New Detailed Description of the Anterior Part of the Cribriform Plate Using Anatomic Specimens and Computed Tomography
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
What Can I Learn from a Skull? Animal Skulls Have Evolved for Millions of Years to Protect Vertebrate’S Brains and Sensory Organs
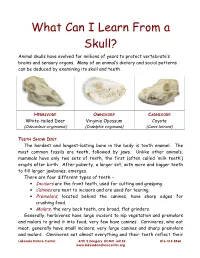
What Can I Learn From a Skull? Animal skulls have evolved for millions of years to protect vertebrate’s brains and sensory organs. Many of an animal’s dietary and social patterns can be deduced by examining its skull and teeth. HERBIVORE OMNIVORE CARNIVORE White-tailed Deer Virginia Opossum Coyote (Odocoileus virginianus) (Didelphis virginiana) (Canis latrans) TEETH SHOW DIET . The hardest and longest-lasting bone in the body is tooth enamel. The most common fossils are teeth, followed by jaws. Unlike other animals, mammals have only two sets of teeth, the first (often called ‘milk teeth’) erupts after birth. After puberty, a larger set, with more and bigger teeth to fill larger jawbones, emerges. There are four different types of teeth – • Incisors are the front teeth, used for cutting and grasping. • Canines are next to incisors and are used for tearing. • Premolars , located behind the canines, have sharp edges for crushing food. • Molars , the very back teeth, are broad, flat grinders. Generally, herbivores have large incisors to nip vegetation and premolars and molars to grind it into food; very few have canines. Carnivores, who eat meat, generally have small incisors, very large canines and sharp premolars and molars. Omnivores eat almost everything and their teeth reflect their Lakeside Nature Center 4701 E Gregory, KCMO 64132 816-513-8960 www.lakesidenaturecenter.org preferences; they have all four types of teeth. In fact, if you’d like to see an excellent example of an omnivore’s teeth, look in the mirror. EYE PLACEMENT IDENTIFIES PREDATORS . Carnivores generally have large eyes, placed so that the eyes look forward and the areas of vision of the two eyes overlap. -

Anatomic Variations of the Nose and Paranasal Sinuses in Saudi Population
234 Original article Anatomic variations of the nose and paranasal sinuses in saudi population: computed tomography scan analysis Nada Alshaikha, Amirah Aldhuraisb aDepartment of Otolaryngology Head & Neck Background Surgery, Rhinology Unit, Dammam Medical Knowledge of the anatomy constitutes an integral part in the total management of Complex (DMC), bDepartment of ENT, King Fahad Specialist Hospital (KFSH), Dammam, patients with sinonasal diseases. The aim of this study was to obtain the prevalence Saudi Arabia of sinonasal anatomic variations in Saudi population and to understand their importance and impact on the disease process, as well as their influence on Correspondence to Nada Alshaikh, MD, Department of Otorhinolaryngology Head and surgical management and outcome. Neck Surgery, Dammam Medical Complex, Materials and methods Dammam - 31414, Saudi Arabia This study is prospective review of retrospectively performed normal computed e-mail: [email protected] tomography (CT) scans of the nose and paranasal sinuses in adult Saudi Received 13 November 2016 population at Dammam Medical Complex. The scans were reviewed by two Accepted 23 December 2016 independent observers. The Egyptian Journal of Otolaryngology Results 2018, 34:234–241 Of all CT scans that were reviewed, 48.4% were of female patients and 51.6% were of male patients. The mean age of the study sample was 38.5±26.5 years. The most common anatomic variation after excluding agger nasi cell was pneumatized crista galli, which was seen in 73% of the scans. However, the least common variation seen in this series was hypoplasia of the maxillary sinus, which was encountered in 5% of the cases. We did not detect a single pneumatized inferior turbinate among the studied scans. -

Skeletal System
1 Name___________________________________ Date____________________________________ Laboratory Report Skeletal system: Axial skeleton and bony landmarks: Review each bone and landmark/s during lab. Skull- Cranial Bones: Frontal Bone supraorbital foramen frontal sinuses supraorbital margins glabella Parietal Bones sagittal suture coronal suture squamous suture lambdoid suture Temporal Bones zygomatic process mandibular fossa external auditory meatus mastoid process styloid process internal acoustic meatus carotid canal jugular foramen Occipital Bone: foramen magnum external occipital protuberance nuchal lines (superior and inferior) occipital condyle hypoglossal canal condylar canal Sphenoid: sella turcica tuberculum sellae dorsum sellae hypophyseal fossa greater wing lesser wing optic foramen superior orbital fissure pterygoid processes Foramen associated with the sphenoid: foramen ovale foramen lacerum* foramen rotundum foramen spinosum *found between sphenoid, temporal and occipital bones Ethmoid Bone: crista galli cribiform plate perpendicular plate cribiform/olfactory foramina superior nasal conchae/turbinates middle nasal conchae/turbinates 2 Skull- Facial Bones: Nasal Bones Palatine Bones Inferior Nasal chonchae/turbinates Vomer Maxillae: Intermaxillary suture Infraorbital foramen alveolar processes incisive foramen Zygomatic Bones temporal arch zygomaticofacial foramen Lacrimal Bones lacrimal fossa Mandible body rami angle condyloid process coronoid process mandibular foramen mental foramen alveolar process mandiubular condyles mandiubular notch Orbits (eye sockets) Formed by seven skull bones: 3 cranial; 4 facial: Frontal Sphenoid Ethmoid Zygomatic Maxillae Lacrimal Palatine Associated structures include: optic foramen superior orbital fissure inferior orbital fissure Bones associated with the skull Hyoid Bone: greater cornu lesser cornu body Auditory Ossicles: Malleus Incus Stapes 3 1. Label the following illustration of the skull (anterior view): 4 2. Label the following illustration of the skull (midsagittal view): 5 3. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

6. the Pharynx the Pharynx, Which Forms the Upper Part of the Digestive Tract, Consists of Three Parts: the Nasopharynx, the Oropharynx and the Laryngopharynx
6. The Pharynx The pharynx, which forms the upper part of the digestive tract, consists of three parts: the nasopharynx, the oropharynx and the laryngopharynx. The principle object of this dissection is to observe the pharyngeal constrictors that form the back wall of the vocal tract. Because the cadaver is lying face down, we will consider these muscles from the back. Figure 6.1 shows their location. stylopharyngeus suuperior phayngeal constrictor mandible medial hyoid bone phayngeal constrictor inferior phayngeal constrictor Figure 6.1. Posterior view of the muscles of the pharynx. Each of the three pharyngeal constrictors has a left and right part that interdigitate (join in fingerlike branches) in the midline, forming a raphe, or union. This raphe forms the back wall of the pharynx. The superior pharyngeal constrictor is largely in the nasopharynx. It has several origins (some texts regard it as more than one muscle) one of which is the medial pterygoid plate. It assists in the constriction of the nasopharynx, but has little role in speech production other than helping form a site against which the velum may be pulled when forming a velic closure. The medial pharyngeal constrictor, which originates on the greater horn of the hyoid bone, also has little function in speech. To some extent it can be considered as an elevator of the hyoid bone, but its most important role for speech is simply as the back wall of the vocal tract. The inferior pharyngeal constrictor also performs this function, but plays a more important role constricting the pharynx in the formation of pharyngeal consonants. -

A New Radiological Classification for the Risk Assessment of Anterior Skull
www.nature.com/scientificreports OPEN A new radiological classifcation for the risk assessment of anterior skull base injury in endoscopic sinus surgery Baharudin Abdullah 1*, Shiun Chuen Chew1, Mohd Ezane Aziz2, Norasnieda Md Shukri1, Salina Husain3, Sng Weirong Joshua4, De Yun Wang4 & Kornkiat Snidvongs5 Keros and Gera classifcations are widely used to assess the risk of skull base injury during endoscopic sinus surgery. Although, both classifcations are useful preoperatively to stratify risk of patients going for surgery, it is not practical to measure the respective lengths during surgery. In this study, we aimed to propose a new radiological classifcation (Thailand-Malaysia-Singapore (TMS)) to assess the anatomical risk of anterior skull base injury using the orbital foor (OF) as a reference. A total of 150 computed tomography images of paranasal sinuses (300 sides) were reviewed. The TMS classifcation was categorized into 3 types by measuring OF to cribriform plate and OF to ethmoid roof. Most patients were classifed as TMS type 1, Keros type 2 and Gera class II, followed by patients classifed as TMS type 3, Keros type 1 and Gera class 1. TMS has signifcant correlation with Keros classifcation (p < 0.05). There was no signifcant correlation between Keros and Gera classifcations (p = 0.33) and between TMS and Gera classifcations (p = 0.80). The TMS classifcation has potential to be used for risk assessment of skull base injury among patients undergoing ESS. It serves as an additional assessment besides the Keros and Gera classifcations. Endoscopic sinus surgery (ESS) has an overall complication rate of 0.5% with the specifc complications of cere- brospinal fuid leak, orbital injury, haemorrhage requiring surgery, blood transfusion and toxic shock syndrome at 0.09%, 0.09%, 0.10%, 0.18%, and 0.02%, respectively1. -

Lab Manual Axial Skeleton Atla
1 PRE-LAB EXERCISES When studying the skeletal system, the bones are often sorted into two broad categories: the axial skeleton and the appendicular skeleton. This lab focuses on the axial skeleton, which consists of the bones that form the axis of the body. The axial skeleton includes bones in the skull, vertebrae, and thoracic cage, as well as the auditory ossicles and hyoid bone. In addition to learning about all the bones of the axial skeleton, it is also important to identify some significant bone markings. Bone markings can have many shapes, including holes, round or sharp projections, and shallow or deep valleys, among others. These markings on the bones serve many purposes, including forming attachments to other bones or muscles and allowing passage of a blood vessel or nerve. It is helpful to understand the meanings of some of the more common bone marking terms. Before we get started, look up the definitions of these common bone marking terms: Canal: Condyle: Facet: Fissure: Foramen: (see Module 10.18 Foramina of Skull) Fossa: Margin: Process: Throughout this exercise, you will notice bold terms. This is meant to focus your attention on these important words. Make sure you pay attention to any bold words and know how to explain their definitions and/or where they are located. Use the following modules to guide your exploration of the axial skeleton. As you explore these bones in Visible Body’s app, also locate the bones and bone markings on any available charts, models, or specimens. You may also find it helpful to palpate bones on yourself or make drawings of the bones with the bone markings labeled. -

Lab Week 7 Part 1 Radius and Ulna
11/7/2018 Lab Week 7 Part 1 Radius and Ulna Part 1 Activities 1. Observe bones and structures from list 2. Bones of the Forearm worksheet in packet 3. Bones of the Pectoral Girdle and Upper Limbs worksheet in packet Part 2 Femur, Tibia, & Fibula 1 11/7/2018 Part 2 Activities 1. Observe bones and structures from list 2. Bones of the Lower Limbs worksheet in packet 3. Bones of the Pelvic Girdle and Lower Limbs worksheet in packet Functions of the Skull • Support • Movement Part 3 • Protection Skull Notes may be found in your packet: SS 27-28 The Skull The Skull 22 bones, 2 groups 2. Facial bones (14 bones) 1. Cranial bones (8) • Framework of face • Enclose the brain in the cranial cavity • Cavities for special sense organs of sight, taste, and • Provide sites of attachment for head and neck muscles smell • • Provide support Openings for air and food passage • Sites of attachment for teeth and muscles of facial expression 2 11/7/2018 Sutures Bones of cranium (cranial vault) • Immovable joints Coronal suture – Become more complex with age Squamous • Fontanelles suture – Soft regions of connective tissue holding bones together at birth • Permits – Brain growth Lambdoid Facial suture bones – Entry into birth canal Occipitomastoid – Normally replaced by bone by about 1 year of age suture Cranial and facial divisions of the skull Foramina Sinuses • Allow passage of blood vessels and nerves • Cavities lined with mucous membranes & ciliated epithelium – • About 85 named openings (foramina, canals, Frontal sinus – Sphenoidal sinus fissures) – Maxillary -

The Skull O Neurocranium, Form and Function O Dermatocranium, Form
Lesson 15 ◊ Lesson Outline: ♦ The Skull o Neurocranium, Form and Function o Dermatocranium, Form and Function o Splanchnocranium, Form and Function • Evolution and Design of Jaws • Fate of the Splanchnocranium ♦ Trends ◊ Objectives: At the end of this lesson, you should be able to: ♦ Describe the structure and function of the neurocranium ♦ Describe the structure and function of the dermatocranium ♦ Describe the origin of the splanchnocranium and discuss the various structures that have evolved from it. ♦ Describe the structure and function of the various structures that have been derived from the splanchnocranium ♦ Discuss various types of jaw suspension and the significance of the differences in each type ◊ References: ♦ Chapter: 9: 162-198 ◊ Reading for Next Lesson: ♦ Chapter: 9: 162-198 The Skull: From an anatomical perspective, the skull is composed of three parts based on the origins of the various components that make up the final product. These are the: Neurocranium (Chondocranium) Dermatocranium Splanchnocranium Each part is distinguished by its ontogenetic and phylogenetic origins although all three work together to produce the skull. The first two are considered part of the Cranial Skeleton. The latter is considered as a separate Visceral Skeleton in our textbook. Many other morphologists include the visceral skeleton as part of the cranial skeleton. This is a complex group of elements that are derived from the ancestral skeleton of the branchial arches and that ultimately gives rise to the jaws and the skeleton of the gill -

MBB: Head & Neck Anatomy
MBB: Head & Neck Anatomy Skull Osteology • This is a comprehensive guide of all the skull features you must know by the practical exam. • Many of these structures will be presented multiple times during upcoming labs. • This PowerPoint Handout is the resource you will use during lab when you have access to skulls. Mind, Brain & Behavior 2021 Osteology of the Skull Slide Title Slide Number Slide Title Slide Number Ethmoid Slide 3 Paranasal Sinuses Slide 19 Vomer, Nasal Bone, and Inferior Turbinate (Concha) Slide4 Paranasal Sinus Imaging Slide 20 Lacrimal and Palatine Bones Slide 5 Paranasal Sinus Imaging (Sagittal Section) Slide 21 Zygomatic Bone Slide 6 Skull Sutures Slide 22 Frontal Bone Slide 7 Foramen RevieW Slide 23 Mandible Slide 8 Skull Subdivisions Slide 24 Maxilla Slide 9 Sphenoid Bone Slide 10 Skull Subdivisions: Viscerocranium Slide 25 Temporal Bone Slide 11 Skull Subdivisions: Neurocranium Slide 26 Temporal Bone (Continued) Slide 12 Cranial Base: Cranial Fossae Slide 27 Temporal Bone (Middle Ear Cavity and Facial Canal) Slide 13 Skull Development: Intramembranous vs Endochondral Slide 28 Occipital Bone Slide 14 Ossification Structures/Spaces Formed by More Than One Bone Slide 15 Intramembranous Ossification: Fontanelles Slide 29 Structures/Apertures Formed by More Than One Bone Slide 16 Intramembranous Ossification: Craniosynostosis Slide 30 Nasal Septum Slide 17 Endochondral Ossification Slide 31 Infratemporal Fossa & Pterygopalatine Fossa Slide 18 Achondroplasia and Skull Growth Slide 32 Ethmoid • Cribriform plate/foramina -

Compact Bone Spongy Bone
Spongy bone Compact bone © 2018 Pearson Education, Inc. 1 (b) Flat bone (sternum) (a) Long bone (humerus) (d) Irregular bone (vertebra), right lateral view (c) Short bone (talus) © 2018 Pearson Education, Inc. 2 Articular cartilage Proximal epiphysis Spongy bone Epiphyseal line Periosteum Compact bone Medullary cavity (lined by endosteum) Diaphysis Distal epiphysis (a) © 2018 Pearson Education, Inc. 3 Trabeculae of spongy bone Osteon (Haversian Perforating system) (Volkmann’s) canal Blood vessel continues into medullary cavity containing marrow Blood vessel Lamellae Compact bone Central (Haversian) canal Perforating (Sharpey’s) fibers Periosteum Periosteal blood vessel (a) © 2018 Pearson Education, Inc. 4 Lamella Osteocyte Canaliculus Lacuna Central Bone matrix (Haversian) canal (b) © 2018 Pearson Education, Inc. 5 Osteon Interstitial lamellae Lacuna Central (Haversian) canal (c) © 2018 Pearson Education, Inc. 6 Articular cartilage Hyaline Spongy cartilage bone New center of bone growth New bone Epiphyseal forming plate cartilage Growth Medullary in bone cavity width Bone starting Invading to replace Growth blood cartilage in bone vessels length New bone Bone collar forming Hyaline Epiphyseal cartilage plate cartilage model In an embryo In a fetus In a child © 2018 Pearson Education, Inc. 7 Bone growth Bone grows in length because: Articular cartilage 1 Cartilage grows here. Epiphyseal plate 2 Cartilage is replaced by bone here. 3 Cartilage grows here. © 2018 Pearson Education, Inc. 8 Bone remodeling Growing shaft is remodeled as: Articular cartilage Epiphyseal plate 1 Bone is resorbed by osteoclasts here. 2 Bone is added (appositional growth) by osteoblasts here. 3 Bone is resorbed by osteoclasts here. © 2018 Pearson Education, Inc. 9 Hematoma External Bony callus callus of spongy bone New Internal blood callus vessels Healed (fibrous fracture tissue and Spongy cartilage) bone trabecula 1 Hematoma 2 Fibrocartilage 3 Bony callus 4 Bone remodeling forms.