The Meeting of Meditative Disciplines and Western Psychology: a Mutually Enriching Dialogue
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2004 Psychotherapy Bulletin, Volume 39, Number 3
B Psychotherapy OFFICIAL PUBLICATION OF DIVISION 29 OF THE AMERICAN PSYCHOLOGICAL ASSOCIATION www.divisionofpsychotherapy.org U In This Issue L Polarities and Synthesis Psychology as Psychology L An Outstanding Return E To Cross or Not to Cross T Candidates for APA President E O I C N VOLUME 39 NO. 3 SUMMER 2004 Division of Psychotherapy Ⅲ 2004 Governance Structure ELECTED BOARD MEMBERS President Past President Alice Rubenstein, Ed.D., 2004-2006 Linda F. Campbell, Ph.D. Patricia M. Bricklin, Ph.D. Monroe Psychotherapy Center University of Georgia 470 Gen. Washington Road 20 Office Park Way 402 Aderhold Hall Wayne, PA 19087 Pittsford, NY 14534 Athens, GA 30602-7142 Ofc: 610-499-1212 Fax: 610-499-4625 Ofc: 585-586-0410 Fax: 585-586-2029 Ofc: 706-542-8508 Fax: 770-594-9441 Email: [email protected] Email: [email protected] E-Mail: [email protected] Board of Directors Members-at-Large Sylvia Shellenberger, Ph.D., 2002-2004 President-elect Norman Abeles, Ph.D. , 2003-2005 3780 Eisenhower Parkway Leon VandeCreek, Ph.D. Michigan State University Macon, GA 31206 The Ellis Institute Dept. of Psychology Ofc: 478-784-3580 Fax: 478-784-3550 9 N. Edwin G. Moses Blvd. E. Lansing, MI 48824-1117 Email: [email protected] Dayton, OH 45407 Ofc: 517-355-9564 Fax: 517-353-5437 Ofc: 937-775-4334 Fax: 937-775-4323 Email: [email protected] APA Council Representatives E-Mail: [email protected] Mathilda B. Canter, Ph.D., 2002-2004 John C. Norcross, Ph.D., 2002-2004 4035 E. McDonald Drive Department of Psychology Secretary Phoenix, AZ 85018 University of Scranton Abraham W. -

T~~E Evolution of Psychotherapy. a Conference
T~~E EvoluTioN of PsycHOTHERApy. SM A CoNfERENCE. Sponsored by The Milton H. Erickson Foundation Cosponsored by University of California, Irvine-Department of Psychiatry & Human Behavior California State University, Fullerton-Department of Psychology December 12-16, 1990 Anaheim, California FEATURING: Beck, Bugental, Ellis, Glasser, M. Goulding, Haley, Hillman, Kaplan, Lazarus, Lowen, Madanes, Marmor, Masterson, May, Meichenbaum, Minuchin, Palazzoli, E. Polster, M. Polster, Rossi, Szasz, Watzlawick, Whitaker, Wolpe and Zeig. KEYNOTE ADDRESSES Viktor Frankl Betty Friedan PsycheScapes= Positions & Projections Featuring: Aaron Beck, M.D. James Bugental, Ph.D. Albert Ellis, Ph.D. William Glasser, M.D. Mary Goulding, M.S.W. Jay Haley, M.A. James Hillman, Ph.D. Helen Singer Kaplan, M.D., Ph.D. Arnold Lazarus, Ph.D. Alexander Lowen, M.D. Cloe Madanes, Lie. Psychol. Judd Marmor, M.D., Ph.D. James Masterson, M.D. Rollo May, Ph.D. Donald Meichenbaum, Ph.D. Salvador Minuchin, M.D. Mara Selvini Palazzoli, M.D. Erving Polster, Ph.D. Miriam Polster, Ph.D. Ernest Rossi, Ph.D. Thomas Szasz, M.D. Paul Watzlawick, Ph.D. Carl Whitaker, M.D. Joseph Wolpe, M.D. Jeffrey Zeig, Ph.D. This second Evolution of Psychotherapy Conference, PsycheScapes: Positions and Projections, is dedicated to those presenters from the 1985 Conference who cannot be with us here, but who will always be with us in spirit. Their wisdom and contributions have added to the well-being of humankind. Bruno Bettelheim Murray Bowen Ronald D. Laing Carl Rogers Virginia Satir Lewis Walberg And to Robert Goulding who could not attend the Conference due to ill health. THE HONORABLE CITY COUNCIL FRED HUNTER, Mayor IRV PICKLER, Mayor Pro Tern MIRIAM KAYWOOD, Councilwoman WILLIAM D. -

Long-Term Benefits from Psychotherapy
UC Irvine UC Irvine Previously Published Works Title Long-term benefits from psychotherapy Permalink https://escholarship.org/uc/item/42m0z598 Journal Journal of Humanistic Psychology, 45(4) Authors Walsh, RN Bugental, J Publication Date 2005 License https://creativecommons.org/licenses/by/4.0/ 4.0 Peer reviewed eScholarship.org Powered by the California Digital Library University of California 10.1177/0022167805280266PsychotherapyRoger Walsh, James Benefits Bugental LONG-TERM BENEFITS FROM PSYCHOTHERAPY: A 30-YEAR RETROSPECTIVE BY CLIENT AND THERAPIST ROGER WALSH, M.D., Ph.D., is a professor of psy- chiatry, philosophy, and anthropology and adjunct professor of religious studies at the University of Cal- ifornia, Irvine, where he teaches psychotherapy and conducts research on meditation and related fields. His publications include Paths Beyond Ego, Essential Spirituality: The Seven Central Practices, The Spirit of Shamanism, and Higher Wisdom: Eminent Think- ers Reflect on the Continuing Impact and Implica- tions of Psychedelics. JAMES BUGENTAL, Ph.D., is an existential, humanistically oriented therapist who was the founding president of the Association for Humanistic Psychology.His interests and therapeutic orientation are suggested by the titles of his writings, such as The Search for Authenticity, Psychotherapy and Process: The Fundamentals of an Existential-Humanistic Approach, Intimate Journeys: Stories from Life- Changing Therapy (1990), Psychotherapy Isn’t What You Think (1999), and The Handbook of Humanistic Psychology (with K. Schneider & J. F. Pierson, 2001). This article offers a uniquely long-term examination by a client and therapist, mental health professionals, of their therapeutic work AUTHORS’ NOTE: We would like to thank Frances Vaughan, Irv Yalom,John Levy, and Michael Mahoney for their helpful feedback, Elizabeth Bugental and Bryan Wittine for their support,and Bonnie L’Allier and Michelle Medlock for their admin- istrative and secretarial assistance. -

Theory and Practice of Counseling and Psychotherapy
ninth edition Theory and Practice of Counseling and Psychotherapy GERALD COREY California State University, Fullerton Diplomate in Counseling Psychology American Board of Professional Psychology $XVWUDOLDä%UD]LOä-DSDQä.RUHDä0H[LFRä6LQJDSRUHä6SDLQä8QLWHG.LQJGRPä8QLWHG6WDWHV Copyright 2011 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s). Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it. About the Author GERALD COREY is a Professor Emeritus of Human Serv- ices at California State University at Fullerton and a licensed psychologist. He received his doctorate in counseling from the University of Southern California. He is a Diplomate in Counseling Psychology, American Board of Professional Psychology; a National Certified Counselor; a Fellow of the American Psychological Association (Counseling Psychol- ogy); a Fellow of the American Counseling Association; and Associated Press a Fellow of the Association for Specialists in Group Work. He also holds memberships in the American Group Psycho- therapy Association; the American Mental Health Counselors Association; the As- sociation for Spiritual, Ethical, and Religious Values in Counseling; the Associa- tion for Counselor Education and Supervision; and the Western Association for Coun selor Education and Supervision. Along with Marianne Schneider Corey, Jerry received the Lifetime Achieve- ment Award from the American Mental Health Counselors Association in 2011 and the Eminent Career Award from the Association for Specialists in Group Work in 2001. -
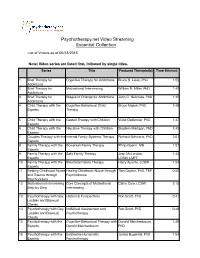
Psychotherapy.Net Video Streaming Essential Collection
Psychotherapy.net Video Streaming Essential Collection List List of Videosof Videos as asof 05/18/2015of 1/18/15; Collection will grow as new titles are added monthly* Note: Video series are listed first, followed by single titles. Series Title Featured Therapist(s) Time (hh:mm) 1 Brief Therapy for Cognitive Therapy for Addictions Bruce S. Liese, PhD 1:55 Addictions 2 Brief Therapy for Motivational Interviewing William R. Miller, PhD 1:42 Addictions 3 Brief Therapy for Stages of Change for Addictions John C. Norcross, PhD 1:45 Addictions 4 Child Therapy with the Cognitive-Behavioral Child Bruce Masek, PhD 1:48 Experts Therapy 5 Child Therapy with the Gestalt Therapy with Children Violet Oaklander, PhD 1:47 Experts 6 Child Therapy with the Narrative Therapy with Children Stephen Madigan, PhD 1:43 Experts 7 Couples Therapy with the Internal Family Systems Therapy Richard Schwartz, PhD 2:01 Experts 8 Family Therapy with the Bowenian Family Therapy Philip Guerin, MD 1:57 Experts 9 Family Therapy with the Satir Family Therapy Jean McLendon, 1:44 Experts LCSW, LMFT 10 Family Therapy with the Structural Family Therapy Harry Aponte, LCSW 1:54 Experts 11 Healing Childhood Abuse Healing Childhood Abuse through Tian Dayton, PhD, TEP 0:55 and Trauma through Psychodrama Psychodrama 12 Motivational Interviewing Core Concepts of Motivational Cathy Cole, LCSW 2:15 Step by Step Interviewing 13 Psychotherapy with Gay, Historical Perspectives Ron Scott, PhD 0:41 Lesbian and Bisexual Clients 14 Psychotherapy with Gay, Individual Assessment and Ron Scott, PhD 0:48 Lesbian and Bisexual Psychotherapy Clients 15 Psychotherapy with the Cognitive-Behavioral Therapy with Donald Meichenbaum, 1:49 Experts Donald Meichenbaum PhD 16 Psychotherapy with the Existential-Humanistic James Bugental, PhD 1:54 Experts Psychotherapy 17 Psychotherapy with the Family Systems Therapy Kenneth V. -

Presence, Being, Initiation: Understanding and Teaching Presence, the Lineage and Legacy of James Bugental an Essay Presented Fo
Presence, Being, Initiation: Understanding and Teaching Presence, the Lineage and Legacy of James Bugental An essay presented for the Elizabeth K. and James F. T. Bugental Student Scholarship Award Saybrook University Oakland, California Juanita Ratner [email protected] April 28, 2017 Ratner Bugental’s Legacy and Lineage 2 Abstract Presence is a foundational construct in humanistic, existential, and existential-humanistic psychotherapy. One of the prominent theorists and practitioners of existential-humanistic psychotherapy, James Bugental, articulated the place and meaning of presence and its relation to being or beingness. He trained and truly formed outstanding psychotherapists who continue to teach, practice, and live according to the principles they learned from him. The practice of presence must be learned experientially; those defensive fears, habitual ways of thinking, and self-limiting behaviors that stand in the way of presence must be directly seen and understood. Gradually doing this, clients can enjoy the freedom of living authentically in presence. Bugental’s “Arts” courses were the medium he used to give therapists intensive exposure to conditions that supported developing presence and authenticity. The Existential-Humanistic Institute’s training program, developed and offered in connection with Saybrook University, continues this formative legacy and lineage in Bugental’s format, offering a similar immersive experience and training in the art of presence and connection with being. Ratner Bugental’s Legacy and Lineage 3 Introduction In humanistic, existential, and existential-humanistic (E-H) psychotherapy, there is an underlying assumption that human beings are multi-dimensional, and that there is a reality deeper and more fundamental than the socialized self or even the workings of the brain and nervous system. -
Client-Centered and Existential Approaches: Are They Mostly Similar Or Different?
Kolpachnikov V. V. CLIENT-CENTERED AND EXISTENTIAL APPROACHES: ARE THEY MOSTLY SIMILAR OR DIFFERENT? BASIC RESEARCH PROGRAM WORKING PAPERS SERIES: PSYCHOLOGY WP BRP 14/PSY/2013 This Working Paper is an output of a research project implemented at the National Research University Higher School of Economics (HSE). Any opinions or claims contained in this Working Paper do not necessarily reflect the views of HSE. Kolpachnikov V. V. 1 CLIENT-CENTERED AND EXISTENTIAL APPROACHES: ARE THEY MOSTLY SIMILAR OR DIFFERENT?2 This article analyzes Client-Centered (Person-Centered) and Existential approaches in counseling and psychotherapy. The proximity of these approaches, both in theoretical and practical terms, is demonstrated. Keywords: Client-Centered Psychotherapy(CCT), Person-Centered approach (PCA), Existential approach, quality of contact between client and counselor, centration on experience of client, phenomenology, awareness, comprehension, choice, full-functioning, being in vital world. JEL Classification: Z 1 National Research University Higher School of Economics, Moscow, Russia 2This article presents reflections and comparison of the Client-centered and Existential approaches as a result of decades of the author’s practicing and teaching these approaches. Introduction I will begin this article with an explication of my own theoretical and personal positions relating to the subject of my analysis. I consider it necessary to do this in as much as it will be of help for the reader to better and more deeply understand my observations, reflections, and conclusions about the relationship between the Person-Centered and Existential approaches in psychological counseling and psychotherapy. Such a course corresponds to tendencies in the modern humanities (and in science as a whole) as knowledge is becoming viewed as inseparable from those who hold knowledge, is personal (Polanyi, 1958), is included in existing scientific discourses, contexts, and dialogues, and is a social construct (Gadamer, 1975; Kvale, 1996; Habermas, 1971 ;Giorgi, 1975, etc.). -

Sándor Ferénczi and the Origins of Humanistic Psychology
ARTÍCULOS SOBRE FERENCZI. CONTEXTUALES E HISTÓRICOS SÁNDOR FERENCZI AND THE ORIGINS OF HUMANISTIC PSYCHOLOGY Dassie Hoffman ABSTRACT This article discusses Sándor Ferenczi’s contributions to the evolution of psychoanalytic theories, and how these ideas were passed through the generations. Ferenczi introduced such concepts as greater activity by the psychotherapist, the need for emotional connection between the therapist and client, the significance of the interpersonal aspects of the therapeutic experience, and the place of empathy within the therapeutic milieu. The second generation reviewed here is the Neo-Freudian, including Andras Angyal, Izette deForest, Erich Fromm, Frieda Fromm-Reichmann, Karen Horney, Harry Stack Sullivan, and Clara Thompson. The next generation reviewed is that of the foremost humanistic psychologists, Abraham Maslow, Rollo May, Carl Rogers, and James Bugental. INTRODUCTION This paper focuses on Sándor Ferenczi’s impact upon the ideas of four co-founders of humanistic psychology. The essay is divided into three sections; the first reviews the origins of psychoanalysis, and the importance of Sándor Ferenczi’s ideas to this process; the second section examines how Ferenczi’s ideas influenced the neo-Freudians, and how this next generation employed his theories; the final section of this essay explores the ways in which the co-founders of humanistic psychology, Abraham Maslow, Rollo May, Carl Rogers, and James Bugental were influenced directly and indirectly byFerenczi. THE IMPORTANCE OF SANDOR FERENCZI TO PSYCHOANALYSIS Humanistic psychology evolved partly as a response to the teachings of psychoanalysis and behaviorism: “Some psychologists... drew upon a long tradition linking psychology with the humanities and in a rebellious manner, institutionally founded humanistic psychology. -

Journal of Humanistic Psychology
SAGE PUBLICATIONS PRESENTS JOURNAL OF HUMANISTIC PSYCHOLOGY Published in cooperation with the Association for Humanistic Psychology Editor: Thomas Greening, Saybrook Graduate School and Research Center, San Francisco, California Explore the many facets of humanistic psychology (the third force) in the most influential and respected international publication in the field the Journal of Humanistic Psychology' Founded by Abraham Maslow and Anthony Sutich in 1961, the Journal of Humanistic Psychology provides a readable and comprehensive overview of humanistic psychology, broadly and critically considered, with articles on a variety of topics such as: Authenticity Humanistic politics Personal growth Community-building Human science research Person-centered counselling Confluent education Identity Self-actualization and self-transcendence Consciousness I-Thou encounters Spiritual development Creativity Love Synergy Existential-humanistic psychotherapy Patients rights and empowerment Values Holistic healing and learning Peace and mediation In addition to bringing you a variety of experiential reports, theoretical papers, personal essays, poems, and research studies emphasizing human science methods and analyses of contemporary culture, Journal of Humanistic Psychology also supplements its coverage with in-depth studies of topics of particular interest, including special issues on: Existential-Humanistic Psychotherapy Ecopsychology James Bugental Positive Psychology Peace and Citizen Diplomacy Rollo May International -

Counseling & Therapy Bro V2 R2.Indd
Prepare your students for their counseling careers learn more at alexanderstreet.com/counseling ALEXANDER STREET’S COUNSELING & THERAPY COLLECTIONS Foundational videos from 1985-2010 cover recent history of practices Provide your students with the essential skills and knowledge CLASSIC Counseling & Therapy in Video: Classic provides 500+ hours of to work effectively with clients video o ering a rsthand look at the realities of working with clients and the challenges associated with putting theoretical concepts into practice. World renowned therapists such as Albert Ellis, Violet Oaklander, Derald Wing Sue, and John Norcross learn more at Diverse Content Exclusive Access to demonstrate their methods and techniques. Students and alexanderstreet.com/counseling to Engage Students Content Partners the Experts faculty will also nd documentaries on the human condition, which help with re ection and empathy skills. ACTUAL THERAPY • Microtraining, Alexander Street’s Highlighted experts include: Highlights include: The Mirror Cracked: Attachment and the Therapeutic Relationship; Women and Depression; Web of Addiction. SESSIONS & REENACTMENTS Counseling Imprint, o ers a strong • Derald Wing Sue – emphasis on culturally sensitive Hundreds of counseling sessions Multicultural Expert Films about the founders of theory counselor training videos. cover a wide range of theories and • Allen Ivey – and the progression of practices to today skills, and include diverse clients • Symptom Media is the leading Microskills Model of Counseling VOL. III and presenting issues. Counseling & Therapy in Video: Volume III presents a rm grounding in the theoretical modalities of provider of DSM-5® / ICD-10 • Jay Haley – counseling and psychotherapy while expanding into new and emerging areas such as social media, video content. -

'Encountering Resistance' in Psychotherapy
Resistance is futile? An existential-phenomenological exploration of psychotherapists' experiences of 'encountering resistance' in psychotherapy Volume I Michael Worrell August 2002 This thesis is submitted in fulfilment ofthe requirements for the degree ofPhD at the School ofPsychotherapy and Counselling at Regent's College London (Validated by City University London) © 'Iichael "'orrell Table of contents Heading Page Volume I Table ofcontents 2 Acknowledgements 5 Abstract 6 Part I: Theories ofResistance 7 Chapter 1: Introduction- 'resistance is futile'? 8 Chapter 2: 'Whatever interrupts progress': psychoanalytic approaches 30 Chapter 3: 'Irrational non-compliance'?: behavioural and 87 cognitive approaches Chapter 4: 'Resistance is and isn't': humanistic approaches 110 Chapter 5: The 'persistence' ofresistance or the death ofresistance: 120 systemic approaches Chapter 6: Resistance as trans-theoretical: integrative approaches. 129 Chapter 7: 'Where there is power there is resistance': 138 postmodem, narrative and constructivist approaches. Chapter 8: The possibilities ofresistance: existential perspectives. 144 Summary: Part I- Theories ofresistance 171 2 Volume II Table ofContents 173 List ofTables 175 List ofGraphs 176 Part II: Researching Resistance 177 Chapter 9: Researching resistance: 178 quantitative and qualitative approaches Chapter 10: An existential-phenomenological investigation of 199 therapists' experiences ofencountering resistance in psychotherapy Chapter 11: A survey oftherapists' experiences, attitudes 244 and concerns -

Expert Psychotherapists' Use of Four Common Factors In
EXPERT PSYCHOTHERAPISTS’ USE OF FOUR COMMON FACTORS IN PSYCHOTHERAPY A DISSERTATION SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY IN THE GRADUATE SCHOOL OF THE TEXAS WOMAN’S UNIVERSITY DEPARTMENT OF PSYCHOLOGY AND PHILOSOPHY COLLEGE OF ARTS AND SCIENCES BY KYLE M. ERWIN, B.A., M.A. DENTON, TEXAS DECEMBER 2015 Copyright © Kyle M. Erwin, 2015 all rights reserved. iii DEDICATION For Mom, Dad, Trisha, Stephen, Will, Rhyder, and Joe iv ACKNOWLEDGMENTS I gratefully acknowledge the exceptional individuals and works that contributed to this dissertation. I want to acknowledge and express my gratitude for the influence of Duncan’s (2010) On Becoming a Better Therapist. I heavily drew from this work to develop and define the four common factors underlying the majority of therapy outcomes. Moreover, I used Ducan’s work as a beacon of light to focus my research efforts on the most eminent and important works related to common factors. In doing so, I developed an excellent foundation for the common factors portion of the literature review and methods section. To lay the foundation of and write the methods section of the proposed research, I unashamedly drew from Hill’s (2012) Consensual Qualitative Research: A Practical Resource for Investigating Social Science Phenomena. Like Duncan’s work, Hill’s book provided useful references for primary sources that undoubtedly added to the depth of the methods section and my understanding of consensual qualitative research. Ericsson, Charness, Hoffman, and Feltovich’s (2006) The Cambridge Handbook of Expertise and Expert Performance provided a wealth of information on the history, development, and research base related to expertise and expert performance.