Transcript of Public Hearing on Fentantyl and Fentanyl Analogues
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Backing Material Packaging Liner
US009314527B2 (12) United States Patent (10) Patent No.: US 9,314,527 B2 Cottrell et al. (45) Date of Patent: *Apr. 19, 2016 (54) TRANSDERMAL DELIVERY PATCH 9/7061 (2013.01); A61K 9/7084 (2013.01); (71) Applicant: Phosphagenics Limited, Clayton, A61 K3I/355 (2013.01); A61K47/24 Victoria (AU) SE7 8E.O. (72) Inventors: Jeremy Cottrell, Caulfield South (AU); ( .01): ( .01): (2013.01) Giacinto Gaetano, South Melbourne (AU); Mahmoud El-Tamimy, Meadow (58) Field of Classification Search Heights (AU); Nicholas Kennedy, None Boronia (AU); Paul David Gavin, See application file for complete search history. Chadstone (AU) (56) References Cited (73) Assignee: Phosphagenics Limited, Victoria (AU) (*) Notice: Subject to any disclaimer, the term of this U.S. PATENT DOCUMENTS patent is extended or adjusted under 35 2,407,823. A 9, 1946 Fieser U.S.C. 154(b) by 0 days. 2.457,932 A 1/1949 Solmssen et al. This patent is Subject to a terminal dis- (Continued) claimer. (21) Appl. No.: 14/550,514 FOREIGN PATENT DOCUMENTS ppl. No.: 9 (22) Filed: Nov. 21, 2014 A 3.3 5.83 (65) Prior Publication Data (Continued) Related U.S. Application Data Gianello et al. Subchronic Oral Toxicity Study of Mixed Tocopheryl (63) Continuation of application No. 14/086,738, filed on Phosphates in Rates, International Journal of Toxicology, 26:475 Nov. 21, 2013, now abandoned, which is a 490; 2007.* continuation of application No. 13/501,500, filed as (Continued) application No. PCT/AU2011/000358 on Mar. 30, 2011, now Pat. No. 8,652,511. Primary Examiner — Robert A Wax (60) Provisional application No. -

Understanding and Challenging the Drugs: Chemistry and Toxicology
UNDERSTANDING AND CHALLENGING THE DRUGS: CHEMISTRY AND TOXICOLOGY Presenter: • Dr. Jasmine Drake, Graduate Program Director and Assistant Professor, Administration of Justice Department, Barbara Jordan-Mickey Leland School of Public Affairs, Texas Southern University NACDL Training Defending Drug Overdose Homicides in Pennsylvania Penn State Harrisburg, Middletown, PA November 6th, 2019 11:30- 12:45 p.m. Understanding & Challenging the Drugs: Chemistry & Toxicology Dr. Jasmine Drake, Forensic Science Learning Laboratory, Texas Southern University I. Opioid Drug Classifications A. Types of Opioids B. Classic vs. Synthetic C. Toxicology of Opioids 1) How opioids interact with the body 2) Addiction (psychological vs. physiological II. New Classes of Drugs A. Emerging Threats B. Potency III. National Trends in Opioid Overdose Deaths in the U.S. A. Based on State B. Ethnicity C. Drug-Type (prescription vs. fentanyl vs. heroin) IV. Trends of Opioid Overdose Deaths in Philadelphia A. Based on Ethnicity B. Drug Type (prescription vs. fentanyl vs. heroin) V. Legal Considerations to the Opioid Epidemic A. Punitive Measures vs. Rehabilitative Treatment B. Progressive Jurisdictions Nationwide C. New Legal Measures in Philadelphia VI. Toxicology Reports A. What’s in the report? B. Key Aspects of the Tox Report C. Terminology D. Evaluating and Interpreting the data? E. Questions and considerations. VII. Conclusion and Discussion A. Case Specific Examples B. Sample Toxicology Reports The Opioid Epidemic: What labs have to do with it? Ewa King, Ph.D. Associate Director of Health RIDOH State Health Laboratories Analysis. Answers. Action. www.aphl.org Overview • Overdose trends • Opioids and their effects • Analytical testing approaches • Toxicology laboratories Analysis. Answers. Action. -

Measures and CDS for Safer Opioid Prescribing: a Literature Review
Measures and CDS for Safer Opioid Prescribing: A Literature Review Measures and CDS for Safer Opioid Prescribing: A Literature Review Executive Summary The U.S. opioid epidemic continues to pose significant challenges for patients, families, clinicians, and public health policy. Opioids are responsible for an estimated 315,000 deaths (from 1999 to 2016) and have caused 115 deaths per day.1 In 2017, the U.S. Department of Health and Human Services declared the opioid epidemic a public health crisis.2 The total economic burden of opioid abuse in the United States has been estimated to be $78.5 billion per year.3 Although providing care for chronic opioid users is important, equally vital are efforts to prevent so-called opioid-naïve patients (patients with no history of opioid use) from developing regular opioid use, misuse, or abuse. However, much remains unclear regarding what role clinician prescribing habits play and what duration or dose of opioids may safely be prescribed without promoting long-term use.4,5 In 2013, ECRI Institute convened the Partnership for Health IT Patient Safety, and its component, single-topic-focused workgroups followed. For this subject, the Electronic Health Record Association (EHRA): Measures and Clinical Decision Support (CDS) for Safer Opioid Prescribing workgroup included members from the Healthcare Information and Management Systems Society (HIMSS) EHRA and the Partnership team. The project was oriented towards exploring methods to enable a synergistic cycle of performance measurement and identifying electronic health record (EHR)/health information technology (IT)–enabled approaches to support healthcare organizations’ ability to assess and measure opioid prescribing. -
Accurate Prediction of Terahertz Spectra of Molecular Crystals of Fentanyl and Its Analogs Chun‑Hung Wang1, Anthony C
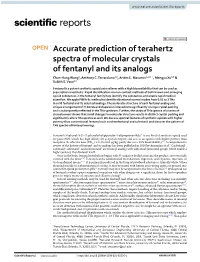
www.nature.com/scientificreports OPEN Accurate prediction of terahertz spectra of molecular crystals of fentanyl and its analogs Chun‑Hung Wang1, Anthony C. Terracciano2,3, Artёm E. Masunov1,4,5*, Mengyu Xu3,6 & Subith S. Vasu2,3 Fentanyl is a potent synthetic opioid pain reliever with a high bioavailability that can be used as prescription anesthetic. Rapid identifcation via non‑contact methods of both known and emerging opioid substances in the fentanyl family help identify the substances and enable rapid medical attention. We apply PBEh‑3c method to identify vibrational normal modes from 0.01 to 3 THz in solid fentanyl and its selected analogs. The molecular structure of each fentanyl analog and unique arrangement of H‑bonds and dispersion interactions signifcantly change crystal packing and is subsequently refected in the THz spectrum. Further, the study of THz spectra of a series of stereoisomers shows that small changes in molecular structure results in distinct crystal packing and signifcantly alters THz spectra as well. We discuss spectral features of synthetic opioids with higher potency than conventional fentanyl such as ohmefentanyl and sufentanil and discover the pattern of THz spectra of fentanyl analogs. Fentanyl (N-phenyl-N-[1-(2-phenylethyl)piperidin-4-yl]propionanilide)1 is one kind of synthetic opioid used for pain relief, which has high afnity for μ-opioid receptor and acts as an agonist with higher potency than 2,3 morphine. Its efective dose (ED 95) is 0.45–0.60 μg/kg, partly due to its 92% bioavailability . A comprehensive review of the history of fentanyl and its analogs has been published in 2018 by Armenian et al.4 Carfentanil5, sufentanil6, alfentanil7, and remifentanil8 are fentanyl analogs with additional functional groups which enable a higher potency than fentanyl itself. -

Values of Several Opioid Receptor Agonists and Their Liability to Cause Depen- Dence
Acta Pharmacologica Sinica (2010) 31: 393–398 npg © 2010 CPS and SIMM All rights reserved 1671-4083/10 $32.00 www.nature.com/aps Original Article Paradoxical relationship between RAVE (relative activity versus endocytosis) values of several opioid receptor agonists and their liability to cause depen- dence Yu-hua WANG1, 2, 3, Jian-feng SUN3, Yi-min TAO3, Xue-jun XU3, Zhi-qiang CHI3, Jing-gen LIU3, * 1School of Pharmacy, China Pharmaceutical University, Nanjing 210009, China; 2School of Pharmacy, Nanjing University of Chinese Medicine, Nanjing 210046, China; 3State Key Laboratory of Drug Research, Shanghai Institute of Materia Medica, Shanghai Institutes for Biological Sciences, Chinese Academy of Sciences, Shanghai 201203, China Aim: To examine the relationship between the RAVE (relative activity versus endocytosis) values of opiate agonists and their dependence liability by studying several potent analgesics with special profiles in the development of physical and psychological dependence. Methods: The effects of (–)-cis-(3R,4S,2′R) ohmefentanyl (F9202), (+)-cis-(3R,4S,2′S) ohmefentanyl (F9204), dihydroetorphine (DHE) and morphine on [35S]GTPγS binding, forskolin-stimulated cAMP accumulation, and receptor internalization were studied in CHO cells stably expressing HA-tagged μ-opioid receptors (CHO-HA-MOR). cAMP overshoot in response to the withdrawal of these compound treatments was also tested. Results: All four agonists exhibited the same rank order of activity in stimulation of [35S]GTPγS binding, inhibition of adenylyl cyclase (AC) and induction of receptor internalization: DHE>F9204>F9202>morphine. Based on these findings and the previous in vivo analgesic data obtained from our and other laboratories, the RAVE values of the four agonists were calculated. -

NIDA Drug Supply Program Catalog, 25Th Edition
RESEARCH RESOURCES DRUG SUPPLY PROGRAM CATALOG 25TH EDITION MAY 2016 CHEMISTRY AND PHARMACEUTICS BRANCH DIVISION OF THERAPEUTICS AND MEDICAL CONSEQUENCES NATIONAL INSTITUTE ON DRUG ABUSE NATIONAL INSTITUTES OF HEALTH DEPARTMENT OF HEALTH AND HUMAN SERVICES 6001 EXECUTIVE BOULEVARD ROCKVILLE, MARYLAND 20852 160524 On the cover: CPK rendering of nalfurafine. TABLE OF CONTENTS A. Introduction ................................................................................................1 B. NIDA Drug Supply Program (DSP) Ordering Guidelines ..........................3 C. Drug Request Checklist .............................................................................8 D. Sample DEA Order Form 222 ....................................................................9 E. Supply & Analysis of Standard Solutions of Δ9-THC ..............................10 F. Alternate Sources for Peptides ...............................................................11 G. Instructions for Analytical Services .........................................................12 H. X-Ray Diffraction Analysis of Compounds .............................................13 I. Nicotine Research Cigarettes Drug Supply Program .............................16 J. Ordering Guidelines for Nicotine Research Cigarettes (NRCs)..............18 K. Ordering Guidelines for Marijuana and Marijuana Cigarettes ................21 L. Important Addresses, Telephone & Fax Numbers ..................................24 M. Available Drugs, Compounds, and Dosage Forms ..............................25 -

List of Narcotic Substances Circulation of Which Is Restricted in Uzbekistan
List of narcotic substances circulation of which is restricted in Uzbekistan 1. 2C-B(4-bromo-2,5-dimethoxyphenethylamine) 2. 3-methylfentanyl 3. 3-methylthiofentanyl 4. 3-Monoacetylmorphine 5. 4-methylaminorex 6. 6- Monoacetylmorphine 7. Acetorphine 8. Acetyl Dihydrocodeine 9. Acetyl-alfametilfentanil 10. Acetylated opium 11. Acetylcodeine 12. Acetylmethadol 13. Alfametadol 14. Alfatsetilmetadol 15. all fungi that contain Psilocine and Psilocybine 16. Allylprodine 17. Alpha Methylfentanyl 18. Alpha Metiltiofentanil 19. Alphaprodine 20. Anileridin 21. Benzethidine 22. Benzylmorphine 23. Betacetylmethadol 24. Betahydroxyfentanyl 25. Betameprodine 26. Betamethadol 27. Betaprodine 28. Bezitramide 29. Cannabis oil (hashish oil) 30. Cannabis, marihuana 31. Cathine ((+)-norpseudoephedrine) 32. Cathinone (l-alpha-aminopropiofenon) 33. Clonitazene 34. Cocaine 35. Codoxime 36. d- Methadone 37. DB [L-(3,4 - methylenedioxyphenyl) -2 butanamine] 38. Desmethylprodine; MPPP (1-methyl-4-phenyl-4-propionoxypiperidine) 39. Desomorphine 40. DET (N,N-diethyltryptamine) 41. Dexamphetamine 42. Diampromide 43. Diethyl phosphate 44. Diethylthiambutene 45. Dihydromorphine 46. Dimenoxadol 47. Dimepheptanol 48. Dimethylthiambutene 49. Dioxaphetyl butyrate 50. Diphenoxine 51. Dipipanone 52. DMA (2,5-dimethoxyamphetamine) 53. DMGP (dimetilgeptilpiran) 54. DMT (dimethyltryptamine) 55. DOB (d, L-2,5-dimethoxy-4-bromo-amphetamine) 56. DOC (d, L-2,5-dimethoxy-4-chloro-amphetamine) 57. DOET (2,5-dimethoxy-4-ethylamphetamine) 58. Drotebanol 59. Ecgonine 60. Ephedrone 61. Ethylmethylthiambutene 62. Eticyclidine 63. Etonitazene 64. Etorphine 65. Etoxeridine 66. Etryptamine 67. Furethidine 68. Hashish (Anasha, cannabis resin) 69. Heroin (Diacetylmorphine) 70. Hydrocodone 71. Hydrocodone phosphate 72. Hydromorphinol 73. Hydromorphone 74. Isomethadone 75. Ketobemidone 76. Khat 77. L- Methadone 78. Levomethorphan 79. Levomoramide 80. Levophenacylmorphan 81. Levorphanol 82. Lysergic acid and its preparations, that include d-Lysergide (LSD, LSD-25) 83. -

Screening for New Psychoactive Substances (NPS) Without Reference Standards on High Resolution Mass Spectrometers (HR-MS)
UNIVERSIDADE DE LISBOA FACULDADE DE CIÊNCIAS DEPARTAMENTO DE QUÍMICA E BIOQUÍMICA Screening for New Psychoactive Substances (NPS) without reference standards on High Resolution Mass Spectrometers (HR-MS) Maria Estevão Fidalgo von Cüpper Mestrado em Química Especialização em Química Dissertação orientada por: Professor Dr. Med. Kristian Linnet Dra. Helena Galla Gaspar 2019 “We must have perseverance and above all confidence in ourselves. We must be- lieve that we are gifted for something and that this thing must be attained.” Marie Curie ii ACKNOWLEDGMENTS This master’s thesis represents the culmination of an important stage in my academic life. Thanks to the Erasmus Traineeship Programme, I had the opportunity to take two semesters abroad and venture into the world of forensics, a field that I have always been passionate about. The project was carried out at the Sec- tion of Forensic Chemistry at the Department of Forensic Medicine, University of Copenhagen, Denmark. First of all, I would like to thank Prof. Dr. Med. Kristian Linnet, for giving me the possibility to do this research within the Forensic Chemistry field at the Institute. I would like to express my sincere gratitude to Dr. Petur Dalsgaard, my external supervisor who intro- duced me to the world of New Psychoactive Substances (NPS) and high-resolution mass spectrometry, for his willingness to offer a stimulating environment, continuous support in the development of my thesis, his patience, motivation, immense knowledge, and for providing me with practical tips. I am very grateful to my internal supervisor Dr. Helena Gaspar, who initially guided my enthusiasm to work with NPS. -

Fentanyl Family at the Mu-Opioid Receptor: Uniform Assessment of Binding and Computational Analysis
molecules Article Fentanyl Family at the Mu-Opioid Receptor: Uniform Assessment of Binding and Computational Analysis Piotr F. J. Lipi ´nski 1,* , Piotr Kosson 2, Joanna Matali ´nska 1, Piotr Roszkowski 3, Zbigniew Czarnocki 3, Małgorzata Jaro ´nczyk 4 , Aleksandra Misicka 1,3 , Jan Cz. Dobrowolski 4 and Joanna Sadlej 4,5,* 1 Department of Neuropeptides, Mossakowski Medical Research Centre, Polish Academy of Sciences, 02-106 Warsaw, Poland; [email protected] (J.M.); [email protected] (A.M.) 2 Toxicology Research Laboratory, Mossakowski Medical Research Centre, Polish Academy of Sciences, 02-106 Warsaw, Poland; [email protected] 3 Faculty of Chemistry, University of Warsaw, 02-093 Warsaw, Poland; [email protected] (P.R.); [email protected] (Z.C.); [email protected] (A.M.) 4 National Medicines Institute, 00-725 Warsaw, Poland; [email protected] (M.J.); [email protected] (J.Cz.D.) 5 Faculty of Mathematics and Natural Sciences, University of Cardinal Stefan Wyszy´nski,1/3 Wóycickiego-Str., 01-938 Warsaw, Poland * Correspondence: [email protected] (P.F.J.L.); [email protected] (J.S.) Received: 30 January 2019; Accepted: 15 February 2019; Published: 19 February 2019 Abstract: Interactions of 21 fentanyl derivatives with µ-opioid receptor (µOR) were studied using experimental and theoretical methods. Their binding to µOR was assessed with radioligand competitive binding assay. A uniform set of binding affinity data contains values for two novel and one previously uncharacterized derivative. The data confirms trends known so far and thanks to their uniformity, they facilitate further comparisons. -
Maternal Deprivation Increases Vulnerability to Morphine Dependence and Disturbs the Enkephalinergic System in Adulthood
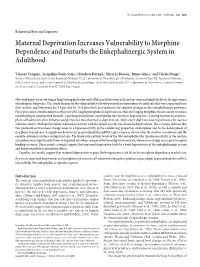
The Journal of Neuroscience, May 4, 2005 • 25(18):4453–4462 • 4453 Behavioral/Systems/Cognitive Maternal Deprivation Increases Vulnerability to Morphine Dependence and Disturbs the Enkephalinergic System in Adulthood Vincent Vazquez,1 Jacqueline Penit-Soria,2 Claudette Durand,2 Marie Jo Besson,2 Bruno Giros,1 and Vale´rie Dauge´1 1Institut National de la Sante´ et de la Recherche Me´dicale, U513, Laboratoire de Neurobiologie et Psychiatrie, Universite´ Paris XII, Faculte´deMe´decine, 94010 Cre´teil, France, and 2Centre National de la Recherche Scientifique, Unite´ Mixte de Recherche 7624, Laboratoire de Neurochimie Anatomie Institut des Neurosciences, Universite´ ParisVI, 75005 Paris, France Maternal deprivation can trigger long-lasting molecular and cellular modifications in brain functions and might facilitate the appearance of pathogenic behaviors. This study focuses on the vulnerability to develop morphine dependence in adult rats that were separated from their mother and littermates for 3 h per day for 14 d after birth and examines the adaptive changes in the enkephalinergic pathways. Place-preference conditioning was observed with 2 mg/kg morphine in deprived rats, whereas 5 mg/kg morphine was necessary to induce conditioning in nondeprived animals. A prolonged morphine conditioning was shown in deprived rats. A strong increase in oral mor- phine self-administration behavior and preference was observed in deprived rats. Only a very slight increase in preference for sucrose solution, a more ethological reinforcer known to interact with the opioid system, was shown in deprived rats. These results indicate that this postnatal environment change leads to a hypersensitivity to the reinforcing properties of morphine and to the development of morphine dependence. -

WO 2014/006004 Al 9 January 2014 (09.01.2014) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2014/006004 Al 9 January 2014 (09.01.2014) P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 9/20 (2006.01) A61K 31/485 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, (21) International Application Number: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, PCT/EP2013/06385 1 DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IS, JP, KE, KG, KN, KP, KR, 1 July 20 13 (01 .07.2013) KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, (25) Filing Language: English OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SC, (26) Publication Language: English SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. (30) Priority Data: PA 2012 70405 6 July 2012 (06.07.2012) DK (84) Designated States (unless otherwise indicated, for every 61/668,741 6 July 2012 (06.07.2012) US kind of regional protection available): ARIPO (BW, GH, GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, SZ, TZ, (71) Applicant: EGALET LTD. -
Fentanyl Crisis in the United States Was the Result of Fentanyl Being Mixed Into Heroin and Distributed to Unsuspecting Heroin Users
William S. Jacobs, MD Chief of Addiction Medicine Medical College of Georgia Medical Director Bluff Plantation Heroin and Synthetic Opioids Thursday, April 6, 2017 9:15 am – 9:40 am Disclosure Information William S. Jacobs, MD No disclosures The 2006 fentanyl crisis in the United States was the result of fentanyl being mixed into heroin and distributed to unsuspecting heroin users. The 2006 fentanyl crisis was fueled by a single clandestine laboratory in Toluca, Mexico, and once the laboratory was seized, the seizures of fentanyl and overdose deaths in the United States suddenly tapered off. During the current fentanyl crisis (2013-present), traffickers have not only used similar historical production and distribution techniques, but have also expanded the fentanyl market by producing wholesale quantities of counterfeit prescription medications containing various fentanyls. The current fentanyl crisis is fueled by China-sourced fentanyls and fentanyl precursor chemicals that are being sold to various individuals and organizations responsible for fentanyl processing and distribution operations; this scenario includes individuals linked to Mexican cartels and other criminal organizations that are not affiliated with Mexican cartels. The seizures of fentanyl-laced pills and clandestine pill press operations all across North America indicate that this is becoming a trend, not a series of isolated incidents. Source: Wikipedia https://ndews.umd.edu/sites/ndews. umd.edu/files/u1486/dea_emerging _threat_report_2016_quarter_4.pdf https://www.dea.gov/docs/Counterfeit%20Prescription%20Pills.pdf May 2015 - Chinese Customs officials seized 46 kilograms of fentanyl and 26 kilograms of acetyl fentanyl hidden in a cargo container destined for Mexico. Six customs officials became ill and one fell into a coma as a result of handling the fentanyls.