Southend-On-Sea Localities Needs Profile
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

WAKERING ROAD, THORPE BAY, SOUTHEND, ESSEX LA FITNESS Wakering Road, Thorpe Bay, Southend, Essex LA FITNESS Wakering Road, Thorpe Bay, Southend, Essex
WELL SECURED FREEHOLD LEISURE INVESTMENT WITH DEVELOPMENT POTENTIAL WAKERING ROAD, THORPE BAY, SOUTHEND, ESSEX LA FITNESS Wakering Road, Thorpe Bay, Southend, Essex LA FITNESS Wakering Road, Thorpe Bay, Southend, Essex Investment Summary Health and Fitness Club with 2 tennis courts and indoor swimming pool. Secured to L A Fitness Ltd for a further 30.5 years. Annual fixed uplifts at 2.5% per annum compound until December 2016. Passing rent reflects £74.28 per sq m (£6.90 per sq ft). Highly reversionary ERV at £107.64 per sq m (£10.00 per sq ft). Total net internal area of 2,811 sq m (30,248 sq ft). 102 car parking spaces providing an excellent ratio of 1:28 sq m (1:297 sq ft). Site area of 0.93 hectares (2.29 acres). Capital value reflects £1,410 per sq m (£131 per sq ft) and £4.3 million per hectare (£1.7 million per acre). Situated in an affluent residential suburb of Southend-on-Sea. Residential potential, subject to the necessary consents. Purchase price in excess of £3,950,000. Net initial yield of 5.0%. Reversionary yield of 7.2%. True equivalent yield of 6.6%. LA FITNESS Wakering Road, Thorpe Bay, Southend, Essex Location Communications Southend-on-Sea is the principal commercial centre in Essex and a popular tourist The north east quadrant of the M25 provides access to Southend via the A12 at resort. The town is situated approximately 72.0 kilometres (45.0 miles) east of Central Junction 28, the A127 at Junction 29 and the A13 at Junction 30. -
Shoeburyness Coastal Management Scheme Non- Technical Study
Shoeburyness Coastal Management Scheme Non- Technical Study Southend-on-Sea Borough Council This document is issued for the party which commissioned it and for specific purposes connected with the above-captioned project only. It should not be relied upon by any other party or used for any other purpose. We accept no responsibility for the consequences of this document being relied upon by any other party, or being used for any other purpose, or containing any error or omission which is due to an error or omission in data supplied to us by other parties. This document contains confidential information and proprietary intellectual property. It should not be shown to other parties without consent from us and from the party which commissioned it. The consultant has followed accepted procedure in providing the services but given the residual risk associated with any prediction and the variability which can be experienced in flood conditions, the consultant takes no liability for and gives no warranty against actual flooding of any property (client’s or third party) or the consequences of flooding in relation to the performance of the service. This report has been prepared for the purposes of informing the Shoeburyness Flood and Erosion Risk Management Scheme only. Shoeburyness Coastal Management Scheme 2 Contents Introduction 4 Aim of Document 4 Shoeburyness Coastal Management Scheme Area 5 The Need for Action 6 Key Issues for the Frontage 6 Section 1: Thorpe Bay Yacht Club to the groyne between the beachs huts on the beach and those on the promenade 6 Section 2: The groyne between the beach and those on the promenade to the H.M.Coastguard 6 Section 3: HM.Coastguard Station to World War 2 Quick Fire Battery 6 Flood and Erosion Risk 7 Flood Risk 7 Erosion Risk 7 Current Risks 7 Managing Impacts on the Environment 8 Designated Areas 8 Coastal Squeeze 8 Environmental Report 8 Appraisal Process 9 Task 1: Long List of Options 10 Task 2: Develop the Short List of Options 10 1. -

Sponsored Walk Saturday 10Th October 2020
th Sponsored Walk Saturday 10 October 2020 Firstly, thank you for joining us on this sponsored walk to raise funds for our programs, and raising awareness of recovery. Our programs enable people to understand why they started to use in the first place, and offer long term trauma informed support, for as long as a person needs us. Secondly, due to Corona Virus, we all need to be mindful of social distancing and with that in mind, when walking and interacting please follow government advice. Please bring your own facemasks and hand sanitiser. More information can be found at https://www.gov.uk/coronavirus Start time: From 17:00 to 18:30 Location: East Beach, Shoeburyness, SS3 9AE Meeting point: Opposite East Beach Car Park is a children’s play area. We shall meet within that vicinity. Volunteers will be stood with our banner Aspirations Program Community Interest Company Company number: 12596744 Facilities: There are public toilets, but please bring your own water and food. You will pass shops along the walk. Parking: East Beach Car Park, is opposite our meeting point. This is a paid car park. Nearest bus stop: Next to our meeting point. Bus times and destinations can be found https://moovitapp.com/index/en-gb/public_transportation-line-9-London_and_South_East-2122-970986- 3663783-1 Nearest train station: Shoeburyness Train, High Street, Shoeburyness, Essex, SS3 9AW is a 5 minutes walk to East Beach. C2C Trains come from London and stop locally along the way. https://www.c2c-online.co.uk/stations/shoeburyness-station/ For those parking at East Beach, you will be able to get the train back from Leigh-on-Sea, which is our end point. -

509 Bus Time Schedule & Line Map
509 bus time schedule & line map 509 Southchurch - Thorpe Bay - Chalkwell - Leigh On View In Website Mode Sea The 509 bus line Southchurch - Thorpe Bay - Chalkwell - Leigh On Sea has one route. For regular weekdays, their operation hours are: (1) Leigh-On-Sea: 7:50 AM Use the Moovit App to ƒnd the closest 509 bus station near you and ƒnd out when is the next 509 bus arriving. Direction: Leigh-On-Sea 509 bus Time Schedule 32 stops Leigh-On-Sea Route Timetable: VIEW LINE SCHEDULE Sunday Not Operational Monday 7:50 AM Jones Memorial Recreation Ground, Southchurch Tuesday 7:50 AM Fossetts Way, Southchurch Wednesday 7:50 AM La Fitness, Bournes Green Thursday 7:50 AM Albert Road, Southend-on-Sea Friday 7:50 AM Brankscombe Walk, Bournes Green Shoebury Road, Southend-on-Sea Saturday Not Operational Maplin Way North, Bournes Green North Shoebury Corner, North Shoebury 509 bus Info North Shoebury Corner, North Shoebury Direction: Leigh-On-Sea A13, Southend-on-Sea Stops: 32 Trip Duration: 37 min St Marys Church, North Shoebury Line Summary: Jones Memorial Recreation Ground, Southchurch, Fossetts Way, Southchurch, La Shoebury Park, North Shoebury Fitness, Bournes Green, Brankscombe Walk, Bournes North Shoebury Road, Southend-on-Sea Green, Maplin Way North, Bournes Green, North Shoebury Corner, North Shoebury, North Shoebury Shoebury Sports Centre, Shoeburyness Corner, North Shoebury, St Marys Church, North Shoebury, Shoebury Park, North Shoebury, Shoebury Thorpedene School, Shoeburyness Sports Centre, Shoeburyness, Thorpedene School, Shoeburyness, -

Southend-On-Sea an Area and Market Guide P2 P3
SOUTHEND-ON-SEA AN AREA AND MARKET GUIDE P2 P3 You have arrived… Southend-on-Sea is a place for all ages to live, work and grow – offering a new Southend-on-Sea’s Gross Value pace, vibrancy and ease many are eager to call home. Added is set to rise 20% by 2030 A newfound magnetism In response to this growing popularity, Southend-on-Sea is currently receiving a series of investments to elevate its innate character. The town is undergoing an extensive, government-backed regeneration programme to key civic areas. Likewise, some of the UK’s leading property developers, such as Weston Homes, are capitalising on ONS data shows the number of the town’s newfound potential, and have begun building state-of- people moving from across the the-art communities. These initiatives will only enable the town’s economy to further flourish. UK to Southend-on-Sea is up 19% In fact, according to Experian, the area is already set to outperform over the past five years, with 40% most of its wider region (the East of England) over the next decade. of movers aged between 20-34 UK migration into Southend, Thousands of people 2019 9,541 ONS data shows that median 2018 8,887 gross weekly earnings increased 2017 9,098 by 23% between 2015 and 2019, compared to 14% across the East 2016 8,069 of England region, 12% in London 2015 8,014 and 13% across the UK Source: ONS, Knight Frank Research The number of people who moved to Southend increased from 8,014 for the 12-month period to June 2015 up to 9,541 for the same period up to June 2019. -
Southend (2012)
EC Regulation 854/2004 CLASSIFICATION OF BIVALVE MOLLUSC PRODUCTION AREAS IN ENGLAND AND WALES SANITARY SURVEY REPORT Southend 2012 SANITARY SURVEY REPORT SOUTHEND Cover photo: Intertidal area at Southend. CONTACTS: For enquires relating to this report or For enquires relating to policy matters on further information on the the implementation of sanitary surveys in implementation of sanitary surveys in England and Wales: England and Wales: Simon Kershaw/Alastair Cook Beverley Küster Food Safety Group Hygiene Delivery Branch Cefas Weymouth Laboratory Enforcement and Delivery Division Barrack Road, Food Standards Agency The Nothe Aviation House WEYMOUTH 125 Kingsway Dorset LONDON DT43 8UB WC2B 6NH +44 (0) 1305 206600 +44 (0) 20 7276 8000 [email protected] [email protected] © Crown copyright, 2012. Pacific oysters, cockles and mussels at Southend 2 SANITARY SURVEY REPORT SOUTHEND STATEMENT OF USE: This report provides information from a study of the information available relevant to perform a sanitary survey of bivalve mollusc classification zones at Southend. Its primary purpose is to demonstrate compliance with the requirements for classification of bivalve mollusc production areas, determined in EC Regulation 854/2004 laying down specific rules for the organisation of official controls on products of animal origin intended for human consumption. The Centre for Environment, Fisheries & Aquaculture Science (Cefas) undertook this work on behalf of the Food Standards Agency (FSA). CONSULTATION: Consultee Consultation Date Response Date Environment Agency 30/08/2012 15/10/2012 London Port Health Authority 31/07/2012 16/10/2012 Inshore Fisheries and Conservation Authority 02/08/2012 13/08/2012 Anglian Water 31/07/2012 29/08/2012 DISSEMINATION: Food Standards Agency, London Port Health Authority, Environment Agency, Kent and Essex Inshore Fisheries and Conservation Authority. -

E-Newsletter – 29Th October 2020
E-Newsletter – 29th October 2020 www.bera.co.uk © Andrew Armstrong Photography 1) Information Corner Scams A member has contacted us with more possible scams. Please see the below email information from the member: a) Talktalk They asked him to take a customer satisfaction survey and enter a prize draw. In fact it wasn't talktalk at all and when he looked carefully at the mail (without clicking on anything of course) it came from someone registered at 801 US Highway California. b) Boots Boots letting him know he has a surprise gift waiting for him if he clicked on the link or phone a number. The actual address at the top of the mail was 'cordenbitcoin' so another scam. c) Door to Door mask sales People are going door to door handing out masks, they say it’s a new initiative from local Government. They will always ask you to please put it on to see if it fits you. It has been doused with chemicals which knocks you out cold and once you’re knocked out, they proceed to rob you. Page | 1 Please do not accept masks from strangers. Remember, we are living in critical times and people are desperate to take advantage with the aim of making money. Crime rate has skyrocketed, so please be cautious and play it safe. d) Vodafone A member received a message from Vodafone saying that they are unable to process his payment and to follow the ink. However, the member does not have a contract with Vodafone. e) HMRC The same member had a telephone call from HMRC, which was a scam as HMRC do not phone the public. -
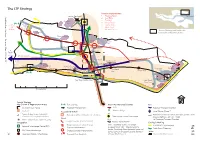
X Fig 5 .2 the LTP Strategy
The LTP Strategy Junction Improvements 1 Progress Road Southend S London Southend o 2 Kent Elms u Airport t h 3 The Bell e Aviation n Way 4 Sutton Road d to P+R P+R - Progress 5 Fairfax Drive o Chelmsford n and A Road 6 West Road - 1 Eastwood S Basildon 27 7 Victoria Circus e Thames Gateway and Sustainable a Airborne L x Communities Plan Growth Area o 1 c a Thanet Grange l T r a 2 n Temple s Fossetts p Farm o Farm r 3 t A1 P Southend 4 159 l a Hospital n to 2 Basildon Prittlewell 0 0 and 6 Canvey London Road 5 t o 2 6 Sutton Road A13 0 A13 Southchurch 1 1 A127 Leigh Southend Victoria Leigh Broadway Hamlet Court 7 New Vanguard Chalkwell Road Southend Ranges Thorpe Bay Way Southend Central East P+R Westcliff 0 8 6 9 1 Towerfield 0 0 0 1 r e Shoeburyness b See Town Centre Inset West Road/ m u N Ness Road e c n e Old ic L t Ranges h g ri y p o c 5 kilometres n w ro C © Spatial Strategy Key Growth & Regeneration Areas P+R Park and Ride Major Maintenance Schemes Bus Southend Town Centre Passenger Transport Link A127 Passenger Transport Corridor Seafront Accessibility to Rail x Warners Bridge Travel Centre (Phase 2) Air Priority Urban Areas - Industrial / Population within 1 kilometre of rail station Potential Corridor for Urban Transport System - SERT Commercial / Employment Areas New railway station/interchange Roads (bus, guided bus, light rail - linked Priority Urban Areas - District Centres Rail to Passenger Transport Corridor) Freight Corridor (A127 / A1159) Integration Railway Improvements Cycling & Walking Priory Crescent / Cuckoo Corner ‘one’ - Southend Victoria to London F SUSTRANS Cycle Network i Regional Interchange Centre (RIC) g Highway Improvements Liverpool Street ‘c2c’ - Shoeburyness to Prittle Brook Greenway London Fenchurch Street (potential metro rail 5 Key Urban Interchanges Strategic Junction Improvements Water . -

215 Northwyke, Southchurch Boulevard, Southend-On-Sea, Essex, ., SS2 4UU Asking Price £220,000
EPC D 215 Northwyke, Southchurch Boulevard, Southend-on-Sea, Essex, ., SS2 4UU Asking Price £220,000 Approximately 810 square feet (plus entry lobby & garage). Abbotts are delighted to welcome to the market this spacious two bedroom first floor flat situated within a popular development on the Thorpe Bay borders and available with no onward chain. This excellent property offers an exciting opportunity for the lucky buyers to add their own stamp, while the all round well proportioned accommodation consists of a bright lounge with an open aspect and a 'Juliette' style balcony, a kitchen/diner, two double bedrooms, fitted shower room and a separate guest's WC. This superb apartment further benefits from a its own garage and residents parking, lots of handy built-in storage, an intercom entry system, uPVC double glazing and is located within easy reach of bus and train services, plus Thorpe Bay's Broadway and Seafront. abbotts.co.uk Viewing arrangement by appointment 01702 582249 [email protected] Abbotts, 154 The Broadway, Thorpe Bay, SS1 3ES Interested parties should satisfy themselves, by inspection or otherwise as to the accuracy of the description given and any floor plans shown in these property details. All measurements, distances and areas listed are approximate. Fixtures, fittings and other items are NOT included unless specified in these details. Please note that any services, heating systems, or appliances have not been tested and no warranty can be given as to their working order. A member of Countrywide plc. Countrywide Estate Agents, trading as Abbotts. Registered in England No. 789476 | Code: Anglia EA_10045_TBY200291_AL6PLB. -

BERA E-Newsletter 10Th September 2020
BERA E-Newsletter 10th September 2020 - www.bera.co.uk Dear Member We have altered the layout of our newsletter and although the COVID-19 information is still very important to us all, we have lost the feel of our personal BERA newsletter. Therefore, we are putting our BERA information at the top along with the news that is happening in our area, with all other news below. However, as there are not so many events happening in the area at the moment, we will also be going back to sending our newsletter out once a week, on a Thursday. We hope that you will find this a more enjoyable read and thank you for your continued support. Keep well, Regards Ron 1) Information Corner New BERA website As you know, we were undertaking a website redesign. This is still in the process of being completed but if you go to www.bera.co.uk, you will be able to see the changes that have currently been made. I am sure that you will agree that this looks so much better and more friendly to use. You can now use any mobile device to view the website and once it is fully completed, we will let you know all of the other benefits that this will offer. Photos for the website If any photographers have any high resolution images for the website of our area that we can display, please email them to either Ron at [email protected] or Mike at [email protected] and we will include them on the new website. -

3, Butterys, Thorpe Bay, Southend-On-Sea, Essex, SS1 3DT Guide Price £400,000
EPC E 3, Butterys, Thorpe Bay, Southend-on-Sea, Essex, SS1 3DT Guide Price £400,000 An Extended Four Bedroom Detached House With West Facing Garden, Garage & Parking Requires Refurbishment & Chain Free The property is situated in a popular Thorpe Bay location within close proximity to local shops, Thorpe Bay Broadway and both Thorpe Bay and Southend East mainline railway stations to London Fenchurch Street. In addition it is within the Thorpe Greenways Primary School catchment and within easy reach of Southend High School for Girls the seafront, Southchurch Park, Southend-on-Sea town centre and amenities with good local road transport links to the A13 and the A127 GUIDE PRICE £400,000 - £415,000 An opportunity has arisen to purchase this extended four bedroom family home with an approximate 30ft front garden , 80ft west facing rear garden, garage and driveway providing off street parking and is brought to market requiring refurbishment, with no onward chain. The additional accommodation comprises a living room, dining room, kitchen/breakfast room, first floor bathroom, and ground floor WC. Benefits include a west facing balcony to bedroom three overlooking the rear garden, double glazing and gas central heating. The property presents as an ideal family home for someone to refurbish to their personal taste. For viewing by appointment only Please contact Bairstoweves. Viewing arrangement by appointment 01702 467701 [email protected] Bairstow Eves, 373 Southchurch Road, Southend-On-Sea, SS1 2PQ https://www.bairstoweves.co.uk Interested parties should satisfy themselves, by inspection or otherwise as to the accuracy of the description given and any floor plans shown in these property details. -

Southend Airport Surface Access Strategy December 2011
Airport Surface Access Strategy December 2011 London Southend Airport Co. Ltd. London Southend Airport Southend-on-Sea Essex SS26YF T: +44 1702 608 100 W: www.southendairport.com Company: London Southend Airport Document: Airport Surface Access Strategy – December 2011 Contents Chapter Title Page FOREWORD 3 1 INTRODUCTION 4 2 SUMMARY OF TARGETS, COMMITTMENTS AND ACTIONS 7 3 LONDON SOUTHEND AIRPORT TODAY AND OUR FUTURE PLANS 9 4 NATIONAL, REGIONAL AND LOCAL POLICIES 17 5 AIR PASSENGER AND EMPLOYEE SURFACE ACCESS 23 6 SUSTAINABLE TRANSPORT 26 7 ROAD NETWORK AND PARKING 35 8 MONITORING AND REVIEW 43 APPENDIX A AIRPORT TRAVEL PLAN 45 APPENDIX B THE SOUTHEND AIRPORT TRANSPORT FORUM 59 2 Company: London Southend Airport Document: Airport Surface Access Strategy – December 2011 Foreword FOREWORD Since becoming Managing Director of London Southend Airport in 2007, I have worked hard to ensure the potential of the airport to serve and support the local area is realised. This year we were delighted to open the Airport’s railway station and in just a few months’ time our new terminal building will be up and running, our extended runway operational and new airline services will have commenced. The return of passenger traffic to the airport after a long period of decline, and the many new staff that are being employed to support our new operations will bring not only great opportunities, but also present new challenges. One of these challenges is how to manage the transport needs of our passengers and airport staff. When we gained planning permission to extend the runway we gave a commitment to working with our local authority partners to prepare a surface access strategy for the airport.