- ᑕᗸᒡ NaZko First Nation Saik’uz First Nation Carrier 12 EYAK-TLINGIT or 3. Dakelh Fraser-Nechakoh Stellat’en First Nation 8 Taculli ~ Takulie NA-DENE (Cheslatta, Sdelakoh, Nadleh, Takla Lake First Nation Saik’uZ, Lheidli) Tl’azt’en Nation Ts’il KaZ Koh First Nation Ulkatcho First Nation Blackwater (Lhk’acho, Yekooche First Nation Lhoosk’uz, Ndazko, Lhtakoh) Urban areas, especially Prince George and Quesnel 1 Please see the appendix for definitions of family, language and dialect. 2 The “Language Names” are those used on First Peoples' Language Map of British Columbia (http://fp-maps.ca) and were compiled in consultation with First Nations communities. 3 The “Other Names” are names by which the language is known, today or in the past. Some of these names may no longer be in use and may not be considered acceptable by communities but it is useful to include them in order to assist with the location of language resources which may have used these alternate names. -

First Nations Health Authority Environmental Contaminants Program
First Nations Health Authority Environmental Contaminants Program GUIDELINES FOR PROPOSALS: A Guide for Health Professionals CONTENTS What is the First Nations Health Authority Environmental Contaminants Program? 1 Who can Apply? 2 Helpful Hints on Building Your Project 4 Project Funding 5 Eligible Projects 6 Review and Selection Process 8 Tools and Resources 12 Proposal Format 14 Example Budget 18 Application Checklist 20 Appendices 22 EXPLORING THE LINK BETWEEN HUMAN HEALTH AND ENVIRONMENTAL CONTAMINANTS GUIDELINES FOR PROPOSALS 3 o n m e i r n t a v F a m i l y l C n R o E e s m Wisdom p P m o h n u y mot s E io s n n C a i R i l b i HUMAN c e M t i S u BEING s y a l e L i n p l o t t a a l e y l n c t c t d S u p i i a r ritual a R l l el s ationship N a t i o n s E c o n o m i c ABOUT What is the BC First Nations a l Environmental Contaminants Program? t THE PROCESS e n S y o m i l L R a c n m om e n The First Nations Health Authority: Environmental Contaminants Program (ECP) supports First a s i Nations projects that explore the link between human health and environmental contaminants. It is d p d o F is e a intended to help First Nation communities in BC address their environmental health concerns and na c to support capacity development. -

Joint Federal/Provincial Consultation and Accommodation Report for the Trans Mountain Expension Project
Joint Federal/Provincial Consultation and Accommodation Report for the Trans Mountain Expansion Project November 2016 Joint Federal/Provincial Consultation and Accommodation Report for the TRANS MOUNTAIN EXPANSION PROJECT TABLE OF CONTENTS Acronyms, Abbreviations and Definitions Used in This Report ...................... xi 1. INTRODUCTION .......................................................................... 1 1.1 Purpose of the Report ..............................................................................1 1.2 Project Description .................................................................................2 1.3 Regulatory Review Including the Environmental Assessment Process .....................7 1.3.1 NEB REGULATORY REVIEW AND ENVIRONMENTAL ASSESSMENT PROCESS ....................7 1.3.2 BRITISH COLUMBIA’S ENVIRONMENTAL ASSESSMENT PROCESS ...............................8 1.4 NEB Recommendation Report.....................................................................9 2. APPROACH TO CONSULTING ABORIGINAL GROUPS ........................... 12 2.1 Identification of Aboriginal Groups ............................................................. 12 2.2 Information Sources .............................................................................. 19 2.3 Consultation With Aboriginal Groups ........................................................... 20 2.3.1 PRINCIPLES INVOLVED IN ESTABLISHING THE DEPTH OF DUTY TO CONSULT AND IDENTIFYING THE EXTENT OF ACCOMMODATION ........................................ 24 2.3.2 PRELIMINARY -

A GUIDE to Aboriginal Organizations and Services in British Columbia (December 2013)
A GUIDE TO Aboriginal Organizations and Services in British Columbia (December 2013) A GUIDE TO Aboriginal Organizations and Services in British Columbia (December 2013) INTRODUCTORY NOTE A Guide to Aboriginal Organizations and Services in British Columbia is a provincial listing of First Nation, Métis and Aboriginal organizations, communities and community services. The Guide is dependent upon voluntary inclusion and is not a comprehensive listing of all Aboriginal organizations in B.C., nor is it able to offer links to all the services that an organization may offer or that may be of interest to Aboriginal people. Publication of the Guide is coordinated by the Intergovernmental and Community Relations Branch of the Ministry of Aboriginal Relations and Reconciliation (MARR), to support streamlined access to information about Aboriginal programs and services and to support relationship-building with Aboriginal people and their communities. Information in the Guide is based upon data available at the time of publication. The Guide data is also in an Excel format and can be found by searching the DataBC catalogue at: http://www.data.gov.bc.ca. NOTE: While every reasonable effort is made to ensure the accuracy and validity of the information, we have been experiencing some technical challenges while updating the current database. Please contact us if you notice an error in your organization’s listing. We would like to thank you in advance for your patience and understanding as we work towards resolving these challenges. If there have been any changes to your organization’s contact information please send the details to: Intergovernmental and Community Relations Branch Ministry of Aboriginal Relations and Reconciliation PO Box 9100 Stn Prov. -

Dionisio Point Excavations
1HE• Publication of the Archaeological Society of Vol. 31 , No. I - 1999 Dionisio Point Excavations ARCHAEOLOGICAL SOCIETY OF &MIDDEN BRITISH COLUMBIA Published four times a year by the Archaeological Society of British Columbia Dedicated to the protection of archaeological resot:Jrces and the spread of archaeological knowledge. Editorial Committee Editor: Heather Myles (274-4294) President Field Editor: Richard Brolly (689-1678) Helmi Braches (462-8942) arcas@istar. ca [email protected] News Editor: Heather Myles Publications Editor: Robbin Chatan (215-1746) Membership [email protected] Sean Nugent (685-9592) Assistant Editors: Erin Strutt [email protected] erins@intergate. be.ca Fred Braches Annual membership includes I year's subscription to [email protected] The Midden and the ASBC newsletter, SocNotes. Production & Subscriptions: Fred Braches ( 462-8942) Membership Fees I SuBSCRIPTION is included with ASBC membership. Individual: $25 Family: $30 . Seniors/Students: $I 8 Non-members: $14.50 per year ($1 7.00 USA and overseas), Send cheque or money order payable to the ASBC to: payable in Canadian funds to the ASBC. Remit to: ASBC Memberships Midden Subscriptions, ASBC P.O. Box 520, Bentall Station P.O. Box 520, Bentall Station Vancouver BC V6C 2N3 Vancouver BC V6C 2N3 SuBMISSIONs: We welcome contributions on subjects germane ASBC on Internet to BC archaeology. Guidelines are available on request. Sub http://home.istar.ca/-glenchan/asbc/asbc.shtml missions and exchange publications should be directed to the appropriate editor at the ASBC address. Affiliated Chapters Copyright Nanaimo Contact: Rachael Sydenham Internet: http://www.geocities.com/rainforest/5433 Contents of The Midden are copyrighted by the ASBC. -

Nlaka'pamux Nation Tribal Council
Nlaka’pamux Nation Tribal Council - Province of British Columbia Political Accord on Advancing Recognition, Reconciliation, and Implementation of Title and Rights 1. The Nlaka’pamux Nation Tribal Council (NNTC) is a governing entity of the Nlaka’pamux peoples. The NNTC is committed to protecting, asserting and exercising Nlaka’pamux Title and Rights to bring about the self-sufficiency and well-being of the Nlaka’pamux people. The NNTC member communities are Boothroyd, Lytton, Boston Bar, Oregon Jack Creek, Skuppah, and Spuzzum. 2. The Province and the NNTC have entered into a number of agreements regarding the use of Nlaka’pamux territory that have been a foundation for collaborative relations. The agreements include: Interim Forestry Appendix/Agreement (2016) Economic and Community Development Agreement (ECDA) dealing with shared decision-making and revenue sharing in relation to the ongoing operations of the Highland Valley Copper Mine (2013) Land and Resource Shared Decision Making Pilot Agreement (2014, as amended) These agreements, and the relations they foster, have helped the Province and NNTC move through challenging conflicts, and establish a foundation for moving forward together on important decisions and actions. 3. The Land and Resource Shared Decision Making (SDM) Pilot Agreement established a foundational shared decision making model, and a joint Board structure. The SDM Board established a new way of co-operating between the Nlaka’pamux Nation and the Province. The Board structure and collaborative process moves away from individual and isolated assessments of potential impacts of any proposed project on Nlaka’pamux Title and Rights, to a shared and transparent process where there is equal accountability. -

LNIB Community Profile
Community Profile December 2015 Welcome! He’n’-le ! (Greetings!), On behalf of the Lower Nicola Indian Band (LNIB), I welcome you to our LNIB Community Profile. The purpose of the profile is to provide you with some essential information about LNIB. The profile highlights various topics, including an overview of who we are, our history, the programs that we deliver, the businesses that we are engaged with, our ancestral lands and Indian reserves, our administration, and our leadership and governance. LNIB is a vibrant community engaged in improving our lives, solidly grounded on the beliefs, traditions, and aspirations of our members. We are proud of who we are and what we have achieved, and we want to share our story with you. I hope that you will find the reading informative and enjoyable, and I thank you for the for the interest that you showed in learning more about us. Kwukwscmx, Humel, (Thank You!) Chief Aaron Sam Lower Nicola Indian Band 2 Vision Statement We, the people of the Lower Nicola Indian Band, commit ourselves to being a peaceful prosperous and secure community made up of healthy individuals rooted in the Nlaka’pamux culture, respecting ourselves, each other, the environment and all of Creation. We will honour and protect our children, the sacred gifts from the Creator, and our elders, the wisdom keepers. Together as one, we will take responsibility to regain control of our own destiny and rebuild our relationships with other people on a firm footing of respect and justice. We will possess our traditional territories and defend our hereditary and Aboriginal rights as Nlaka’pamux people, and promote the unity and strength of the Nlaka’pamux Nation as a whole.