Afya Uzazi Program
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

"Afrika-Studien" Edited by Ifo-Institut Für Wirtschafts- Forschung E
© Publication series "Afrika-Studien" edited by Ifo-Institut für Wirtschafts- forschung e. V., München, in connexion with Prof. Dr. PETER VON BLANCKENBURG, Berlin Prof. Dr. HEINRICH KRAUT, Dortmund Prof. Dr. OTTO NEULOH, Saarbriicken Prof. Dr. Dr. h. c. RUDOLP STUCKEN, Erlangen Prof. Dr. HANS WILBRANDT, Gottingen Prof. Dr. EMIL WOERMANN, Gottingen Editors in Cbief: Dr. phil. WILHELM MARQUARDT, München, Afrilca-Studienstelle im Ifo-Institut Prof. Dr. HANS RUTHENDERG, Stuttgart-Hohenheim, Institut für Auslandische Landwirtscliafl AFRIKA-STUDIENSTELLE MWEA An Irrigated Rice Settlement in Kenya Edited by ROBERT CHAMBERS and JON MORIS WELTFORUM VERLAG • MÜNCHEN M. The Perkerra Irrigation Scheme: A Contrasting Case by ROBERT CHAMBERS I. Historical Narrative 345 II. The Problems Experienced 352 1. Construction and Irrigation Problems 352 2. Production and Marketing Problems 353 3. Problems of Tenants and Staff 355 4. Problems of Organisation and Control 358 III. Some Concluding Lessons 361 List of Tables 1. Development Targets and Adiievements 349 2. Finance and Settlement 350 3. Onion Acreages and Yields 354 4. The Perkerra Local Committee 360 It is difficult to appreciate adequately a single development project con- sidered in isolation from its environment and from the record of similar projects elsewhere. To give a sharper focus to our review in this book of the achievements of the Mwea Irrigation Settlement, this chapter describes the very different history of effort and expenditure on a sister scheme whidi was started at the same time and for much the same reasons as Mwea. The Per- kerra Irrigation Scheme is located in the Rift Valley north of Nakuru (see Chapter A, Fig. -
RTJRC24.10 (Baringo GTI Hall, Kabarnet)
Seattle University School of Law Seattle University School of Law Digital Commons The Truth, Justice and Reconciliation I. Core TJRC Related Documents Commission of Kenya 10-24-2011 Public Hearing Transcripts - Rift Valley - Baringo - RTJRC24.10 (Baringo GTI Hall, Kabarnet) Truth, Justice, and Reconciliation Commission Follow this and additional works at: https://digitalcommons.law.seattleu.edu/tjrc-core Recommended Citation Truth, Justice, and Reconciliation Commission, "Public Hearing Transcripts - Rift Valley - Baringo - RTJRC24.10 (Baringo GTI Hall, Kabarnet)" (2011). I. Core TJRC Related Documents. 107. https://digitalcommons.law.seattleu.edu/tjrc-core/107 This Report is brought to you for free and open access by the The Truth, Justice and Reconciliation Commission of Kenya at Seattle University School of Law Digital Commons. It has been accepted for inclusion in I. Core TJRC Related Documents by an authorized administrator of Seattle University School of Law Digital Commons. For more information, please contact [email protected]. ORAL SUBMISSIONS MADE TO THE TRUTH, JUSTICE AND RECONCILIATION COMMISSION ON MONDAY, 24 TH OCTOBER, 2011 AT BARINGO GTI HALL, KABARNET PRESENT Tom Ojienda - The Presiding Chair, Kenya Ahmed Farah - Commissioner, Kenya Berhanu Dinka - Commissioner, Ethiopia Ronald Slye - Commissioner, USA Margaret Shava - Commissioner, Kenya Gertrude Chawatama - Commissioner, Zambia SECRETARIAT Patrick Njue - Leader of Evidence IN ATTENDANCE Dr. Samuel Tororei - Commissioner, KNCHR Rev. Lawrence Bomet - Commissioner, NCIC (Opening Prayers) (The Commission commenced at 10.05 a.m.) The Presiding Chair (Commissioner Ojienda): Thank you all once again. As part of the process, I want to specifically welcome the dancers from the Ilchamus community who are here to invite the Commission. -

Displacement Situation at Arabal Division and Sibilo Locations In
Displacement situation at Arabal Division and Sibilo Locations in Marigat and Baringo North Districts of Baringo County: - Kenya Initial Rapid Assessment Report Visited the affected areas (Arabal and Sibilo areas) on 22nd and 23rd January 2013 and triangulated it with Secondary Data from Kenya Red Cross Society and Government of Kenya officers CONTEXT: Brief description of the event and the location To undertake a multi-sector rapid assessment in line with the Kenya Initial Rapid Assessment (KIRA) process in areas hosting displaced communities Mission objectives To conduct a multi-sectoral rapid assessment following insecurity in Muchongoi division of Marigat district to identify gaps that need to be addressed in terms of humanitarian needs. Meet with GOK and Partners taking part in resolving issues surrounding the conflict in Marigat and Baringo north Districts Review sectoral issues of the IDP’s and host community and make recommendation on action to be taken Identify the reasons behind the displacement and highlight coping mechanisms of the community and their proposed solutions Mission dates 22nd and 23rd January 2013 Spatial coverage The mission will cover Marigat and Baringo north District the site of the recent cattle rustling incident that resulted in mass displacement of local population Mission team composition Paul Mutinda Kituku 0723 251828 [email protected] (Team leader) Lorraine Ombech 0728 602541 [email protected] Gabriel Wambua 0723 747676 [email protected] Stella Chumo 0722 475693 [email protected] Carlos, Based in Marigat 0721 929112 [email protected] Charlotte Mathysse 0732 436713 [email protected] Dr. S. Wanguru 0720 940577 [email protected] Faith Muriuki 0721 822232 [email protected] Joe Shields 0732 436716 Marigat District Background Information The larger Baringo county is divided into four administrative districts namely: Baringo Central, Baringo North, Marigat and East Pokot. -

Geothermal Potential of the Kenya Rift
Presented at Short Course III on Exploration for Geothermal Resources, organized by UNU-GTP and KenGen, at Lake Naivasha, Kenya, October 24 - November 17, 2008. GEOTHERMAL TRAINING PROGRAMME Kenya Electricity Generating Co., Ltd. STATUS OF GEOTHERMAL EXPLORATION IN KENYA AND FUTURE PLANS FOR ITS DEVELOPMENT Peter A. Omenda Kenya Electricity Generating Company Ltd. (KenGen) P.O. Box 785, Naivasha KENYA [email protected] ABSTRACT The high temperature geothermal prospects in Kenya are located within and are associated with the development of the Kenya Rift. Kenya Rift is a continental scale volcano-tectonic feature that stretches from northern to southern Africa. Development of the Rift started during the Oligocene (30million years ago) and activity has continued to recent times. The last 2 million years saw the development of large shield volcanoes within the axis of the rift. These centres are the most important geothermal prospects within the rift. Association between rifting and most of the occurrences of geothermal energy is mainly due to shallow magma chambers underneath the young volcanoes within the rift axis. KenGen in collaboration with the Ministry of Energy of the Government of Kenya has undertaken detailed surface studies of most of the prospects in the central sector of the rift which comprises Suswa, Longonot, Olkaria, Eburru, Menengai, Lakes Bogoria and Baringo, Korosi and Paka volcanic fields. Electric power is currently being generated at Olkaria with 130MWe installed while exploration drilling has been undertaken at Eburru and a 2.5MWe pilot plant is planned for development by KenGen and commissioning by 2009. Common methods that have been used by KenGen during exploration expeditions include geology (lithology, geochronology, structures); geophysics (seismic, gravity, magnetic, and resistivity); geochemistry (fluid and thermometry), heat flow and environmental baseline assessments. -

Geothermal Mapping Using Temperature Measurements
Presented at Short Course VII on Exploration for Geothermal Resources, organized by UNU-GTP, GDC and KenGen, at Lake Bogoria and Lake Naivasha, Kenya, Oct. 27 – Nov. 18, 2012. GEOTHERMAL TRAINING PROGRAMME Kenya Electricity Generating Co., Ltd. GEOTHERMAL MAPPING USING TEMPERATURE MEASUREMENTS Godwin M. Mwawongo Geothermal Development Company P. O. Box 100746, Nairobi 00101 KENYA [email protected] ABSTRACT Shallow temperature gradient holes are reliable in mapping geothermal prospects with heat loss features as surface manifestation. The sun least affects ground temperatures at 1 m depth and temperatures in the North rift are least affected by seasonal changes. Over 10,736 MWt is lost naturally from Menengai to Paka along the Kenyan rift. Most of the geothermal surface manifestations associated with the heat loss are oriented in the NW-SE with a few located in the NE-SW direction. Estimated down-hole temperature at I km depth is over 200oC. Fluid flow in the prospects from Lake Baringo to Paka is from East to West with an outflow to the north. 1. INTRODUCTION Kenya is located in East Africa where the Great African Rift virtually splits the landmass into two. 14 geothermal prospects have been identified within the Kenyan Rift Valley starting from Barrier in the north to Lake Magadi in the south with a potential of over 3,000 MWe (Figure 1). The rift is a graben and during the formation of the prospects, hot rocks were brought closer to the surface and with intensive faulting and presence of water, the geothermal systems were formed as shown in the model in Figure 2. -

Status of Geothermal Exploration in Kenya and Future Plans for Its Development
Presented at Short Course IV on Exploration for Geothermal Resources, organized by UNU-GTP, KenGen and GDC, at Lake Naivasha, Kenya, November 1-22, 2009. Kenya Electricity Generating Co., Ltd. GEOTHERMAL TRAINING PROGRAMME Geothermal Development Company STATUS OF GEOTHERMAL EXPLORATION IN KENYA AND FUTURE PLANS FOR ITS DEVELOPMENT Peter A. Omenda Geothermal Development Company P. O. Box 100746, Nairobi 00101 KENYA [email protected] ABSTRACT The high temperature geothermal prospects in Kenya are located within and are associated with the development of the Kenya Rift. Kenya Rift is a continental scale volcano-tectonic feature that stretches from northern to southern Africa. Development of the Rift started during the Oligocene (30million years ago) and activity has continued to recent times. The last 2 million years saw the development of large shield volcanoes within the axis of the rift. These centres are the most important geothermal prospects within the rift. Association between rifting and most of the occurrences of geothermal energy is mainly due to shallow magma chambers underneath the young volcanoes within the rift axis. KenGen in collaboration with the Ministry of Energy of the Government of Kenya has undertaken detailed surface studies of most of the prospects in the central sector of the rift which comprises Suswa, Longonot, Olkaria, Eburru, Menengai, Lakes Bogoria and Baringo, Korosi and Paka volcanic fields. Electric power is currently being generated at Olkaria with 130MWe installed while exploration drilling has been undertaken at Eburru and a 2.5MWe pilot plant is planned for development by KenGen and commissioning by 2009. Common methods that have been used by KenGen during exploration expeditions include geology (lithology, geochronology, structures); geophysics (seismic, gravity, magnetic, and resistivity); geochemistry (fluid and thermometry), heat flow and environmental baseline assessments. -

Kenya IDP Transit Sites, Rift Valley Province Molo, Uasin Gishu, Kwanza, Trans Nzoia West & Koibatek Districts
UN Office for the Coordination of Humanitarian Affairs, Kenya Kenya IDP Transit Sites, Rift Valley Province Molo, Uasin Gishu, Kwanza, Trans Nzoia West & Koibatek Districts Go-down: West Pokot Distrib.P.* SalamNa N Kenya Provinces GSUNKimondo N N Matumbee NNChepkoilel TobooN Gathata Geta Farm Kalaha N N Patwaka Trans Marakwet EASTERN N Nasianda Nzoia N Gatina Village RIFT VALLEY NORTH EASTERN N Gitwamba WESTERN N Kokwet N CENTRAL Mt. NYANZA Elgon NAIROBI Sirikwa N Moiben- Mafuta COAST N Moiben BenmNoi Farm !(Kimilili Ziwa Rayfarm machine Moiben Bungoma N N Baringo WESTERN Soy Soy TransitN!( Turbo Uasin !( Gishu Gilgil- Maili Tarigo Chepkanga Nne/Kambi N transit Thomas N N Kimumu Huruma N Transit N !(Eldoret Yamumbi Kipkaren Kabarnet N Keiyo !( Mkt RIFT !( Ndeffo N!(Marigat KasarinaN VALLEY Losuru Jasho & Kiamba MalelN NNOutspan Kaptagat Geticha Kihingo Lugaria !( N N Kabiyet Transit Kamwaura N !(Mkt Nyakinyua N Matunda Langwenda N N Beestone Grassland N Njokerio N N Kipkabus/waunifor N Kuresoi Sasumua Baringo BN Kio Farm Centre N Bindura N N Sosiot Usalama !(Kakamega Kimkaza Farm N N N (&Nyakinyua) Kakamega Rurigi N N Geti Cheptiret BF Town !( N NFarm Kamuyu Center Lessos BurnNt Ngarua Kapsabet !( Farm !( !( N FoNrNest Farm N N Nandi KondoN-N Kondo- 7 Farm Center NSDA N N & Bisaria Kio Farm BaptisNtNNPAG N Charismata Chavakali Kuresoi CeNnatnredi Molo !( Hills Baraka Police Rongai Koibatek !( N N Kapdening N Kahuho N Mbale Vihiga Matharu NVillage N !( Center !(Timboroa Eldama Majengo Usalama (&Nyakinyua) ravine !( Rurigi N NKangema BodeniN!( -

N014785CR.Pdf
á • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • 4I ID • List of Contents • GEOLOGY ID AVAILABILITY OF GROUNDWATER DATA ID GROUNDWATER • Springs ID Boreholes AQUIFER TYPES AND DESCRIFTIONS • • Weathered zone aquifers of the Kapasia Hills • Sedimentary deposits of the Kerio Valley and Baringo-Bogoria basin • • GROUNDWATER MOVEMEIVT GROUNDWATER RECHARGE • GROUNDWATER QUALITY • GROUNDWATER DEVELOPM ENT Present Borehole Abstraction • Development Potential: Weathered Zones • Sedimentary Deposits 41 • FURTHER INVESTIGATIONS • Exploratory Drilling Investigations ID • Appendix A Borehole Inventory for Baringo District • Pumping Test Results for Baringo District • B Chemical Analyses • • • • • • List of Figures Figure 1 Simplified Geological Map (1:128000) • 2 Borehole Location Map (1:128(10) • 3 Drilled Boreholes, 1930-81 • • List of Tables • Table 1 Distribution of Main Aquifer Types in Baringo District 2 Annual Direct Recharge 3 Annual Borehole Abstraction • • • • • • • • • • • • • • • • ID 4, • CEOLOGY 40 The project area forms part of the Kenya Rift Valley. Intense volcanic and tectonic activity, with intervening periods of erosion and sedimentation , has occurred in the area since the mid-Miocene. The geology of the area is extremely complex as a result and this is reflected by a wide range of • groundwater conditions. ID 40 Figure 1 shows the principal rock types and main structures. This • has been prepared from 1:125000 geological maps published by the Geological 1,2 Survey of Kenya and the East African Geological Research Unit of Lancaster ID 3 University . • The geology of the area can be divided into two broad types. Most of the area consists of volcanic rocks which consist predominantly of 40 phonolites, trachytes, basalts and tuffs. The sequence becomes progressively ID younger in age towards the main rift valley and also includes sedimentary • formations of generally alluvial or lacustrine origin. -

Impact of Introducing Reserve Flows on Abstractive Uses in Water Stressed Catchment in Kenya: Application of WEAP21 Model
International Journal of the Physical Sciences Vol. 5(16), pp. 2441-2449, 4 December, 2010 Available online at http://www.academicjournals.org/IJPS ISSN 1992 - 1950 ©2010 Academic Journals Full Length Research Paper Impact of introducing reserve flows on abstractive uses in water stressed Catchment in Kenya: Application of WEAP21 model Erick Mugatsia Akivaga1*, Fred A. O. Otieno1, E. C. Kipkorir2, Joel Kibiiy3 and Stanley Shitote3 1Durban University of Technology, P. O. Box 1334, Durban, 4000, South Africa. 2School of Environmetal Studies, Moi University, P. O. Box 3900-30100, Eldoret, Kenya. 3Department of Civil and Structural Engineering Moi University, P. O. Box 3900-30100, Eldoret, Kenya. Accepted 02 November 2010 Kenya is implementing Integrated Water Resources Management (IWRM) policies. The water policy provides for mandatory reserve (environmental flow) which should be sustained in a water resource. Four out of the six main catchments in Kenya face water scarcity. Further water resource quality objectives for many rivers are yet to be determined. This study applied Water Evaluation and Planning System (WEAP21) to study the implications of implementing the water reserve in Perkerra River which is among the few rivers that drain into Lake Baringo. The Tennant method was used to determine minimum environmental flows that should be sustained into the lake. WEAP21 was used to perform hydrological and water management analysis of the catchment. Mean monthly discharge time series of the catchment monitoring stations indicate that Perkerra River is becoming seasonal. The results further show that implementing the reserve with the present level of water management and development will increase the demand by more than 50%. -

Geology and Geothermal Resource Utilization Options in the Arus-Lake
Proceedings ARGeo 2 conference Entebbe, Uganda, 24-26 November 2008 Geology and Geothermal Resource Utilization Options in the Arus- Lake Bogoria Prospect, Northern Kenya Rift John Lagat, Kenya Electricity Generating Company Ltd, Olkaria Geothermal Project, P. O. Box 785, Naivasha 20117, Kenya [email protected] ABSTRACT area was carried to determine the potential and propose how best the resource could be Arus-Lake Bogoria geothermal prospect is utilized. located in the northern sector of the Kenyan Ethiopia Rift. Geothermal phenomena in form of a d n a a g i l U fumaroles, hot springs, steam jets, geysers, a KENYA L. Turkana m o sulphur deposits and high geothermal gradient S Nairobi expressed by anomalously hot ground and anomalous groundwater manifest the area. Tanzania Mombasa Detailed surface exploration surveys carried Barrier out in the prospect indicate presence of low to Namarunu 2oN intermediate temperature fracture controlled Emuruangogolak geothermal system(s) in the area. Silali Paka These low to medium enthalpy resources can Korosi be utilized in direct uses and electric power L. Baringo generation using binary-cycle power plants. L. Bogoria 0o The direct use applications that can be realized Nyanza Rift Menengai L. Nakuru in the area include tourism, spa pools, L. Elmenteita Eburru greenhouse heating, agricultural produce L. Naivasha Olkaria volcanic Longonot drying and industrial processes. The direct use complex application currently available in area is Suswa LEGEND tourism and a spa pool at one of the tourist Central volcanoes Lakes L. Magadi hotel. Advances in binary-cycle power and 2oS Faults submersible pump technologies have made L. -
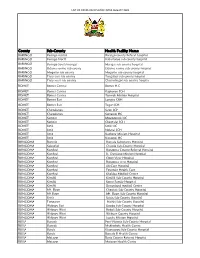
List of Covid-Vaccination Sites August 2021
LIST OF COVID-VACCINATION SITES AUGUST 2021 County Sub-County Health Facility Name BARINGO Baringo central Baringo county Referat hospital BARINGO Baringo North Kabartonjo sub county hospital BARINGO Baringo South/marigat Marigat sub county hospital BARINGO Eldama ravine sub county Eldama ravine sub county hospital BARINGO Mogotio sub county Mogotio sub county hospital BARINGO Tiaty east sub county Tangulbei sub county hospital BARINGO Tiaty west sub county Chemolingot sub county hospital BOMET Bomet Central Bomet H.C BOMET Bomet Central Kapkoros SCH BOMET Bomet Central Tenwek Mission Hospital BOMET Bomet East Longisa CRH BOMET Bomet East Tegat SCH BOMET Chepalungu Sigor SCH BOMET Chepalungu Siongiroi HC BOMET Konoin Mogogosiek HC BOMET Konoin Cheptalal SCH BOMET Sotik Sotik HC BOMET Sotik Ndanai SCH BOMET Sotik Kaplong Mission Hospital BOMET Sotik Kipsonoi HC BUNGOMA Bumula Bumula Subcounty Hospital BUNGOMA Kabuchai Chwele Sub-County Hospital BUNGOMA Kanduyi Bungoma County Referral Hospital BUNGOMA Kanduyi St. Damiano Mission Hospital BUNGOMA Kanduyi Elgon View Hospital BUNGOMA Kanduyi Bungoma west Hospital BUNGOMA Kanduyi LifeCare Hospital BUNGOMA Kanduyi Fountain Health Care BUNGOMA Kanduyi Khalaba Medical Centre BUNGOMA Kimilili Kimilili Sub-County Hospital BUNGOMA Kimilili Korry Family Hospital BUNGOMA Kimilili Dreamland medical Centre BUNGOMA Mt. Elgon Cheptais Sub-County Hospital BUNGOMA Mt.Elgon Mt. Elgon Sub-County Hospital BUNGOMA Sirisia Sirisia Sub-County Hospital BUNGOMA Tongaren Naitiri Sub-County Hospital BUNGOMA Webuye -

Factors Influencing Honey Production in Marigat, Baringo County - Kenya
International Journal of Research and Innovation in Social Science (IJRISS) |Volume III, Issue II, February 2019|ISSN 2454-6186 Factors Influencing Honey Production in Marigat, Baringo County - Kenya Chemwok C. K1*, Tuitoek D. K2 , Nganai S. K.2 1University of Eldoret, Kenya 2Moi University, Kenya *Corresponding Author Abstract:-Beekeeping is the maintenance of honey bee colonies in I. BACKGROUND INFORMATION hives. Beekeeping is a viable business that contributes income significantly to many rural households in Marigat, Baringo eekeeping is one of the more universal agricultural County. It provides a means of supplementary business and self B activity. Bees are found all over the world (Adjare, employment opportunities. Over the years, demand for honey 1990). Bees work a dual agricultural role by both producing continued to increase while quantity of honey produced declined. honey and aiding in the pollination of flowering crops. The study analyzed the effects of technological, economic, social Although much work has focused on improving the practice and institutional factors that influenced quantity of honey of beekeeping, it is still possible to manage beehives at a very produced. The theory of the firm was the theoretical framework low level of technological and capital input. Their of the study. The study adopted a survey design. The research cosmopolitan distribution, multipurpose nature and relative was conducted in Marigat, Baringo County with various regions being sampled to obtain reliable data. Target population of the simplicity in management combine to make bees a natural study was 1,500 bee farmers in the region and a sample size of agricultural supplement for many types of farm systems, 134 bee farmers were selected from three divisions.