Use of Oral Iodized Oil to Control Iodine
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

GENERAL AGREEMENT on °90M '2£Ft& TARIFFS and TRADE Limited
RESTRICTED 0M GENERAL AGREEMENT ON °9 '2£ft& TARIFFS AND TRADE Limited Distribution Oonaitteg II - Expansion of Trade DOCUMENTATION FOR FUTURE WORK OF COMMITTEE II Addendum Attached for the information of the Committee is the revised summary schedule of non-tariff devices affecting vegetable oils. COM.ll/85/Add.4 VEGETABLE OILS Page 2/3 Income and Price Support Aids, to Exports (3) (7) (8) (9) (10) (11) (12) (1) (2) Consumer (4) (5) (6) Surplus Quantitative State Mixing Other Non-tariff GATT Tariff Production Other Forms of Income and Subsidy Subsidy Financing Indirect Disposal Restrictions Trading Regulations Devices and Remarks Bindings Subsidy Price Support of Losses Aids United States Seo column (2) Cottonseed ( non-mandatory) Export of cottons.ied, See column See column (4) Foes on flaxseed and linseed The United States Purchase programme for Olive oil, kapok C0M.II/2(J)/Rev.l Loans on farm-stored cotton tung oil and flaxseed (4) oil of 502 ad valorem under takes the position edible grados of pea-r seed oil, C0tUI/2(j)/Rev.l/ seed purchases. by CCC at less than Section 22. that the activities nuts of less than top cottonseed oil, Add.l Soyabeans and flaxseed domestic market Section 22 quotas for peanuts of the CCC do not quality for crushing palm kernel oil, COM. 11/37 (non-mandatory) prices. (global). constitute State into oil. Soil bank sesame oil, COM. 11/59 Loans to producers. Imports peanut oil and/or trading within the (conservation reserve coconut oil, L/1048 Purchase Agreement. withdrawal from warehouses meaning of programme). -
The Effect of Linseed Oil on the Properties of Lime-Based Restoration Mortars
Allma Mater Studiiorum – Uniiversiità dii Bollogna DOTTORATO DI RICERCA Science for Conservation Ciclo XXII Settore/i scientifico disciplinari di afferenza: CHIM/12 TITOLO TESI THE EFFECT OF LINSEED OIL ON THE PROPERTIES OF LIME-BASED RESTORATION MORTARS Presentata da: Eva Čechová Coordinatore Dottorato Relatore Prof. Rocco Mazzeo Prof. Ioanna Papayianni Esame finale anno 2009 Abstract THE EFFECT OF LINSEED OIL ON THE PROPERTIES OF LIME-BASED RESTORATION MORTARS The traditional lime mortar is composed of hydrated lime, sand and water. Besides these constituents it may also contain additives aiming to modify fresh mortar´s properties and/or to improve hardened mortar´s strength and durability. Already in the first civilizations various additives were used to enhance mortar´s quality, among the organic additives, linseed oil was one of the most common. From literature we know that it was used already in Roman period to reduce water permeability of a mortar, but the mechanism and the technology, e.g. effects of different dosages, are not clearly explained. There are only few works studying the effect of oil experimentally. Knowing the function of oil in historical mortars is important for designing a new compatible repair mortar. Moreover, linseed oil addition could increase the sometimes insufficient durability of lime-based mortars used for reparation and it could be a natural alternative to synthetic additives. In the present study, the effect of linseed oil on the properties of six various lime- based mortars has been studied. Mortars´ compositions have been selected with respect to composition of historical mortars, but also mortars used in a modern restoration practise have been tested. -
Almond Oil 92
Iodine value Oil / Fat g/100 g Almond oil 92 - 106 94 - 101 Apricot kernel oil 97 - 110 Argan seed oil 92 - 102 Avocado oil 63 - 95 85 - 90 Babassu oil 10 - 18 10 - 18 Blackcurrent oil 173 182 Camelina oil 127 - 155 130 - 145 Cashew nut oil 79 - 89 Castor oil 82 - 88 81 - 91 Chia oil 190 - 199 196 - 199 Cocoa butter 33 - 40 32 - 40 Coconut oil 6 - 9 6,3 - 11 6 - 11 Coconut oil, cochin 7 - 12 Coconut oil, RBD 7 - 12 Corn oil 127 - 133 Cottonseed oil 103 - 115 100 - 123 100 - 115 Cottonseed oil, RBD 98 - 118 Crambe oil 93 Flaxseed oil 182 - 203 Grape seed oil 130 - 138 128 - 150 Hazelnut oil 85 - 95 Illipe butter 58 - 65 Linseed oil 170 - 204 Maize germ oil 103 - 128 103 - 135 107 - 128 Melon seed oil 124 Mustardseed oil 92 - 125 Oiticica oil 140 - 180 Iodine value Oil / Fat g/100 g Olive oil 75 - 94 Ongokea oil 180 - 205 Palm kernel oil 16 - 23 14,1 - 21 Palm oil 50,6 - 55 51 - 54 50 - 55 Palm olein 56 - 61 Palm stearin Palm oil, neutralized 50 - 55 Palm oil, neutralized and bleached 50 - 55 ≥ 56 Palm oil (RBD/NBD) 50 - 55 Palm olein, crude 56 Palm olein, neutralized 56 Palm olein, neutralized and bleached 56 Palm olein (RBD/NBD) 56 Palm stearin 22 - 49 ≤ 48 Palm superolein ≥ 60 Peanut oil 86 - 107 86 - 107 Peanut oil, Africa 85 - 90 Peanut oil, South America 92 - 110 Perilla oil 192 - 208 Poppyseed oil 130 - 143 Pumpkin seed oil 117 Rapeseed oil 94 - 120 Rapeseed oil (Canola) 110 - 126 Rapeseed oil, erucic acid incl. -
Niop Trading Rules
NIOP TRADING RULES Effective July 2013 Minor changes and corrections (approved by the NIOP Technical Committee) have been included as of July 29, 2013 APPLICATION OF RULES INCORPORATION OF THESE RULES OR ANY PORTION THEREOF IS NOT MANDATORY BUT IS OPTIONAL BETWEEN PARTIES TO CONTRACTS. Published by the National Institute of Oilseed Products 750 National Press Building, 529 14th St NW Washington, D.C. 20045 TEL: (202) 591-2438 FAX: (202) 591-2445 e-mail: [email protected] Internet: www.niop.org ©2013 by the National Institute of Oilseed Products NIOP TRADING RULES TABLE OF CONTENTS CHAPTER 1 - TYPES OF SALES RULE 1.1 TRADE PRACTICE 1 -1 1.2 PLACE OF CONTRACT 1 -1 1.3 C.I.F. (COST, INSURANCE AND FREIGHT) 1 -1 LISTING OF DOCUMENTS 1 -2 1.4 C.& F. (COST AND FREIGHT) 1 -3 1.5 F.O.B. VESSEL (FREE ON BOARD VESSEL) 1 -3 1.6 F.A.S. VESSEL (FREE ALONGSIDE) -NAMED PORT OF SHIPMENT 1 -5 1.7 EX DOCK (NAMED PORT OF IMPORTATION) 1 -6 1.8 EX WAREHOUSE 1 -7 1.9 MISCELLANEOUS TYPES OF SALES 1 -7 1.10 VESSEL CLASSIFICATION 1 -7 1.11 PUBLIC HEALTH SECURITY AND BIOTERRORISM PREPAREDNESS 1 -7 CHAPTER 2 - SHIPMENT RULE 2.1 TIME 2 -1 2.2 DAYS OR HOURS 2 -1 2.3 NOTICE 2 -1 2.4 TENDERS 2 -1 2.5 EXTENSION OF SHIPMENT 2 -1 2.6 PROOF OF ORIGIN 2 -3 2.7 TRANSHIPMENT 2 -3 2.8 SHIPPING INSTRUCTIONS 2 -3 2.9 VESSEL NOMINATION AND DECLARATION OF DESTINATION 2 -3 2.10 BILL OF LADING-EVIDENCE OF DATE OF SHIPMENT 2 -3 CHAPTER 3 - TANK CARS, TRUCKS, BARGES AND CONTAINERS RULE 3.1 DATE OF SHIPMENT 3 -1 3.2 TIME OF SHIPMENT 3 -1 3.3 SPREAD (SCATTERED) DELIVERIES OF SHIPMENTS 3 -1 3.4 F.O.B. -

Essential Ingredients in Fine Cuisine
ESSENTIAL INGREDIENTS IN FINE CUISINE FINE VINEGAR www.goelles.at AND SOON THERE‘S VINEGAR CLASSIC TYPES APPLE WHITE WINE The Volcano Country is known as RED WINE Austrian‘s orchard. ROSÉ WINE The fruit has to be fully ripe and juicy before we can use it to make fi ne vinegar. Special fl air and passion as well as peace of mind are required to make our delicacies, which have meanwhile become essential ingredients in CREATIVE TYPES fi ne cuisine. BEER THE PATHWAY TO THE PERFECT SALAD PEAR RASPBERRY CHERRY APRICOT QUINCE TOMATO ENJOY YOUR SALAD PLUM DRY THE LETTUCE IN A SALAD SPINNER 2 TO 3 PARTS OIL FOR 1 PART VINEGAR BALSAMIC VINEGARS SEASONINGS & APPLE BALSAMIC SALT PEAR BALSAMIC WINE BALSAMIC MIX IN THE WHITE BALSAMIC DRESSING CAREFULLY DO NOT ADD WATER OR SUGAR FINE VINEGAR ESSENTIAL INGREDIENTS IN FINE CUISINE FINE VINEGAR www.goelles.at Ap APPLE CLASSIC EVERYBODY‘S DARLING Styrian bright fruity tartness Deeply rooted in its Styrian home- land, apple vinegar is widely used in 2 YEARS the area. One possible explanation is OAK that it combines wonderfully with another BARREL typical local product, pumpkin seed oil. Fermented from heirloom varieties, such as Maschansker, Rosenäpfel (“rose” apples) or Bohnäpfel (“bean” apples), and aged in oak barrels, this vinegar features fruity tartness and the unique PURE FRUIT taste of fully ripened apples. 125 ml EXCELLENT IN: COMBINE 250 ml WELL WITH: 500 ml green salads 5 l goulash soup pumpkin seed oil carrot salad olive oil Tafelspitz sunfl ower oil Acidity: 5 % No expiration date FINE VINEGAR ESSENTIAL INGREDIENTS IN FINE CUISINE FINE VINEGAR www.goelles.at Zw ZWEIGELT RED WINE CLASSIC EVERYBODY‘S DARLING full flavour strong enormous opulence When Austrians mention red wine, they often mean the popular Zweigelt 2 YEARS OAK grape, and this is the raw material for BARREL this vinegar. -

Biodiesel from Afghanistan Poppies
Biodiesel from Afghanistan Poppies Proposal from CSIRO Plant Industry, Canberra. Dr Philip Larkin March, 2007 Background Current world diesel consumption is about 1087 billion litres p.a. Biodiesel currently accounts for 0.4% of the total, but this is increasing due to mandated targets in Europe. Europe currently accesses much of its biodiesel from palm oil. However palm oil has poor “cold flow” properties (high viscosity when cold). Preferred so-called “soft” oils have good cold flow properties. Poppy seed oil is a soft oil composed of 12% palmitic (16:0), 19% oleic (18:1) and 56% linoleic (18:2) fatty acids. Unmodified poppyseed oil biodiesel would blend well with diesel in Europe. Afghanistan is very dependent on imported fuel, not least to power many thousands of local electrical generators. Shortages are frequent and power stoppages very disruptive to the economy. Village-scale biodiesel processing is available technology. Poppyseed biodiesel would be a carbon- neutral energy source, produced and processed in very many localities in Afghanistan and becoming the foundation of a major export industry, especially into the rapidly expanding European market. The business model might involve villages jointly owning the production, crushing and biodiesel processing equipment. Poppy seed yields are already impressive, being about 1.8 tonnes/ha seed (cf. 2.4 for canola). The oil content is exceptional at 45-50% oil content per unit seed weight (cf. 40% in canola). Poppy yields about 0.8 tonnes oil per ha. The area sown to illegal poppy in Afghanistan in 2004 was 131,000 ha. This is less than 2% of the arable land and therefore could be greatly expanded when the crop becomes legalized. -

Cosmetic Oils Assortment Henry Lamotte Oils Gmbh
Product Portfolio Cosmetics Discover our broad product range Henry Lamotte Oils GmbH is a leading supplier and producer of oils, waxes and seed flour as well as colours and flavourings – in conventional as well as in certified organic qualities. Oils and fats for the cosmetics industry ils and fats are two of the most important cosmetic ingredients and are deployed in a variety of very different external applications, for example skin care products such as creams, lotions, lipsticks, massage oils as well as hair care products such as shampoos, conditioners and hair tonics. Henry Lamotte Oils – partners to the... • cosmetics industry • pharmaceuticals industry and wholesale pharmaceuticals • food processing industries and the food wholesale and retail industry • veterinary and feed industry • chemicals industry Our services • production, contract manufacturing and bottling • worldwide purchasing and sales • quality assurance and in-house laboratories • quality management • product development, customer-specific recipes • EU certified organic operation (DE-ÖKO-003) • officially licensed pharmaceutical company (GMP) • Kosher and Halal certified • BSCI-membership and continuing sustainability efforts 02.2020 Natural Special Oils – Cosmetic Ingredients: Our products are available as... • pressed • refined • hydrogenated • fractionated • conventional • certified organic ...qualities For more information do not hesitate to contact us! Oils and special ingredients Flour Açai Oil Manketti Oil Almond Flour Linseed Flour Ahiflower® Oil Marula Oil -

RULE 5.12 - PRIOR CARGO LISTINGS September 1, 2007
RULE 5.12 - PRIOR CARGO LISTINGS September 1, 2007 NOTE: All substances on Acceptable Lists 1 and 2 also appear on the NIOP-FOSFA Harmonized International List of Acceptable Previous Cargoes except those designated by (*). Substances not appearing on either Acceptable List 1 or 2 are not permitted to be carried as the last cargo immediately prior to edible oils. 5.12.1 - ACCEPTABLE PRIOR CARGO - LIST NO. 1 The following items are acceptable prior cargoes for transported edible oils, which may or may not be further processed prior to use: CARGO COMMON NAME Acetic acid – (USP and Food Grades only) Alcoholic beverages (i.e. rum, wine) Almond oil Anchovy oil Apple juice concentrate Apricot kernel oil Avocado oil Babassu oil Beechnut oil Beeswax (white & yellow) Candelilla wax Canola oil - LEAR (“double zero”) Carnauba wax Castor oil Cocoa butter Coconut oil Cod liver oil Cod oil Cohune oil Corn oil - (maize oil) Corn syrup Cottonseed oil Dairy products (limited per USA 21CFR, Part 131) Dextrose solution Ethyl alcohol – (Food Grades only) Fish liver oil Fish oil Fructose Glucose syrup Glycerin Grape juice concentrate Grapeseed oil Hazelnut oil Herring oil Illipe butter - (mowrah butter) Juice concentrates (i.e. apple, grape) Lactic acid (limited per USA 21CFR, Parts 150 & 184) Lard Linseed oil Lycopersicum esculentum oil - (tomato seed oil) Menhaden oil Molasses Montan wax Murumuru fat Mustard seed oil Non-alcoholic beverages Nutmeg butter Olive oil Orange juice slurry Palm kernel oil Palm kernel olein Palm kernel stearin Palm oil 5.12.1 - -
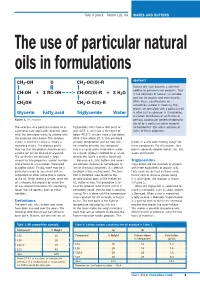
The Use of Particular Natural Oils in Formulations
Tony O’Lenick – Siltech LLC, US WAXES AND BUTTERS The use of particular natural oils in formulations ABSTRACT CH2-OH O CH2-OC(O)-R Natural oils have become a common additive to personal care products. They CH-OH +3 RC-OH CH-OC(O)-R + 3 H2O fit the definition of natural, sustainable and can be organic and even organic. CH OH CH -O-C(O)-R While these classifications are 2 2 sometimes unclear in meaning, the reason we formulate with a particular oil Glycerin Fatty acid Triglyceride Water is often just as obscure. Is it marketing, or carbon distribution or aesthetics or Figure 1: The reaction. perhaps a particular benefit rendered to the oil by a particular native material The selection of a particular natural oil in triglycerides. Fats have a titer point of (antioxidants)? This article will look at a personal care application depends upon over 40.5˚C, oils have a titer point of some of these properties. what the formulator wants to achieve with below 40.5˚C. Butters have a titer below the particular formulation. The simplest 40.5˚C but above 20˚C. Oils are liquid choice is when the choice is simply a at room temperature and we now use results in a very wide melting ‘range’ for marketing choice. The product profile this word to describe any compound these compounds. For this reason, titer may say that the product should contain that is a liquid and is insoluble in water. point is generally determined on fats, oils, a particular oil like olive oil or argan oil. -

Almond Butter, Sweet Almond Oil, Sweet Aloe
NaOH (oz.) KOH (oz.) Sodium Potassium Hydroxide Hydroxide Oil SAP (for Bar Soaps) (for Liquid Soaps) INCI Name Almond Butter, Sweet 90 - 140 0.098 0.139 Prunus amygdalus dulcis (Sweet Almond) Oil Almond Oil, Sweet 190 - 200 0.137 0.194 Prunus amygdalus dulcis (Sweet Almond) Oil Aloe Butter 220 - 260 0.176 0.247 Cocos Nucifera (Coconut) Oil and Aloe Barbadensis Leaf Extract Aloe Vera Oil 185 - 200 0.135 0.191 Apricot Kernel Butter 130 - 145 0.097 0.1361 Prunus armeniacae (Apricot) Kernel Oil Apricot Kernel Oil 185 - 195 0.135 0.19 Prunus armeniaca (Apricot) Kernel Oil Argan Oil 0.192 .136 Argania Spinosa Avocado Butter 177 - 198 0.132 0.186 Hydrogenated Persea gratissima (Avocado) Seed Oil Avocado Oil 177 - 198 0.133 0.188 Persea gratissima (Avocado) Oil Babassu Oil 245-256 0.178 0.251 Orbignya oleifera (Babassu) Seed Oil Baobab Oil 190 - 220 0.143 0.202 Adansonia digitata (Baobab) Seed Oil Beef Tallow 190 - 200 0.14 0.196 Beeswax, white 89 - 103 0.067 0.095 Beeswax Beeswax, yellow 89 - 103 0.067 0.095 Beeswax Black currant Oil 185 - 195 0.134 0.188 Ribes nigrum (Blackcurrant) Fruit Oil Borage Oil 175 - 196 0.134 0.189 Borago officinalis (Borage) Seed Oil Brazil Nut Oil 245-256 0.176 0.247 Camellia Oil 185 - 197 0.134 0.189 Camellia oleifera (Camellia) Seed Oil Candelilla Wax 43 - 65 0.038 0.053 Canola Oil 0.132 0.187 Castor Oil 175 - 187 0.127 0.179 Ricinus communis (Castor) Seed Oil Cherry Kernel Oil 182-202 0.138 0.194 Prunus avium (Cherry) Kernel Oil Cocoa Butter (deodorized)188 - 200 0.136 0.192 Theobroma cacao (Cocoa) Seed Butter -
SANA OIL EXTRACTOR User Manual
SANA OIL EXTRACTOR User Manual • Keep the user manual where you can fi nd easily and read “Important Safeguards” before using the product. • This product is for home use (domestic use) and its Model commercial and industrial use is prohibited. EUJ702 TABLE OF CONTENTS Read this fiRst ..........................................................................................................................3 iMPORTANt safeGUaRds..........................................................................................................4 teChNiCaL sPeCifiCATIONs .....................................................................................................5 PaRts List ...................................................................................................................................5 JUiCeRs COMPATIBLe With the saNa OiL eXtRaCtOR ......................................................6 NUts aNd seeds that CaN Be PROCessed .........................................................................6 ChOOsiNG seeds .......................................................................................................................7 ChOOsiNG the ReGULATING RiNG ..........................................................................................8 seeds aNd NUts PRePaRATION ..............................................................................................9 asseMBLY iNstRUCtiONs ....................................................................................................... 10 OPeRATING iNstRUCtiONs .................................................................................................... -

Oil and Fats Anise Seed Oil Apricot Kernel Oil Avellana Oil Avocado Oil
Oil and Fats Anise seed oil Apricot kernel oil Avellana oil Avocado oil Baobab oil Chia seed oil Cranberry seed oil Strawberry seed oils Tigernuts oil (earth almond oil) Peanut oil Fig seed oil Goji seed oil Pomegranate seed oil Cucumber seed oil Rose hip seed oil Hemp seed oil Hazelnut oil Raspberry seed oil Elderberry seed oil Black currant seed oil Jojoba oil Coffee bean oil Prickly pear seed oil Camellia oleifera seed oil Cherry kernel oil Coconut oil Coriander seed oil Cumin seed oil Pumpkin seed oil Camelina seed oil Linseed oil Almond oil Poppy seed oil Moringa oil Evening primrose oil Neem oil Brazil nut oil Passion fruit seed oil Pequi oil Perilla seed oil Peach kernel oil Plum kernel oil Castor oil Sacha inchi seed oil Sea buckthorn pulp oil Sea buckthorn seed oil Black cumin seed oil Tamanu oil Grape seed oil Brazil nut oil Walnut oil Watermelon seed oil Wheat germ oil Cedar nut oil Açai Oil Ahiflower Oil Amaranth Oil Argan Oil Avocado Oil Babassu Oil Black Currant Oil Borageseed Oil Brazilnut Oil Broccoliseed Oil Calendula Oil Camelina Oil Castor Oil Chilean Hazelnut Oil Coconut Oil Corn Oil Cottonseed Oil Evening Primrose Oil Grapeseed Oil Groundnut Oil Hazelnut Oil Hemp Oil Kukuinut Oil Laurel Oil Linseed Oil Macadamianut Oil Manketti Oil Marula Oil MCT Oil Meadowfoam Seed Oil Milk Thistle Oil Moringa Oil Mustardseed Oil Olive Oil Olus Oil Omega-3-6-9-Oils Palm Oil Palmkernel Oil Palmolein Palmstearin Oil Passionfruit Seed Pecan Nut Oil Perilla Oil Pistachionut Oil Pomegranate Oil Poppyseed Oil Pumpkinseed Oil Rapeseed Oil Rice Bran Oil Rose Hip Oil Sacha Inchi Oil Safflower Oil Seabuckthorn Pulp Oil Sesame Oil Soybean Oil St.