Toxicological Profile for Chloromethane
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Hydrogen and Carbon Isotope Fractionation During Degradation Of
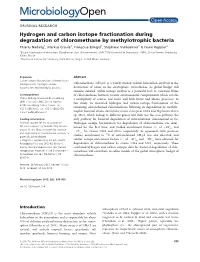
ORIGINAL RESEARCH Hydrogen and carbon isotope fractionation during degradation of chloromethane by methylotrophic bacteria Thierry Nadalig1, Markus Greule2, Francßoise Bringel1,Stephane Vuilleumier1 & Frank Keppler2 1Equipe Adaptations et Interactions Microbiennes dans l’Environnement, UMR 7156 Universite de Strasbourg - CNRS, 28 rue Goethe, Strasbourg, 67083, France 2Max Planck Institute for Chemistry, Hahn-Meitner-Weg 1, 55128 Mainz, Germany Keywords Abstract Carbon isotope fractionation, chloromethane biodegradation, hydrogen isotope Chloromethane (CH3Cl) is a widely studied volatile halocarbon involved in the fractionation, methylotrophic bacteria. destruction of ozone in the stratosphere. Nevertheless, its global budget still remains debated. Stable isotope analysis is a powerful tool to constrain fluxes Correspondence of chloromethane between various environmental compartments which involve Thierry Nadalig, Universite de Strasbourg, a multiplicity of sources and sinks, and both biotic and abiotic processes. In UMR 7156 UdS-CNRS, 28 rue Goethe, this study, we measured hydrogen and carbon isotope fractionation of the 67083 Strasbourg Cedex, France. Tel: +33 3 68851973; Fax: +33 3 68852028; remaining untransformed chloromethane following its degradation by methylo- Methylobacterium extorquens Hyphomicrobium E-mail: [email protected] trophic bacterial strains CM4 and sp. MC1, which belong to different genera but both use the cmu pathway, the Funding Information only pathway for bacterial degradation of chloromethane characterized so far. Financial support for the acquisition of Hydrogen isotope fractionation for degradation of chloromethane was deter- GC-FID equipment by REALISE (http://realise. mined for the first time, and yielded enrichment factors (e)ofÀ29& and unistra.fr), the Alsace network for research À27& for strains CM4 and MC1, respectively. In agreement with previous and engineering in environmental sciences, is studies, enrichment in 13C of untransformed CH Cl was also observed, and gratefully acknowledged. -

Catalytic Conversion of Chloromethane to Methanol and Dimethyl Ether Over Two Catalytic Beds: a Study of Acid Strength
BRAZILIAN JOURNAL OF PETROLEUM AND GAS | v. 4 n. 3 | p. 083-089 | 2010 | ISSN 1982-0593 CATALYTIC CONVERSION OF CHLOROMETHANE TO METHANOL AND DIMETHYL ETHER OVER TWO CATALYTIC BEDS: A STUDY OF ACID STRENGTH a a a 1 Fernandes, D. R.; Leite, T. C. M., Mota, C. J. A. a Universidade Federal do Rio de Janeiro, Instituto de Química ABSTRACT The catalytic hydrolysis of chloromethane to methanol and dimethyl ether (DME) was studied over metal- exchanged Beta and Mordenite zeolites, acidic MCM-22 and SAPO-5. The use of a second catalytic bed with HZSM-5 zeolite increased the selectivity to DME, due to methanol dehydration on the acid sites. The effect was more significant on catalysts presenting medium and weak acid site distribution, showing that dehydration of methanol to DME is accomplished over sites of higher acid strength. KEYWORDS natural gas conversion; chloromethane; zeolites; methanol; dimethyl ether 1 To whom all correspondence should be addressed. Address: Universidade Federal do Rio de Janeiro, Instituto de Química. Av Athos da Silveira Ramos 149, CT Bloco A, 21941-909, Rio de Janeiro, Brazil |e-mail: [email protected] doi:10.5419/bjpg2010-0009 83 BRAZILIAN JOURNAL OF PETROLEUM AND GAS | v. 4 n. 3 | p. 083-089 | 2010 | ISSN 1982-0593 1. INTRODUCTION derivatives, either through direct reaction of natural gas with the halogens, or through The production of methanol and dimethyl ether oxyhalogenation processes, using HCl or HBr and (DME) from natural gas has been the subject of air. In addition, the electrophilic halogenation of great industrial interest. These oxygenates have methane can be performed with the use of Lewis high commercial value, because they can be used acid catalysts, yielding monohalomethane as liquid fuels and raw material for petrochemicals. -

Methanol Consumption Drives the Bacterial Chloromethane Sink in a Forest Soil
The ISME Journal (2018) 12:2681–2693 https://doi.org/10.1038/s41396-018-0228-4 ARTICLE Methanol consumption drives the bacterial chloromethane sink in a forest soil 1,2 2 1,4 3 1 Pauline Chaignaud ● Mareen Morawe ● Ludovic Besaury ● Eileen Kröber ● Stéphane Vuilleumier ● 1 3 Françoise Bringel ● Steffen Kolb Received: 16 February 2018 / Revised: 1 June 2018 / Accepted: 15 June 2018 / Published online: 10 July 2018 © The Author(s) 2018. This article is published with open access Abstract Halogenated volatile organic compounds (VOCs) emitted by terrestrial ecosystems, such as chloromethane (CH3Cl), have pronounced effects on troposphere and stratosphere chemistry and climate. The magnitude of the global CH3Cl sink is uncertain since it involves a largely uncharacterized microbial sink. CH3Cl represents a growth substrate for some specialized methylotrophs, while methanol (CH3OH), formed in much larger amounts in terrestrial environments, may be more widely used by such microorganisms. Direct measurements of CH3Cl degradation rates in two field campaigns and in microcosms allowed the identification of top soil horizons (i.e., organic plus mineral A horizon) as the major biotic sink in a fi 1234567890();,: 1234567890();,: deciduous forest. Metabolically active members of Alphaproteobacteria and Actinobacteria were identi ed by taxonomic and functional gene biomarkers following stable isotope labeling (SIP) of microcosms with CH3Cl and CH3OH, added alone 13 or together as the [ C]-isotopologue. Well-studied reference CH3Cl degraders, such as Methylobacterium extorquens CM4, were not involved in the sink activity of the studied soil. Nonetheless, only sequences of the cmuA chloromethane dehalogenase gene highly similar to those of known strains were detected, suggesting the relevance of horizontal gene transfer for CH3Cl degradation in forest soil. -
List of Lists
United States Office of Solid Waste EPA 550-B-10-001 Environmental Protection and Emergency Response May 2010 Agency www.epa.gov/emergencies LIST OF LISTS Consolidated List of Chemicals Subject to the Emergency Planning and Community Right- To-Know Act (EPCRA), Comprehensive Environmental Response, Compensation and Liability Act (CERCLA) and Section 112(r) of the Clean Air Act • EPCRA Section 302 Extremely Hazardous Substances • CERCLA Hazardous Substances • EPCRA Section 313 Toxic Chemicals • CAA 112(r) Regulated Chemicals For Accidental Release Prevention Office of Emergency Management This page intentionally left blank. TABLE OF CONTENTS Page Introduction................................................................................................................................................ i List of Lists – Conslidated List of Chemicals (by CAS #) Subject to the Emergency Planning and Community Right-to-Know Act (EPCRA), Comprehensive Environmental Response, Compensation and Liability Act (CERCLA) and Section 112(r) of the Clean Air Act ................................................. 1 Appendix A: Alphabetical Listing of Consolidated List ..................................................................... A-1 Appendix B: Radionuclides Listed Under CERCLA .......................................................................... B-1 Appendix C: RCRA Waste Streams and Unlisted Hazardous Wastes................................................ C-1 This page intentionally left blank. LIST OF LISTS Consolidated List of Chemicals -

Downloaded from Genbank
Methylotrophs and Methylotroph Populations for Chloromethane Degradation Françoise Bringel1*, Ludovic Besaury2, Pierre Amato3, Eileen Kröber4, Stefen Kolb4, Frank Keppler5,6, Stéphane Vuilleumier1 and Thierry Nadalig1 1Université de Strasbourg UMR 7156 UNISTR CNRS, Molecular Genetics, Genomics, Microbiology (GMGM), Strasbourg, France. 2Université de Reims Champagne-Ardenne, Chaire AFERE, INR, FARE UMR A614, Reims, France. 3 Université Clermont Auvergne, CNRS, SIGMA Clermont, ICCF, Clermont-Ferrand, France. 4Microbial Biogeochemistry, Research Area Landscape Functioning – Leibniz Centre for Agricultural Landscape Research – ZALF, Müncheberg, Germany. 5Institute of Earth Sciences, Heidelberg University, Heidelberg, Germany. 6Heidelberg Center for the Environment HCE, Heidelberg University, Heidelberg, Germany. *Correspondence: [email protected] htps://doi.org/10.21775/cimb.033.149 Abstract characterized ‘chloromethane utilization’ (cmu) Chloromethane is a halogenated volatile organic pathway, so far. Tis pathway may not be representa- compound, produced in large quantities by terres- tive of chloromethane-utilizing populations in the trial vegetation. Afer its release to the troposphere environment as cmu genes are rare in metagenomes. and transport to the stratosphere, its photolysis con- Recently, combined ‘omics’ biological approaches tributes to the degradation of stratospheric ozone. A with chloromethane carbon and hydrogen stable beter knowledge of chloromethane sources (pro- isotope fractionation measurements in microcosms, duction) and sinks (degradation) is a prerequisite indicated that microorganisms in soils and the phyl- to estimate its atmospheric budget in the context of losphere (plant aerial parts) represent major sinks global warming. Te degradation of chloromethane of chloromethane in contrast to more recently by methylotrophic communities in terrestrial envi- recognized microbe-inhabited environments, such ronments is a major underestimated chloromethane as clouds. -

4. Production, Import/Export, Use, and Disposal
CHLOROMETHANE 149 4. PRODUCTION, IMPORT/EXPORT, USE, AND DISPOSAL 4.1 PRODUCTION Table 4-1 lists the facilities in each state that manufacture or process chloromethane, the intended use, and the range of maximum amounts of chloromethane that are stored on site. The data listed in Table 4-l are derived from the Toxics Release Inventory (TRI96 1998). Only certain types of facilities were required to report. Therefore, this is not an exhaustive list. Based on the most current TRI information, there are currently 96 facilities that produce or process chloromethane in the United States. Chloromethane (also commonly known as methyl chloride) is both an anthropogenic and naturally occurring chemical. Anthropogenic sources include industrial production, polyvinyl chloride burning, and wood burning; natural sources include the oceans, microbial fermentation, and biomass fires (e.g., forest fires, grass fires). Chloromethane is produced industrially by reaction of methanol and hydrogen chloride (HCl) or by chlorination of methane (Edwards et al. 1982a; Holbrook 1992; Key et al. 1980). While the reaction of methanol with HCl is the most common method, the choice of process depends, in part, on the HCl balance at the site (the methane route produces HCl, the methanol route uses it) (Edwards et al. 1982a; Holbrook 1992). Typically, manufacturing plants that produce chloromethane also produce higher chlorinated methanes (methylene chloride, chloroform, and carbon tetrachloride). The methanol-HCl process involves combining vapor-phase methanol and HCl at 180-200 °C, followed by passage over a catalyst where the reaction occurs (Holbrook 1992; Key et al. 1980). Catalysts include alumina gel, gamma alumina, and cuprous or zinc chloride on pumice or activated carbon. -

Determination of Chloromethane and Dichloromethane in a Tropical T Terrestrial Mangrove Forest in Brazil by Measurements and Modelling
Atmospheric Environment 173 (2018) 185–197 Contents lists available at ScienceDirect Atmospheric Environment journal homepage: www.elsevier.com/locate/atmosenv Determination of chloromethane and dichloromethane in a tropical T terrestrial mangrove forest in Brazil by measurements and modelling ∗ S.R. Kolusua,c, , K.H. Schlünzena, D. Grawea, R. Seifertb a Meteorological Institute, CEN, University of Hamburg, Hamburg, Germany b Institute for Geology and Marine Chemistry, University of Hamburg, Hamburg, Germany c Department of Geography, School of Global Studies, University of Sussex, Brighton, UK ARTICLE INFO ABSTRACT Keywords: Chloromethane (CH3Cl) and dichloromethane (CH2Cl2) are known to have both natural and anthropogenic Chloromethane sources to the atmosphere. From recent studies it is known that tropical and sub tropical plants are primary Dichloromethane sources of CH3Cl in the atmosphere. In order to quantify the biogenic emissions of CH3Cl and CH2Cl2 from Mangrove mangroves, field measurement were conducted in a tropical mangrove forest on the coast of Brazil. To the best of Emission our knowledge these field measurements were the first of its kind conducted in the tropical mangrove ecosystem METRAS of Braganca. A mesoscale atmospheric model, MEsoscale TRAnsport and fluid (Stream) model (METRAS), was used to simulate passive tracers concentrations and to study the dependency of concentrations on type of emission function and meteorology. Model simulated concentrations were normalized using the observed field data. With the help of the mesoscale model results and the observed data the mangrove emissions were estimated at the local scale. By using this bottom-up approach the global emissions of CH3Cl and CH2Cl2 from mangroves were quantified. The emission range obtained with different emission functions and different meteorology are −1 4–7Ggyr for CH3Cl and 1–2Ggyr2 for CH2Cl2. -

Locating and Estimating Air Emissions from Sources of Chloroform
United States Office of Air Quality EPA-450/4-84-007c Environmental Protection Planning And Standards Agency Research Triangle Park, NC 27711 March 1984 AIR EPA LOCATING AND ESTIMATING AIR EMISSIONS FROM SOURCES OF CHLOROFORM L &E EPA- 450/4-84-007c March 1984 LOCATING & ESTIMATING AIR EMISSIONS FROM SOURCES OF CHLOROFORM U.S. ENVIRONMENTAL PROTECTION AGENCY Office of Air and Radiation Office of Air Quality Planning and Standards Research Triangle Park, North Carolina 27711 This report has been reviewed by the Office Of Air Quality Planning And Standards, U.S. Environmental Protection Agency, and has been approved for publication as received from GCA Technology. Approval does not signify that the contents necessarily reflect the views and policies of the Agency, neither does mention of trade names or commercial products constitute endorsement or recommendation for use. ii CONTENTS Figures ...................... iv Tables ...................... v 1. Purpose of Document ............... 1 2. Overview of Document Contents .......... 3 3. Background .................... 5 Nature of Pollutant ............ 5 Overview of Production and Uses ...... 8 4. Chloroform Emission Sources ........... 11 Chloroform Production ........... 11 Fluorocarbon Production .......... 20 Pharmaceutical Manufacturing ........ 26 Ethylene Dichloride Production ....... 29 Perchloroethylene and Trichloroethylene Production . ............. 38 Chlorination of Organic Precursors in Water. 44 Miscellaneous Chloroform Emission Sources . 61 5. Source Test Procedures ............... 63 References 66 Appendix - Derivation of Emission Factors from Chloroform Production .................... A-1 References for Appendix ............... A-23 iii FIGURES Number Page 1 Chemical use tree for chloroform ............ 10 2 Basic operations that may be used in the methanol hydrochlorination/methyl chloride chlorination process 12 3 Basic operations that may be used in the methane chlorination process ................ -

DOI: 10.1126/Science.1238937 , (2013); 341 Science Et Al. L. A
Volatile, Isotope, and Organic Analysis of Martian Fines with the Mars Curiosity Rover L. A. Leshin et al. Science 341, (2013); DOI: 10.1126/science.1238937 This copy is for your personal, non-commercial use only. If you wish to distribute this article to others, you can order high-quality copies for your colleagues, clients, or customers by clicking here. Permission to republish or repurpose articles or portions of articles can be obtained by following the guidelines here. The following resources related to this article are available online at www.sciencemag.org (this information is current as of September 27, 2013 ): Updated information and services, including high-resolution figures, can be found in the online version of this article at: http://www.sciencemag.org/content/341/6153/1238937.full.html on September 27, 2013 Supporting Online Material can be found at: http://www.sciencemag.org/content/suppl/2013/09/25/341.6153.1238937.DC1.html http://www.sciencemag.org/content/suppl/2013/09/26/341.6153.1238937.DC2.html A list of selected additional articles on the Science Web sites related to this article can be found at: http://www.sciencemag.org/content/341/6153/1238937.full.html#related This article cites 43 articles, 9 of which can be accessed free: www.sciencemag.org http://www.sciencemag.org/content/341/6153/1238937.full.html#ref-list-1 This article has been cited by 3 articles hosted by HighWire Press; see: http://www.sciencemag.org/content/341/6153/1238937.full.html#related-urls Downloaded from Science (print ISSN 0036-8075; online ISSN 1095-9203) is published weekly, except the last week in December, by the American Association for the Advancement of Science, 1200 New York Avenue NW, Washington, DC 20005. -

Evidence for a Major Missing Source in the Global Chloromethane Budget from Stable Carbon Isotopes
Atmos. Chem. Phys., 19, 1703–1719, 2019 https://doi.org/10.5194/acp-19-1703-2019 © Author(s) 2019. This work is distributed under the Creative Commons Attribution 4.0 License. Evidence for a major missing source in the global chloromethane budget from stable carbon isotopes Enno Bahlmann1,2, Frank Keppler3,4,5, Julian Wittmer6,7, Markus Greule3,4, Heinz Friedrich Schöler3, Richard Seifert1, and Cornelius Zetzsch5,6 1Institute of Geology, University Hamburg, Bundesstrasse 55, 20146 Hamburg, Germany 2Leibniz Centre for Tropical Marine Research, Fahrenheitstraße 6, 28359 Bremen, Germany 3Institute of Earth Sciences, Heidelberg University, Im Neuenheimer Feld 234–236, 69120 Heidelberg, Germany 4Heidelberg Center for the Environment (HCE), Heidelberg University, 69120 Heidelberg, Germany 5Max-Planck-Institute for Chemistry, Hahn-Meitner-Weg 1, 55128 Mainz, Germany 6Atmospheric Chemistry Research Unit, BayCEER, University of Bayreuth, Dr Hans-Frisch Strasse 1–3, 95448 Bayreuth, Germany 7Agilent Technologies Sales & Services GmbH & Co. KG, Hewlett-Packard-Str. 8, 76337 Waldbronn, Germany Correspondence: Enno Bahlmann ([email protected]) Received: 17 August 2018 – Discussion started: 11 September 201 Revised: 17 January 2019 – Accepted: 18 January 2019 – Published: 8 February 2019 Abstract. Chloromethane (CH3Cl) is the most important with the OH-driven seasonal cycle in tropospheric mixing ra- natural input of reactive chlorine to the stratosphere, con- tios. tributing about 16 % to stratospheric ozone depletion. Due Applying these new values for the carbon isotope effect to the phase-out of anthropogenic emissions of chlorofluoro- to the global CH3Cl budget using a simple two hemispheric carbons, CH3Cl will largely control future levels of strato- box model, we derive a tropical rainforest CH3Cl source spheric chlorine. -

SAFETY DATA SHEET Methyl Chloride (R40) Issue Date: 16.01.2013 Version: 1.0 SDS No.: 000010021780 Revision Date: 15.10.2013 1/15
SAFETY DATA SHEET Methyl chloride (R40) Issue date: 16.01.2013 Version: 1.0 SDS No.: 000010021780 Revision date: 15.10.2013 1/15 SECTION 1: Identification of the substance/mixture and of the company/undertaking 1.1 Product identifier Product name: Methyl chloride (R40) Trade name: Methyl Chloride Grade N3.0 Additional identification Chemical name: chloromethane; methyl chloride Chemical formula: CH3Cl INDEX No. 602-001-00-7 CAS-No. 74-87-3 EC No. 200-817-4 REACH Registration No. 01-2119493708-22 1.2 Relevant identified uses of the substance or mixture and uses advised against Identified uses: Industrial and professional. Perform risk assessment prior to use. Degreasing. Using gas alone or in mixtures for the calibration of analysis equipment. Using gas as feedstock in chemical processes. Formulation of mixtures with gas in pressure receptacles. Uses advised against Consumer use. 1.3 Details of the supplier of the safety data sheet Supplier BOC Telephone: 0800 111 333 Priestley Road, Worsley M28 2UT Manchester E-Mail: [email protected] 1.4 Emergency telephone number: 0800 111 333 SECTION 2: Hazards identification 2.1 Classification of the substance or mixture Classification according to Directive 67/548/EEC or 1999/45/EC as amended F+; R12 Carc. 3; R40 Xn; R48/20 The full text for all R-phrases is displayed in section 16. Classification according to Regulation (EC) No 1272/2008 as amended Physical hazards Flammable gas Category 1 H220: Extremely flammable gas. Gases under pressure Liquefied gas H280: Contains gas under pressure; may explode if heated. SDS_GB - 000010021780 SAFETY DATA SHEET Methyl chloride (R40) Issue date: 16.01.2013 Version: 1.0 SDS No.: 000010021780 Revision date: 15.10.2013 2/15 Health hazards Carcinogenicity Category 2 H351: Suspected of causing cancer. -
Methyl Chloride Handbook
METHYL CHLORIDE HANDBOOK OXYCHEM TECHNICAL INFORMATION 11/2014 Dallas-based Occidental Chemical Corporation is a leading North American manufacturer of basic chemicals, vinyls and performance chemicals directly and through various affiliates (collectively, OxyChem). OxyChem is also North America's largest producer of sodium chlorite. As a Responsible Care® company, OxyChem's global commitment to safety and the environment goes well beyond compliance. OxyChem's Health, Environment and Safety philosophy is a positive motivational force for our employees, and helps create a strong culture for protecting human health and the environment. Our risk management programs and methods have been, and continue to be, recognized as some of the industry's best. OxyChem offers an effective combination of industry expertise, experience, on line business tools, quality products and exceptional customer service. As a member of the Occidental Petroleum Corporation family, OxyChem represents a rich history of experience, top-notch business acumen, and sound, ethical business practices. Table of Contents Page Introduction to Methyl Chloride ................................................................................................................... 3 Manufacturing .................................................................................................................................................. 3 Methyl Chloride — Uses .................................................................................................................................