So Far, Our Indianapolis-Ibadan Study Has Demonstrated That
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Channel Affiliate Market Timeframe of Move Call
TV Broadcasters’ Impact on Indiana Impact on IN 06 Broadcasters have an impact of $21.99 billion annually on Indiana’s economy. 46,420 Jobs 31 Commercial TV Stations Call Channel Affiliate Market Timeframe of Move WALV-CD 0 Cozi TV Affiliation Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WBXI-CA 47 Wx Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WDNI-CD 19 Telemundo Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WDTI 69 Daystar TV Network Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WHMB-TV 40 Independent Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WIPB 49 Public Television Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WIPX-TV 63 ION Media Networks Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WIWU-CD 51 Independent Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WTIU 30 Public Television Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WTTK 29 CBS Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WTTV 4 CBS Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WXIN 59 FOX Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WCET 48 Public Television Cincinnati, OH (36) Phase 6: Sept 7, 2019 - Oct 18, 2019 WCPO-TV 9 ABC Cincinnati, OH (36) Phase 6: Sept 7, 2019 - Oct 18, 2019 WCVN-TV 54 Public Television Cincinnati, OH (36) Phase 6: Sept 7, 2019 - Oct 18, 2019 WKON 52 Public Television Cincinnati, OH (36) Phase 6: Sept 7, 2019 - Oct 18, 2019 WLWT 5 NBC Cincinnati, OH (36) Phase 6: Sept 7, 2019 - Oct 18, -

Nexstar Media Group Stations(1)
Nexstar Media Group Stations(1) Full Full Full Market Power Primary Market Power Primary Market Power Primary Rank Market Stations Affiliation Rank Market Stations Affiliation Rank Market Stations Affiliation 2 Los Angeles, CA KTLA The CW 57 Mobile, AL WKRG CBS 111 Springfield, MA WWLP NBC 3 Chicago, IL WGN Independent WFNA The CW 112 Lansing, MI WLAJ ABC 4 Philadelphia, PA WPHL MNTV 59 Albany, NY WTEN ABC WLNS CBS 5 Dallas, TX KDAF The CW WXXA FOX 113 Sioux Falls, SD KELO CBS 6 San Francisco, CA KRON MNTV 60 Wilkes Barre, PA WBRE NBC KDLO CBS 7 DC/Hagerstown, WDVM(2) Independent WYOU CBS KPLO CBS MD WDCW The CW 61 Knoxville, TN WATE ABC 114 Tyler-Longview, TX KETK NBC 8 Houston, TX KIAH The CW 62 Little Rock, AR KARK NBC KFXK FOX 12 Tampa, FL WFLA NBC KARZ MNTV 115 Youngstown, OH WYTV ABC WTTA MNTV KLRT FOX WKBN CBS 13 Seattle, WA KCPQ(3) FOX KASN The CW 120 Peoria, IL WMBD CBS KZJO MNTV 63 Dayton, OH WDTN NBC WYZZ FOX 17 Denver, CO KDVR FOX WBDT The CW 123 Lafayette, LA KLFY CBS KWGN The CW 66 Honolulu, HI KHON FOX 125 Bakersfield, CA KGET NBC KFCT FOX KHAW FOX 129 La Crosse, WI WLAX FOX 19 Cleveland, OH WJW FOX KAII FOX WEUX FOX 20 Sacramento, CA KTXL FOX KGMD MNTV 130 Columbus, GA WRBL CBS 22 Portland, OR KOIN CBS KGMV MNTV 132 Amarillo, TX KAMR NBC KRCW The CW KHII MNTV KCIT FOX 23 St. Louis, MO KPLR The CW 67 Green Bay, WI WFRV CBS 138 Rockford, IL WQRF FOX KTVI FOX 68 Des Moines, IA WHO NBC WTVO ABC 25 Indianapolis, IN WTTV CBS 69 Roanoke, VA WFXR FOX 140 Monroe, AR KARD FOX WTTK CBS WWCW The CW WXIN FOX KTVE NBC 72 Wichita, KS -
NSAC Book Pages
AAF District 7’s role in the NATIONAL STUDENT ADVERTISING COMPETITION A HISTORY 1967–2012 AAF DISTRICT 7’S ROLE IN THE NATIONAL STUDENT ADVERTISING COMPETITION ––– A HISTORY I first became knowledgeable of the activities of the Seventh District in 1982 when for the first time, I attended their Convention. Prior to this Convention a member of our Nashville Advertising Federation, Bill Satterwhite, asked me to handle some minor duties for the District Student Advertising Competition, which was to be held in Nashville in 1983. He Dear Charlie, described these duties as “being in Thank You for sending charge of getting some equipment to be me a copy of your book used for this competition, such as projection screens, sound on the NSAC and the equipment, etc.” I agreed to take care of this assignment, but Seventh District. was much surprised when at the National Convention in June, Former Governor Mike Gallagher, congratulated me for being IN I enjoyed it, and deeply CHARGE of the District Student Competition for ‘83. I told him appreciate your taking that there must be a mistake because I had only been informed the time to highlight of duties related to arranging for some equipment. The aftermath this important AAF of all of this was that I was the Competition Coordinator in 1983. National program and This was a significant assignment for me in that while the Seventh District’s carrying it out, I became aware of the uniqueness of this student central role in starting, competition, and became completely enthusiastic about the developing, and purposes served and value received by advertising students from growing it. -

I. Tv Stations
Before the FEDERAL COMMUNICATIONS COMMISSION Washington, DC 20554 In the Matter of ) ) MB Docket No. 17- WSBS Licensing, Inc. ) ) ) CSR No. For Modification of the Television Market ) For WSBS-TV, Key West, Florida ) Facility ID No. 72053 To: Office of the Secretary Attn.: Chief, Policy Division, Media Bureau PETITION FOR SPECIAL RELIEF WSBS LICENSING, INC. SPANISH BROADCASTING SYSTEM, INC. Nancy A. Ory Paul A. Cicelski Laura M. Berman Lerman Senter PLLC 2001 L Street NW, Suite 400 Washington, DC 20036 Tel. (202) 429-8970 April 19, 2017 Their Attorneys -ii- SUMMARY In this Petition, WSBS Licensing, Inc. and its parent company Spanish Broadcasting System, Inc. (“SBS”) seek modification of the television market of WSBS-TV, Key West, Florida (the “Station”), to reinstate 41 communities (the “Communities”) located in the Miami- Ft. Lauderdale Designated Market Area (the “Miami-Ft. Lauderdale DMA” or the “DMA”) that were previously deleted from the Station’s television market by virtue of a series of market modification decisions released in 1996 and 1997. SBS seeks recognition that the Communities located in Miami-Dade and Broward Counties form an integral part of WSBS-TV’s natural market. The elimination of the Communities prior to SBS’s ownership of the Station cannot diminish WSBS-TV’s longstanding service to the Communities, to which WSBS-TV provides significant locally-produced news and public affairs programming targeted to residents of the Communities, and where the Station has developed many substantial advertising relationships with local businesses throughout the Communities within the Miami-Ft. Lauderdale DMA. Cable operators have obviously long recognized that a clear nexus exists between the Communities and WSBS-TV’s programming because they have been voluntarily carrying WSBS-TV continuously for at least a decade and continue to carry the Station today. -

The American Legion Annual Report 2014 PREAMBLE to the AMERICAN LEGION CONSTITUTION
THE AMERICAN LEGION ANNUAL REPORT: 2014 AMERICANTHE REPORT: LEGION ANNUAL The American Legion Annual Report 2014 PREAMBLE TO THE AMERICAN LEGION CONSTITUTION FOR GOD AND COUNTRY WE ASSOCIATE OURSELVES TOGETHER FOR THE FOLLOWING PURPOSES: To uphold and defend the Constitution of the United States of America; To maintain law and order; To foster and perpetuate a one hundred percent Americanism; To preserve the memories and incidents of our associations in the Great Wars; To inculcate a sense of individual obligation to the community, state and nation; To combat the autocracy of both the classes and the masses; To make right the master of might; To promote peace and goodwill on earth; To safeguard and transmit to posterity the principles of justice, freedom and democracy; To consecrate and sanctify our comradeship by our devotion to mutual helpfulness. The American Legion The American Legion John H. Geiger National Headquarters Washington Offi ce Operations Center 700 N. Pennsylvania St. 1608 K St. NW 5745 Lee Road Indianapolis, IN 46204 Washington, D.C. 20006 Indianapolis, IN 46216 (317) 630-1200 (202) 861-2700 (317) 860-3100 P.O. Box 1055 Indianapolis, IN 46206 THE AMERICAN LEGION ANNUAL REPORT Who We Are . 2-3 System Worth Saving . 4-5 Legislative . 6-7 National Emergency Fund . 8-9 Troop Support . .10-11 Veterans Education . .12-13 Veterans Employment . .14-15 Membership . .16-17 American Legion Baseball . .18-19 Operation Comfort Warriors . .20-21 Youth Cadet Law Enforcement. .22-23 Fundraising . .24-25 Youth Programs . .26-27 Emblem Sales . .28-29 American Legion Riders . .30-31 Scholarships . -

Gaming-Sports Partnerships*
Gaming-Sports Partnerships* Updated 7/6/2021 USA / # Gaming Company League Team Announced International Provisions Synopsis 169 Golden Nugget Rocket 6/30/21 USA Marketing Golden Nugget will have on- Online Gaming Mortgage site branding at the event. The Classic casino will be giving away prizes and offering exclusive (PGA) promotional casino and sportsbook bonuses for tournament attendees. 168 Bally's Phoenix 6/30/21 USA Market Bally's is the exclusive sports Mercury access, betting partner of the Phoenix (WNBA) marketing Mercury over 15 years beginning July 1, 2021. Upon the Phoenix Mercury's receipt of a mobile sports betting license from the Arizona Dept. of Gaming, Bally's will, among other things, host and manage an online and mobile sports betting service in Arizona, operate a retail sportsbook in the vicinity of the Phoenix Suns Arena, and promote its business in connection with Phoenix Mercury games. 167 Sportradar NHL 6/29/21 USA Data, Having served as the NHL’s Streaming official global data distributor since 2015, Sportradar will now distribute the NHL’s official data and statistics to media, technology and sports betting companies worldwide, including real-time data from the NHL’s new Puck and Player Tracking technology. The deal also awards Sportradar rights to provide sports betting operators with live streams of NHL games via operators’ digital betting platforms in legalized markets. 166 Kindred/Unibet Stewart-Haas 6/23/21 USA Marketing Through the Unibet brand, Racing Kindred Group will serve as a (Nascar) primary sponsor for two NASCAR Cup Series at Indianapolis Motor Speedway and Martinsville Speedway (VA). -

National Executive Committee the AMERICAN LEGION
PROCEEDINGS of the National Executive Committee THE AMERICAN LEGION NATIONAL HEADQUARTERS INDIANAPOLIS, INDIANA May 6-7, 1970 43 PRINTED IN U.S.A. PROCEEDINGS of the National Executive Committee THE AMERICAN LEGION NATIONAL HEADQUARTERS INDIANAPOLIS, INDIANA May 6-7, 1970 143 PRINTED IN U.8.A. INDEX Page Page COMMISSION, COMMITTEE AND PUBLIC RELATIONS 27 SUB-COMMITTEE REPORTS PUBLICATIONS 61 AMERICANISM 47 Resolutions following: REHABILITATION 35 No. Resolutions following: 14— PrayersNo. in Public Buildings 53 15— Annual Observances of Moon Shot. 53 19— Rescinding National Rehabilitation CHILD WELFARE 115 Non-Legislative Policy resolutions... 40 Resolutions following: 20— Funds for Operating VA Medical No. and Hospital Program 41 38— Supplementary21— Income of the Disability Pension 42 Under Employed 121 22— Amend 38 USC, Chapter 35 42 39— Including23— Servicemen’s Families Amend 38 USC, Chapter 3104 43 in Welfare and Social Service 24— Treatment and Rehabilitation of Programs 121 Veterans with Chronic Alcoholism. .. 43 40— Interstate Compact on the Placement of Children 122 25— Participation in Conference on Aging 44 41— Rescinding33—Transfer of Non-Legislative of National Life Policy Resolutions 123 Insurance Funds 45 CONVENTION 90 REORGANIZATION SUB-COMMITTEE... 69 Resolutions following: Resolutions following: No. No. 9—National Convention Badges 91 4— Redesignation of Child Welfare 10—National Convention Registration Fee 92 Commission 71 CONVENTION, REPORT on 1969 62 5— Redesignation of Publications Commission 72 ECONOMIC 85 6— Redesignation of Rehabilitation Resolutions following: Commission 73 No. 34— RemoveSECURITY Limitations on Loans 87 13 35— AmendResolutions Dual Compensation following: Act 88 36— Postal No.Reform Legislation 88 37— Career Civil Service Employees 89 26—Vietnam 16 50TH ANNIVERSARY COMMITTEE 98 32—The Reid Amendment 17 FINANCE 99 1— Draft Evaders and/or Deserters... -

Channel Affiliate Market Timeframe of Move Call
TV Broadcasters’ Impact on Indiana Impact on IN 08 Broadcasters have an impact of $21.99 billion annually on Indiana’s economy. 46,420 Jobs 31 Commercial TV Stations Call Channel Affiliate Market Timeframe of Move WALV-CD 0 Cozi TV Affiliation Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WBXI-CA 47 Wx Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WDNI-CD 19 Telemundo Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WDTI 69 Daystar TV Network Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WHMB-TV 40 Independent Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WIPB 49 Public Television Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WIPX-TV 63 ION Media Networks Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WIWU-CD 51 Independent Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WTIU 30 Public Television Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WTTK 29 CBS Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WTTV 4 CBS Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WXIN 59 FOX Indianapolis, IN (27) Phase 6: Sept 7, 2019 - Oct 18, 2019 WAVE 3 NBC Louisville, KY (49) Phase 6: Sept 7, 2019 - Oct 18, 2019 WDRB 41 FOX Louisville, KY (49) Phase 6: Sept 7, 2019 - Oct 18, 2019 WJYL-CD 9 Trinity Broadcasting Network Louisville, KY (49) Phase 6: Sept 7, 2019 - Oct 18, 2019 WKMJ-TV 68 Public Television Louisville, KY (49) Phase 6: Sept 7, 2019 - Oct 18, 2019 WKPC-TV 15 Public Television Louisville, KY (49) Phase 6: Sept 7, -
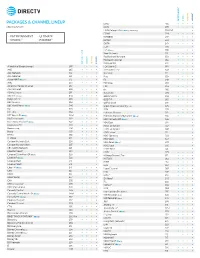
Packages & Channel Lineup
™ ™ ENTERTAINMENT CHOICE ULTIMATE PREMIER PACKAGES & CHANNEL LINEUP ESNE3 456 • • • • Effective 6/17/21 ESPN 206 • • • • ESPN College Extra2 (c only) (Games only) 788-798 • ESPN2 209 • • • • • ENTERTAINMENT • ULTIMATE ESPNEWS 207 • • • • CHOICE™ • PREMIER™ ESPNU 208 • • • EWTN 370 • • • • FLIX® 556 • FM2 (c only) 386 • • Food Network 231 • • • • ™ ™ Fox Business Network 359 • • • • Fox News Channel 360 • • • • ENTERTAINMENT CHOICE ULTIMATE PREMIER FOX Sports 1 219 • • • • A Wealth of Entertainment 387 • • • FOX Sports 2 618 • • A&E 265 • • • • Free Speech TV3 348 • • • • ACC Network 612 • • • Freeform 311 • • • • AccuWeather 361 • • • • Fuse 339 • • • ActionMAX2 (c only) 519 • FX 248 • • • • AMC 254 • • • • FX Movie 258 • • American Heroes Channel 287 • • FXX 259 • • • • Animal Planet 282 • • • • fyi, 266 • • ASPiRE2 (HD only) 381 • • Galavisión 404 • • • • AXS TV2 (HD only) 340 • • • • GEB America3 363 • • • • BabyFirst TV3 293 • • • • GOD TV3 365 • • • • BBC America 264 • • • • Golf Channel 218 • • 2 c BBC World News ( only) 346 • • Great American Country (GAC) 326 • • BET 329 • • • • GSN 233 • • • BET HER 330 • • Hallmark Channel 312 • • • • BET West HD2 (c only) 329-1 2 • • • • Hallmark Movies & Mysteries (c only) 565 • • Big Ten Network 610 2 • • • HBO Comedy HD (c only) 506 • 2 Black News Channel (c only) 342 • • • • HBO East 501 • Bloomberg TV 353 • • • • HBO Family East 507 • Boomerang 298 • • • • HBO Family West 508 • Bravo 237 • • • • HBO Latino3 511 • BYUtv 374 • • • • HBO Signature 503 • C-SPAN2 351 • • • • HBO West 504 • -

Konstantin Pavolotsky Interviewer: Whitney Stalnaker Date of Interview: July 2, 2015 Location of Interview: 6028 Mayfield Rd #8, Mayfield Heights, OH
Soviet Jewish Oral History Project Western Reserve Historical Society Interviewee: Konstantin Pavolotsky Interviewer: Whitney Stalnaker Date of interview: July 2, 2015 Location of interview: 6028 Mayfield Rd #8, Mayfield Heights, OH Whitney Stalnaker: Today is July 2, 2015. My name is Whitney Stalnaker. I’m here with Konstantin Pavolotsky. We are here in his office at Mayfield Heights. First of all I do want to thank you again for agreeing to meet with me. First we’re going to start with a pretty easy question, could you just introduce yourself? Konstantin Pavolotsky: Konstantin Pavolotsky. General things I work in Mayfield Heights, I reside in Cleveland since 1996 and in the United States since 1990. WS: Okay great. Can you tell me a little bit about your family here? KP: I have a wife, Larisa, and my son Felix. He is 28 years old. He is a Kent State University student. WS: Wonderful. Does your wife work here or…? KP: Yeah she works with me. She is the manager for the office. She is an accountant by education. She works with me since I was opening my practice. WS: Where did you go to school? KP: I graduated from dental school. It was a dental school in Moscow, which was then the capital of the Soviet Union. I graduated in 1986. In the United States I graduated dental school from Indiana University School of dentistry class of 1995. WS: I would like to talk a little bit about your life pre-immigration. Could you describe what your life was like before you decided to immigrate? KP: After I graduated dental school in 86’ I had a residency in Rostov which is a city on the river Don in the South of Russia for one year. -

Wttv-Tv, Wxin-Tv Eeo Public File Report I. Vacancy List
Page: 1/11 WTTV-TV, WXIN-TV EEO PUBLIC FILE REPORT April 1, 2019 - March 31, 2020 I. VACANCY LIST See Section II, the "Master Recruitment Source List" ("MRSL") for recruitment source data Recruitment Sources ("RS") RS Referring Job Title Used to Fill Vacancy Hiree 2-20, 25, 27-28, 30-31, 34-37, 39, 41, Producer, Digital Content 13 43-52, 55-58 2-12, 14-20, 25-28, 30-31, 34-37, 39, Reporter/MMJ 26 41, 43-52, 55-58 2-10, 12, 14-20, 25-28, 30-31, 34-37, Executive Producer 26 39, 41, 43-52, 55-58 2-10, 12-20, 25, 27-28, 30-31, 34-37, Associate Producer 13 39, 41, 43-52, 55-58 2-10, 12, 14-20, 25-28, 30-31, 34-37, Production Technician 26 39, 41, 43-52, 55-58 1, 3-20, 25, 27-28, 30-31, 34-39, 41, 43 Reporter 13 -50, 52, 55-58 2-12, 14-20, 25, 27-28, 30-31, 34-37, Editor, Non- Linear 18 39, 41, 43-50, 52, 55-58 2-12, 14-20, 25, 27-28, 30-31, 33-37, Reporter/MMJ 18 39, 43-50, 52, 55-58 2-20, 25, 27-28, 30-31, 34-37, 39, 43- Producer, News 13 50, 52, 55-58 2-20, 25, 27-31, 34-37, 39, 43-50, 52, Sales Assistant 18 55-58 2-20, 25, 27-28, 30-31, 34-37, 43-50, Anchor, Sports 13 52, 55-58 2-12, 14-25, 27-28, 30-31, 34-37, 39- Associate Producer 44 40, 42-44, 46-50, 52-56, 58 2-20, 25, 27-28, 30-31, 34-37, 39, 43- Account Executive 13 50, 52-53, 55-56, 58 2-12, 14-20, 25, 27-31, 34-37, 39, 43- Digital Content Producer 29 50, 52-53, 55-56, 58 2-11, 14-20, 25, 27-28, 30-31, 34-37, Graphic Artist 44 39, 43-50, 52-53, 55-56, 58 2-11, 14-20, 25, 27-28, 30-32, 34-37, Vice President/General Manager, WXIN/WTTV 32 39, 43-53, 55-56, 58 2-3, 5-10, 12, 14-20, 25-28, 30-32, 35- Director, Sales 26 37, 39, 43-53, 55-56, 58 2-3, 5-11, 14-20, 25, 27-28, 30-32, 35- Director, News 32 37, 39, 43-53, 55-56, 58 Page: 2/11 WTTV-TV, WXIN-TV EEO PUBLIC FILE REPORT April 1, 2019 - March 31, 2020 II. -
![Indianapolis, in WHHH-FM, WTLC-AM, WTLC-FM, WDNI-CD and WNOW-FM EEO PUBLIC FILE REPORT April 1, 2020 – March 31, 2021 [1]](https://docslib.b-cdn.net/cover/0532/indianapolis-in-whhh-fm-wtlc-am-wtlc-fm-wdni-cd-and-wnow-fm-eeo-public-file-report-april-1-2020-march-31-2021-1-2940532.webp)
Indianapolis, in WHHH-FM, WTLC-AM, WTLC-FM, WDNI-CD and WNOW-FM EEO PUBLIC FILE REPORT April 1, 2020 – March 31, 2021 [1]
Radio One of Indiana, L.P. Radio One – Indianapolis, IN WHHH-FM, WTLC-AM, WTLC-FM, WDNI-CD and WNOW-FM EEO PUBLIC FILE REPORT April 1, 2020 – March 31, 2021 [1] I. VACANCY LIST See Section II, the “Master Recruitment Source List” (“MRSL”) for recruitment source data Recruitment Sources (RS) Used Number of Candidates RS Referring Job Title to Fill Vacancy Interviewed (RS) Hiree Sales Team Coordinator (10/23/20) 1-35, 38, 43 3[2 RS #(38), 1 RS #(43)] 38 Morning Show Producer (10/16/20) 1-35, 38, 43 3[1 RS #(38), 2 RS #(43)] 38 Producer (10/15/20) 1-35, 43 3[2 RS #(35), 1 RS #(43)] 35 Account Executive (12/28/20) 1-35, 38, 43 5[1 RS #(38), 4 RS # 43] 38 Online Editor (1/26/20) 1-35, 43 5[3 RS #43, 2 RS # 35] 43 Integrated Marketing Specialist (2/1/21) 1-35, 38, 43 5[1 RS #35, 1 RS #38,3 RS #43] 38 Total Candidates Interviewed - 24 [1] This report provides recruitment data collected from March 21, 2020 through March 19, 2021. Radio One of Indiana, L.P. Radio One – Indianapolis, IN WHHH-FM, WTLC-AM, WTLC-FM, WDNI-CD and WNOW-FM EEO PUBLIC FILE REPORT April 1, 2020 – March 31, 2021 [1] II. MASTER RECRUITMENT SOURCE LIST (MRSL) Source Entitled No. of Interviewees RS Referred by RS RS Information to Vacancy Number Notification? over (Yes/No) 12-month period 1 American Women in Radio and Television Y 0 8405 Greensboro Drive, Ste.