Exome Sequencing Identifies FANCM As a Susceptibility Gene for Triple-Negative Breast Cancer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

This Document Has Been Downloaded from Tampub – the Institutional Repository of University of Tampere
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Trepo - Institutional Repository of Tampere University This document has been downloaded from Tampub – The Institutional Repository of University of Tampere Post-print Authors: Häkli Jouni Cultures of demarcation : territory and national identity in Name of article: Finland Name of work: Nested identities : identity, territory, and scale Editors of work: Herb Guntram H., Kaplan David H. Year of 1999 publication: ISBN: 0-8476-8466-0 Publisher: Rowman & Littlefield Pages: 123-149 Discipline: Social sciences / Social and economic geography Language: en URN: http://urn.fi/urn:nbn:uta-3-959 All material supplied via TamPub is protected by copyright and other intellectual property rights, and duplication or sale of all part of any of the repository collections is not permitted, except that material may be duplicated by you for your research use or educational purposes in electronic or print form. You must obtain permission for any other use. Electronic or print copies may not be offered, whether for sale or otherwise to anyone who is not an authorized user. Author’s copy. Originally published in Guntram H. Herb & D. H. Kaplan (eds.). Nested identities: Identity, Territory, and Scale. Lanham: Rowman & Littlefield (1999), 123-149. Cultures of Demarcation: Territory and National Identity in Finland JOUNI HÄKLI Introduction This chapter explores the significance of geographical scale in the negotiation of spatial identities, and especially attempts to understand the processes of nation- building in Finland, which stands out as an exceptional case among the several "successor states" born out of the European geopolitical turmoil in the turn of the 19th and 20th centuries. -

The Kainuu Regional Experiment
SJPA The Kainuu regional experiment: deliberate and 19(4) unintended effects of scaling local government tasks to the regional level Arto Haveri, Jenni Airaksinen and Anni Jäntti* Abstract Arto Haveri This article examines the deliberate and unintended effects of the Kainuu Regional Exper- School of Management, iment, a regional reform where some important local government tasks were rescaled to University of Tampere the regional level. The analysis is based on the empirical results of a long-running evalua- [email protected] tion study. In Kainuu, the new regional government was successful in securing the quality Jenni Airaksinen and availability of welfare services, but in the task of regional development ‒ creating School of Management, new growth and development ‒ its role has been practically secondary, and in some cases University of Tampere the new regional government has been marginalised by the tensions built into it during the rescaling process. The Kainuu experiment exemplifies a case of rescaling where some Anni Jäntti (political) tensions between two perspectives/factors, service and development, were School of Management, rescaled together with local government functions, reflecting the reformer’s problem that University of Tampere it is extremely difficult to achieve many different outcomes with one governance expedi- ent. Altering the scale of governance has consequences for political decision-making, power structures, institutions, and citizens. Rescaling through a restructuring of hierarchy may produce different outcomes -

Economic Development of Ultra Small Peripheral Regions of West Europe (Case of Aland and Faroe Islands)
A Service of Leibniz-Informationszentrum econstor Wirtschaft Leibniz Information Centre Make Your Publications Visible. zbw for Economics Efimova, Elena; Kuznetsova, Natalia Conference Paper Economic development of ultra small peripheral regions of West Europe (Case of Aland and Faroe islands) 54th Congress of the European Regional Science Association: "Regional development & globalisation: Best practices", 26-29 August 2014, St. Petersburg, Russia Provided in Cooperation with: European Regional Science Association (ERSA) Suggested Citation: Efimova, Elena; Kuznetsova, Natalia (2014) : Economic development of ultra small peripheral regions of West Europe (Case of Aland and Faroe islands), 54th Congress of the European Regional Science Association: "Regional development & globalisation: Best practices", 26-29 August 2014, St. Petersburg, Russia, European Regional Science Association (ERSA), Louvain-la-Neuve This Version is available at: http://hdl.handle.net/10419/124527 Standard-Nutzungsbedingungen: Terms of use: Die Dokumente auf EconStor dürfen zu eigenen wissenschaftlichen Documents in EconStor may be saved and copied for your Zwecken und zum Privatgebrauch gespeichert und kopiert werden. personal and scholarly purposes. Sie dürfen die Dokumente nicht für öffentliche oder kommerzielle You are not to copy documents for public or commercial Zwecke vervielfältigen, öffentlich ausstellen, öffentlich zugänglich purposes, to exhibit the documents publicly, to make them machen, vertreiben oder anderweitig nutzen. publicly available on the internet, or to distribute or otherwise use the documents in public. Sofern die Verfasser die Dokumente unter Open-Content-Lizenzen (insbesondere CC-Lizenzen) zur Verfügung gestellt haben sollten, If the documents have been made available under an Open gelten abweichend von diesen Nutzungsbedingungen die in der dort Content Licence (especially Creative Commons Licences), you genannten Lizenz gewährten Nutzungsrechte. -

The Finnish Archipelago Coast from AD 500 to 1550 – a Zone of Interaction
The Finnish Archipelago Coast from AD 500 to 1550 – a Zone of Interaction Tapani Tuovinen [email protected], [email protected] Abstract New archaeological, historical, paleoecological and onomastic evidence indicates Iron Age settle- ment on the archipelago coast of Uusimaa, a region which traditionally has been perceived as deso- lated during the Iron Age. This view, which has pertained to large parts of the archipelago coast, can be traced back to the early period of field archaeology, when an initial conception of the archipelago as an unsettled and insignificant territory took form. Over time, the idea has been rendered possible by the unbalance between the archaeological evidence and the written sources, the predominant trend of archaeology towards the mainland (the terrestrical paradigm), and the history culture of wilderness. Wilderness was an important platform for the nationalistic constructions of early Finnishness. The thesis about the Iron Age archipelago as an untouched no-man’s land was a history politically convenient tacit agreement between the Finnish- and the Swedish-minded scholars. It can be seen as a part of the post-war demand for a common view of history. A geographical model of the present-day archaeological, historical and palaeoecological evi- dence of the archipelago coast is suggested. Keywords: Finland, Iron Age, Middle Ages, archipelago, settlement studies, nationalism, history, culture, wilderness, borderlands. 1. The coastal Uusimaa revisited er the country had inhabitants at all during the Bronze Age (Aspelin 1875: 58). This drastic The early Finnish settlement archaeologists of- interpretation developed into a long-term re- ten treated the question of whether the country search tradition that contains the idea of easily was settled at all during the prehistory: were perishable human communities and abandoned people in some sense active there, or was the regions. -

FOOTPRINTS in the SNOW the Long History of Arctic Finland
Maria Lähteenmäki FOOTPRINTS IN THE SNOW The Long History of Arctic Finland Prime Minister’s Office Publications 12 / 2017 Prime Minister’s Office Publications 12/2017 Maria Lähteenmäki Footprints in the Snow The Long History of Arctic Finland Info boxes: Sirpa Aalto, Alfred Colpaert, Annette Forsén, Henna Haapala, Hannu Halinen, Kristiina Kalleinen, Irmeli Mustalahti, Päivi Maria Pihlaja, Jukka Tuhkuri, Pasi Tuunainen English translation by Malcolm Hicks Prime Minister’s Office, Helsinki 2017 Prime Minister’s Office ISBN print: 978-952-287-428-3 Cover: Photograph on the visiting card of the explorer Professor Adolf Erik Nordenskiöld. Taken by Carl Lundelius in Stockholm in the 1890s. Courtesy of the National Board of Antiquities. Layout: Publications, Government Administration Department Finland 100’ centenary project (vnk.fi/suomi100) @ Writers and Prime Minister’s Office Helsinki 2017 Description sheet Published by Prime Minister’s Office June 9 2017 Authors Maria Lähteenmäki Title of Footprints in the Snow. The Long History of Arctic Finland publication Series and Prime Minister’s Office Publications publication number 12/2017 ISBN (printed) 978-952-287-428-3 ISSN (printed) 0782-6028 ISBN PDF 978-952-287-429-0 ISSN (PDF) 1799-7828 Website address URN:ISBN:978-952-287-429-0 (URN) Pages 218 Language English Keywords Arctic policy, Northernness, Finland, history Abstract Finland’s geographical location and its history in the north of Europe, mainly between the latitudes 60 and 70 degrees north, give the clearest description of its Arctic status and nature. Viewed from the perspective of several hundred years of history, the Arctic character and Northernness have never been recorded in the development plans or government programmes for the area that later became known as Finland in as much detail as they were in Finland’s Arctic Strategy published in 2010. -

Dual Origins of Finns Revealed by Y Chromosome Haplotype Variation Rick A
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Am. J. Hum. Genet. 62:1171–1179, 1998 Dual Origins of Finns Revealed by Y Chromosome Haplotype Variation Rick A. Kittles,1 Markus Perola,4 Leena Peltonen,4 Andrew W. Bergen,2 Richard A. Aragon,2 Matti Virkkunen,5 Markku Linnoila,3 David Goldman,2 and Jeffrey C. Long1 1Section on Population Genetics and Linkage, 2Laboratory of Neurogenetics, and 3Laboratory of Clinical Studies, National Institute on Alcohol Abuse and Alcoholism, National Institutes of Health, Bethesda; 4Department of Human Molecular Genetics, National Public Health Institute, and 5Department of Psychiatry, University of Helsinki, Helsinki Summary studies on genetic disorders, has increased rapidly. At present, there are 133 rare genetic diseases that are more The Finnish population has often been viewed as an prevalent in Finland than in other populations (de la isolate founded 2,000 years ago via a route across the Chapelle 1993). The high prevalence of these rare dis- Gulf of Finland. The founding event has been charac- eases has been attributed to founder effects resulting terized as involving a limited number of homogeneous from Finland’s unique population history. This unique- founders, isolation, and subsequent rapid population ness is conspicuously reflected by the fact that, unlike growth. Despite the purported isolation of the popula- most other Europeans, Finns do not speak an Indo-Eur- tion, levels of gene diversity for the Finns at autosomal opean language. Finnish is a member dialect of the Uralic and mitochondrial DNA loci are indistinguishable from language family, whose only other speakers within Eu- those of other Europeans. -
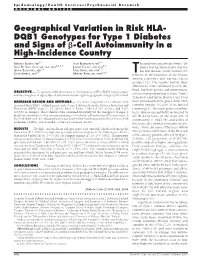
Geographical Variation in Risk HLA- DQB1 Genotypes for Type 1 Diabetes and Signs of ß-Cell Autoimmunity in a High-Incidence
Epidemiology/Health Services/Psychosocial Research ORIGINAL ARTICLE Geographical Variation in Risk HLA- DQB1 Genotypes for Type 1 Diabetes and Signs of -Cell Autoimmunity in a High-Incidence Country 1,2 1,6 MARIKA KUKKO, MD SARI KORHONEN, MD he epidemiological map of type 1 di- 1,2,3,4 1,7 SUVI M. VIRTANEN, MD, MSC, PHD JORMA ILONEN, MD, PHD abetes that has been drawn over the 1,2 1,5 ANNA TOIVONEN, MD OLLI SIMEL, MD, PHD 1,5 1,2,8 last few decades shows marked dif- ATU IMELL MD IKAEL NIP MD, PHD T S S , M K , ferences in the incidence of the disease among countries and various racial groups (1,2). The reasons behind these differences have remained poorly de- fined, but both genetic and environmen- OBJECTIVE — To assess possible differences in the frequency of HLA-DQB1 risk genotypes and the emergence of signs of -cell autoimmunity among three geographical regions in Finland. tal factors may contribute to them. Type 1 diabetes is a polygenic disorder, but it has RESEARCH DESIGN AND METHODS — The series comprised 4,642 children with been estimated that the genes of the HLA increased HLA-DQB1–defined genetic risk of type 1 diabetes from the Diabetes Prediction and complex explain 30–60% of its familial Prevention (DIPP) study: 1,793 (38.6%) born in Turku, 1,646 (35.5%) in Oulu, and 1,203 clustering (3). The main genes contribut- (25.9%) in Tampere. These children were examined frequently for the emergence of signs of ing to disease susceptibility are located in -cell autoimmunity, for the primary screening of which islet cell antibodies (ICA) were used. -

Ruderals and Weeds in Godby, Åland Islands, SW Finland
Memoranda Soc. Soc. Fauna Fauna Flora Flora Fennica Fennica 91, 91: 2015 21–32. • Hæggström 2015 & Hæggström 21 Ruderals and weeds in Godby, Åland Islands, SW Finland Carl-Adam Hæggström & Eeva Hæggström Carl-Adam Hæggström, Finnish Museum of Natural History, Botanical Museum, P. O. Box 7, FI- 00014 University of Helsinki, Finland. E-mail: [email protected] Eeva Hæggström, Tornfalksvägen 2/26, FI-02620 Esbo, Finland. E-mail: eeva.haeggstrom@ kolumbus.fi The Åland Islands in SW Finland are known for their luxuriant vegetation with numerous calci- philic vascular plants. Ruderal plants are rather few compared to the adjoining regions of Finland and Sweden. However, new ruderal plants are occasionally found in Åland. We came across a ruderal site in the centre of the village of Godby, municipality of Finström, in 2002. Most of the organic topsoil had been removed and several rare ruderal species grew then on the open ruderal site. The site became more closed, resembling a meadow rather than a ruderal ground already in 2006 and later the vegetation developed into a tall and rough grown meadow with some shrubs and young trees. The following ruderal plants are treated more in detail: Agrostemma githago, Anthemis tinctoria, Centaurea cyanus, Cichorium intybus, Dianthus deltoides (cultivar), Echium vulgare, Holcus lanatus, Leontodon hispidus, Lotus corniculatus var. sativus, Papaver dubium subsp. dubium, P. rhoeas, Phleum phleoides, Rumex thyrsiflorus, Senecio jacobaea, Thymus pule- gioides, Trifolium dubium and Vicia tenuifolia. Besides some trees and shrubs, 133 vascular plant taxa, most of them common in the Åland Islands, were observed growing in the ruderal site during the period 2002–2015. -
STATE of the NORDIC REGION 2018 STATE of the NORDIC REGION 2018 Julien Grunfelder, Linus Rispling and Gustaf Norlén (Eds.)
STATE OF THE NORDIC REGION 2018 STATE OF THE NORDIC REGION 2018 Julien Grunfelder, Linus Rispling and Gustaf Norlén (eds.) Nord 2018:001 ISBN 978-92-893-5280-2 (PRINT) ISBN 978-92-893-5281-9 (PDF) ISBN 978-92-893-5282-6 (EPUB) http://dx.doi.org/10.6027/NORD2018-001 © Nordic Council of Ministers 2018 Layout: Louise Jeppesen and Gitte Wejnold Linguistic editing: Chris Smith Cover Photo: unsplash.com Photos: unsplash.com, except photo on page 22 by Johner Bildbyrå Print: Rosendahls Printed in Denmark Nordic co-operation Nordic co-operation is one of the world’s most extensive forms of regional collaboration, involving Denmark, Finland, Iceland, Norway, Sweden, the Faroe Islands, Greenland, and Åland. Nordic co-operation has firm traditions in politics, the economy, and culture. It plays an important role in European and international collaboration, and aims at creating a strong Nordic community in a strong Europe. Nordic co-operation seeks to safeguard Nordic and regional interests and principles in the global community. Shared Nordic values help the region solidify its position as one of the world’s most innovative and competitive. Nordic Council of Ministers Nordens Hus Ved Stranden 18 DK-1061 Copenhagen K www.norden.org Download Nordic publications at www.norden.org/nordpub STATE OF THE NORDIC REGION 2018 Julien Grunfelder, Linus Rispling and Gustaf Norlén (eds.) COUNTRY CODES FOR FIGURES AX Åland DK Denmark FI Finland FO Faroe Islands GL Greenland IS Iceland NO Norway SE Sweden EU The European Union EU28 The 28 European Union member states -

Regional Socio-Economic Disparities in Finland
Stefan Fina, Bastian Heider, Maija Mattila, Pauli Rautiainen, Mikko-Waltteri Sihvola, Kaisa Vatanen Unequal Finland Regional socio-economic disparities in Finland FRIEDRICH-EBERT-STIFTUNG – POLITICS FOR EUROPE Europe needs social democracy! Why do we need Europe? Can we demonstrate to European citizens the opportu- nities offered by social politics and a strong social democracy in Europe? This is the aim of the new Friedrich-Ebert-Stiftung project “Politics for Europe”. It shows that European integration can be done in a democratic, economic and socially balanced way and with a reliable foreign policy. The following issues will be particularly important: – Democratic Europe – Social and ecological transformation – Economic and social policy in Europe – Foreign and security policy in Europe We focus on these issues in our events and publications. We provide impetus and offer advice to decision-makers from politics and trade unions. Our aim is to drive the debate on the future of Europe forward and to develop specific proposals to shape central policy areas. With this publication series we want to engage you in the debate on the “Politics for Europe”! About this publication On the outset and in international comparison, Finland has developed one of the wealthiest and most generous welfare states in the world and with low levels of income inequality and high social mobility. A deeper look reveals deepening re- gional disparities, leading to the observation that in fact there are four Finlands. Following Finland's post-war industrialisation, the rate of urbanisation and rural depopulation have been rapid, however the country's demographic change and stagnating unemployment rate have increased regional inequalities and put in- creasing pressure on municipalities. -

ECONOMY State of the Nordic Region 2018 Theme 3: Economy Julien Grunfelder, Linus Rispling and Gustaf Norlén (Eds.)
STATE OF THE NORDIC REGION 2018 THEME 3: ECONOMY State of the Nordic Region 2018 Theme 3: Economy Julien Grunfelder, Linus Rispling and Gustaf Norlén (eds.) Nord 2018:004 ISBN 978-92-893-5478-3 (PRINT) ISBN 978-92-893-5480-6 (PDF) ISBN 978-92-893-5479-0 (EPUB) http://dx.doi.org/10.6027/NORD2018-001 © Nordic Council of Ministers 2018 Layout: Louise Jeppesen and Gitte Wejnold Linguistic editing: Chris Smith Cover Photo: unsplash.com Photos: unsplash.com, except photo on page 22 by Johner Bildbyrå Nordic co-operation Nordic co-operation is one of the world’s most extensive forms of regional collaboration, involving Denmark, Finland, Iceland, Norway, Sweden, the Faroe Islands, Greenland, and Åland. Nordic co-operation has firm traditions in politics, the economy, and culture. It plays an important role in European and international collaboration, and aims at creating a strong Nordic community in a strong Europe. Nordic co-operation seeks to safeguard Nordic and regional interests and principles in the global community. Shared Nordic values help the region solidify its position as one of the world’s most innovative and competitive. Nordic Council of Ministers Nordens Hus Ved Stranden 18 DK-1061 Copenhagen K www.norden.org Download Nordic publications at www.norden.org/nordpub STATE OF THE NORDIC REGION 2018 THEME 3: ECONOMY Julien Grunfelder, Linus Rispling and Gustaf Norlén (eds.) COUNTRY CODES FOR FIGURES AX Åland DK Denmark FI Finland FO Faroe Islands GL Greenland IS Iceland NO Norway SE Sweden EU The European Union EU28 The 28 European -

Policy Guidelines for Regions Falling Under The
Milano Csil Policy guidelines for regions falling under the new regional competitiveness and employment objective for the 2007 - 2013 period in the fields of the knowledge economy and the environment, in line with the Lisbon and Gothenburg objectives Call for tenders by open procedure N° 2004 CE 16 0 AT 039 Policy guidelines for regions falling under the new regional competitiveness and employment objective for the 2007 - 2013 period Vol. II Country Report. FINLAND Prepared for: European Commission December 2005 DG REGIONAL POLICY Conception and analysis, accession negotiations unit CSIL, Centre for Industrial Studies- Milan EPRC, European Policies Research Centre and FAI- Fraser of Allander Institute, University of Strathclyde - Glasgow DMIO, Department of Management and Industrial Organisation, Marche Polytechnic University - Ancona Mazars & Guérard, Evaluation & Pilotage des politiques publiques-Paris Country Expert: Hallgeir Aalbu, EuroFutures - Stockholm Milano Csil DISCLAIMER This report was produced by a consortium led by CSIL-Centre for Industrial Studies (Milan) for the Regional Policy Directorate General and represents the views of the contractor. These views were produced in order to provide analytical support for the Commission services. They have not been adopted by the Commission and do not necessarily represent the view of the Commission itself or the Directorate General for Regional Policy. The Team takes full responsibility for the data, information and judgments expressed in the present report. CSIL - CENTRO STUDI INDUSTRIA LEGGERA Scrl Corso Monforte 15 20122 Milano - Italy Tel. +39 02 796630 Fax +39 02 780703 [email protected] www.csildevelopment.com Cod. Fiscale e Partita Iva 04825320155 CCIAA Iscriz. n. 1042964 Reg. Soc.