Hairy Tongue - a Series of 4 Cases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Oral Diagnosis: the Clinician's Guide
Wright An imprint of Elsevier Science Limited Robert Stevenson House, 1-3 Baxter's Place, Leith Walk, Edinburgh EH I 3AF First published :WOO Reprinted 2002. 238 7X69. fax: (+ 1) 215 238 2239, e-mail: [email protected]. You may also complete your request on-line via the Elsevier Science homepage (http://www.elsevier.com). by selecting'Customer Support' and then 'Obtaining Permissions·. British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Library of Congress Cataloging in Publication Data A catalog record for this book is available from the Library of Congress ISBN 0 7236 1040 I _ your source for books. journals and multimedia in the health sciences www.elsevierhealth.com Composition by Scribe Design, Gillingham, Kent Printed and bound in China Contents Preface vii Acknowledgements ix 1 The challenge of diagnosis 1 2 The history 4 3 Examination 11 4 Diagnostic tests 33 5 Pain of dental origin 71 6 Pain of non-dental origin 99 7 Trauma 124 8 Infection 140 9 Cysts 160 10 Ulcers 185 11 White patches 210 12 Bumps, lumps and swellings 226 13 Oral changes in systemic disease 263 14 Oral consequences of medication 290 Index 299 Preface The foundation of any form of successful treatment is accurate diagnosis. Though scientifically based, dentistry is also an art. This is evident in the provision of operative dental care and also in the diagnosis of oral and dental diseases. While diagnostic skills will be developed and enhanced by experience, it is essential that every prospective dentist is taught how to develop a structured and comprehensive approach to oral diagnosis. -

Guideline # 18 ORAL HEALTH
Guideline # 18 ORAL HEALTH RATIONALE Dental caries, commonly referred to as “tooth decay” or “cavities,” is the most prevalent chronic health problem of children in California, and the largest single unmet health need afflicting children in the United States. A 2006 statewide oral health needs assessment of California kindergarten and third grade children conducted by the Dental Health Foundation (now called the Center for Oral Health) found that 54 percent of kindergartners and 71 percent of third graders had experienced dental caries, and that 28 percent and 29 percent, respectively, had untreated caries. Dental caries can affect children’s growth, lead to malocclusion, exacerbate certain systemic diseases, and result in significant pain and potentially life-threatening infections. Caries can impact a child’s speech development, learning ability (attention deficit due to pain), school attendance, social development, and self-esteem as well.1 Multiple studies have consistently shown that children with low socioeconomic status (SES) are at increased risk for dental caries.2,3,4 Child Health Disability and Prevention (CHDP) Program children are classified as low socioeconomic status and are likely at high risk for caries. With regular professional dental care and daily homecare, most oral disease is preventable. Almost one-half of the low-income population does not obtain regular dental care at least annually.5 California children covered by Medicaid (Medi-Cal), ages 1-20, rank 41 out of all 50 states and the District of Columbia in receiving any preventive dental service in FY2011.6 Dental examinations, oral prophylaxis, professional topical fluoride applications, and restorative treatment can help maintain oral health. -

Oral Lesions in Sjögren's Syndrome
Med Oral Patol Oral Cir Bucal. 2018 Jul 1;23 (4):e391-400. Oral lesions in Sjögren’s syndrome patients Journal section: Oral Medicine and Pathology doi:10.4317/medoral.22286 Publication Types: Review http://dx.doi.org/doi:10.4317/medoral.22286 Oral lesions in Sjögren’s syndrome: A systematic review Julia Serrano 1, Rosa-María López-Pintor 1, José González-Serrano 1, Mónica Fernández-Castro 2, Elisabeth Casañas 1, Gonzalo Hernández 1 1 Department of Oral Medicine and Surgery, School of Dentistry, Complutense University, Madrid, Spain 2 Rheumatology Service, Hospital Infanta Sofía, Madrid, Spain Correspondence: Departamento de Especialidades Clínicas Odontológicas Facultad de Odontología Universidad Complutense de Madrid Plaza Ramón y Cajal s/n, 28040 Madrid. Spain [email protected] Serrano J, López-Pintor RM, González-Serrano J, Fernández-Castro M, Casañas E, Hernández G. Oral lesions in Sjögren’s syndrome: A system- atic review. Med Oral Patol Oral Cir Bucal. 2018 Jul 1;23 (4):e391-400. Received: 18/11/2017 http://www.medicinaoral.com/medoralfree01/v23i4/medoralv23i4p391.pdf Accepted: 09/05/2018 Article Number: 22291 http://www.medicinaoral.com/ © Medicina Oral S. L. C.I.F. B 96689336 - pISSN 1698-4447 - eISSN: 1698-6946 eMail: [email protected] Indexed in: Science Citation Index Expanded Journal Citation Reports Index Medicus, MEDLINE, PubMed Scopus, Embase and Emcare Indice Médico Español Abstract Background: Sjögren’s syndrome (SS) is an autoimmune disease related to two common symptoms: dry mouth and eyes. Although, xerostomia and hyposialia have been frequently reported in these patients, not many studies have evaluated other oral manifestations. -

Oral Manifestations of Systemic Disease Their Clinical Practice
ARTICLE Oral manifestations of systemic disease ©corbac40/iStock/Getty Plus Images S. R. Porter,1 V. Mercadente2 and S. Fedele3 provide a succinct review of oral mucosal and salivary gland disorders that may arise as a consequence of systemic disease. While the majority of disorders of the mouth are centred upon the focus of therapy; and/or 3) the dominant cause of a lessening of the direct action of plaque, the oral tissues can be subject to change affected person’s quality of life. The oral features that an oral healthcare or damage as a consequence of disease that predominantly affects provider may witness will often be dependent upon the nature of other body systems. Such oral manifestations of systemic disease their clinical practice. For example, specialists of paediatric dentistry can be highly variable in both frequency and presentation. As and orthodontics are likely to encounter the oral features of patients lifespan increases and medical care becomes ever more complex with congenital disease while those specialties allied to disease of and effective it is likely that the numbers of individuals with adulthood may see manifestations of infectious, immunologically- oral manifestations of systemic disease will continue to rise. mediated or malignant disease. The present article aims to provide This article provides a succinct review of oral manifestations a succinct review of the oral manifestations of systemic disease of of systemic disease. It focuses upon oral mucosal and salivary patients likely to attend oral medicine services. The review will focus gland disorders that may arise as a consequence of systemic upon disorders affecting the oral mucosa and salivary glands – as disease. -
Addisonian Pigmentation of the Oral Mucosa
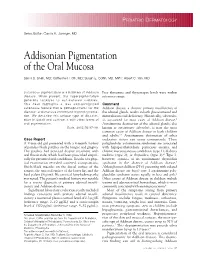
PEDIATRIC DERMATOLOGY Series Editor: Camila K. Janniger, MD Addisonian Pigmentation of the Oral Mucosa Samir S. Shah, MD; Catherine H. Oh, MD; Susan E. Coffin, MD, MPH; Albert C. Yan, MD Cutaneous pigmentation is a hallmark of Addison Free thyroxine and thyrotropin levels were within disease. When present, the hyperpigmentation reference range. generally localizes to sun-exposed surfaces. This case highlights a less well-recognized Comment cutaneous feature that is pathognomonic for the Addison disease, a chronic primary insufficiency of disease: oral mucous membrane hyperpigmenta- the adrenal glands, results in both glucocorticoid and tion. We describe this unique type of discolor- mineralocorticoid deficiency. Historically, tuberculo- ation in detail and contrast it with other forms of sis accounted for most cases of Addison disease.1 oral pigmentation. Autoimmune destruction of the adrenal glands, also Cutis. 2005;76:97-99. known as autoimmune adrenalitis, is now the most common cause of Addison disease in both children and adults.2,3 Autoimmune destruction of other Case Report endocrine tissues can occur concurrently. These A 9-year-old girl presented with a 4-month history polyglandular autoimmune syndromes are associated of painless black patches on the tongue and gingiva. with hypoparathyroidism, pernicious anemia, and The patches had persisted despite treatment with chronic mucocutaneous candidiasis (type 1); diabetes oral fluconazole, which had been prescribed empiri- mellitus (type 2); or thyroiditis (type 3).4 Type 3, cally for presumed oral candidiasis. Results of a phys- however, consists of an autoimmune thyroiditis ical examination revealed scattered, asymptomatic, syndrome in the absence of Addison disease.5 bluish-black macules on the dorsal surface of the Although most children (75%) presenting with isolated tongue, the mucosal surface of the lower lip, and the Addison disease are boys,6 type 1 autoimmune poly- hard palate (Figure). -

The OHNEP Interprofessional Oral Health Faculty Toolkit
The OHNEP Interprofessional Oral Health Faculty Toolkit Adult-Gerontology Nurse Practitioner Program CURRICULUM INTEGRATION OF INTERPROFESSIONAL ORAL HEALTH CORE COMPETENCIES: • Adult-Gerontology Health Assessment • Adult-Gerontology Health Promotion • Adult-GerontologyPrimary Care • Resources © Oral Health Nursing Education and Practice (OHNEP) INTRODUCTION The Oral Health Nursing Education and Practice (OHNEP) program has developed an Interprofessional Oral Health Faculty Tool Kit to S! provide you with user friendly curriculum templates and teaching-learning resources to use when integrating oral health and its links to ! overall health in your Adult-Gerontology Nurse Practitioner program. ! Oral health and its relation to overall health has been identified as an important population health issue. Healthy People 2020 (2011), the IOM Reports, Advancing Oral Health in America (2011) and Building Workforce Capacity in Oral Health (2011), as well as the IPEC Competencies ! (2011), challenged HRSA to develop interprofessional oral health core competencies for primary care providers. Publication of the report, ! Integrating Oral Health in Primary Care Practice (2014), reflects those interprofessional oral health competencies that can be used by Adult- Gerontology Nurse Practitioners for faculty development, curriculum integration and establishment of “best practices” in clinical settings. ! The HRSA interprofessional oral health core competencies, the IPEC competencies and the NONPF core competencies provide the framework for the curriculum templates and resources. Exciting teaching-learning strategies that take students from Exposure to Immersion to Competence can begin in the classroom, link to simulated or live clinical experiences and involve community-based service learning, advocacy and policy initiatives as venues you can readily use to integrate oral health into your existing primary care curriculum. -

Adverse Effects of Medications on Oral Health
Adverse Effects of Medications on Oral Health Dr. James Krebs, BS Pharm, MS, PharmD Director of Experiential Education College of Pharmacy, University of New England Presented by: Rachel Foster PharmD Candidate, Class of 2014 University of New England October 2013 Objectives • Describe the pathophysiology of various medication-related oral reactions • Recognize the signs and symptoms associated with medication-related oral reactions • Identify the populations associated with various offending agents • Compare the treatment options for medication-related oral reactions Medication-related Oral Reactions • Stomatitis • Oral Candidiasis • Burning mouth • Gingival hyperplasia syndrome • Alterations in • Glossitis salivation • Erythema • Alterations in taste Multiforme • Halitosis • Oral pigmentation • Angioedema • Tooth discoloration • Black hairy tongue Medication-related Stomatitis • Clinical presentation – Aphthous-like ulcers, mucositis, fixed-drug eruption, lichen planus1,2 – Open sores in the mouth • Tongue, gum line, buccal membrane – Patient complaint of soreness or burning http://www.virtualmedicalcentre.com/diseases/oral-mucositis-om/92 0 http://www.virtualmedicalcentre.com/diseases/oral-mucositis-om/920 Medication-related Stomatitis • Offending agents1,2 Medication Indication Patient Population Aspirin •Heart health • >18 years old •Pain reliever • Cardiac patients NSAIDs (i.e. Ibuprofen, •Headache General population naproxen) •Pain reliever •Fever reducer Chemotherapy (i.e. •Breast cancer •Oncology patients methotrexate, 5FU, •Colon -

BIMJ April 2013
Original Article Brunei Int Med J. 2013; 9 (5): 290-301 Yellow lesions of the oral cavity: diagnostic appraisal and management strategies Faraz MOHAMMED 1, Arishiya THAPASUM 2, Shamaz MOHAMED 3, Halima SHAMAZ 4, Ramesh KUMARASAN 5 1 Department of Oral & Maxillofacial Pathology, Dr Syamala Reddy Dental College Hospital & Research Centre, Bangalore, India 2 Department of Oral Medicine & Radiology, Dr Syamala Reddy Dental College Hospital & Research Centre, Bangalore, India 3 Department of Community & Public Health Dentistry, Faculty of Dentistry, Amrita University, Cochin, India 4 Amrita center of Nanosciences, Amrita University, Cochin, India 5 Oral and Maxillofacial Surgery, Faculty of Dentistry, AIMST University, Kedah, Malaysia ABSTRACT Yellow lesions of the oral cavity constitute a rather common group of lesions that are encountered during routine clinical dental practice. The process of clinical diagnosis and treatment planning is of great concern to the patient as it determines the nature of future follow up care. There is a strong need for a rational and functional classification which will enable better understanding of the basic disease process, as well as in formulating a differential diagnosis. Clinical diagnostic skills and good judgment forms the key to successful management of yellow lesions of the oral cavity. Keywords: Yellow lesions, oral cavity, diagnosis, management INTRODUCTION INTRODUCTI Changes in colour have been traditionally low lesions have a varied prognostic spec- used to register and classify mucosal and soft trum. The yellowish colouration may be tissue pathology of the oral cavity. Thus, the- caused by lipofuscin (the pigment of fat). It se lesions have been categorised as white, may also be the result of other causes such red, white and red, blue and/or purple, as accumulation of pus, aggregation of lym- brown, grey and/or black and yellow. -

Hairy Leukoplakia James E
Marquette University e-Publications@Marquette School of Dentistry Faculty Research and Dentistry, School of Publications 5-5-2017 Hairy Leukoplakia James E. Cade Meharry Medical College School of Dentistry Richard P. Vinson Paul L Foster School of Medicine Jeff urB gess University of Washington School of Dental Medicine Sanjiv S. Agarwala Temple University Shool of Medicine Denis P. Lynch Marquette University, [email protected] See next page for additional authors Published version. Medscape Drugs & Diseases (May 5, 2017). Publisher link. © 2017 by WebMD LLC. Used with permission. Authors James E. Cade, Richard P. Vinson, Jeff urB gess, Sanjiv S. Agarwala, Denis P. Lynch, and Gary L. Stafford This blog post/website is available at e-Publications@Marquette: https://epublications.marquette.edu/dentistry_fac/252 Overview Background Oral hairy leukoplakia (OHL) is a disease of the mucosa first described in 1984. This pathology is associated with Epstein-Barr virus (EBV) and occurs mostly in people with HIV infection, both immunocompromised and immunocompetent, and can affect patients who are HIV negative.{ref1}{ref2} The first case in an HIV-negative patient was reported in 1999 in a 56-year-old patient with acute lymphocytic leukemia. Later, many cases were reported in heart, kidney, and bone marrow transplant recipients and patients with hematological malignancies.{ref3}{ref4} Pathophysiology The Epstein-Barr virus (EBV), a ubiquitous herpesvirus estimated to infect 90% of the world's population, is linked to a growing number of diseases, especially in immunocompromised hosts. Like all herpesviruses, EBV establishes a life-long, persistent infection of its host. The pathogenesis of hairy leukoplakia is clearly complex, potentially requiring a convergence of factors including EBV co-infection, productive EBV replication, EBV genetic evolution, expression of specific EBV "latent" genes, and immune escape. -
A Concise Guide to Treating Painful Oral Lesions
Drugs Used to Treat Osteoporosis and Bone Cancer Perio & Implant Centers The Team for of the Monterey Bay (831) 648-8800 Jochen P. Pechak, DDS, MSD in Silicon Valley (408) 738-3423 Which May Cause Osteonecrosis of the Jaws mobile: www.DrPechakapp.com he many bisphosphonates and monoclonal antibodies which are used to treat osteoporosis and bone cancer often web: GumsRus.com causeDrugsDrugs osteonecrosis Used Used of the to jaws.to Treat AsTreat dental clinicians,Osteoporosis Osteoporosis it is important that and andwe are Bone awareBone of this Cancers Cancers side effect before Ttreating our patients who are taking these drugs. The tables below summarize these drugs, the route these drugs are administered, andWhich Whichtheir likelihood May May of causing Cause Cause osteonecrosis Osteonecrosis Osteonecrosis of the jaws as reported byof of Dr. the theRobert Jaws JawsMarx at the University of Miami Division of Oral and Maxillofacial Surgery. PDL tm Osteoporosis Drugs Drugs Osteoporosis Used to Treat Drugs Osteoporosis PerioDontaLetter Jochen P. Pechak, DDS, MSD, Periodontics and Implant Dentistry Spring DrugDrug ClassificationClassification ActionAction DoseDose RouteRoute %% of of ReportedReported CasesCases of of OsteonecrosisOsteonecrosis AlendronateAlendronate BisphosphonateBisphosphonate OsteoclastOsteoclast 7070 mg/wk mg/wk OralOral 8282%% From Our Office A Concise Guide to Treating (Fosamax(Fosamax ToxicityToxicity to Yours... Generic)Generic) Painful Oral Lesions ResidronateResidronate BisphosphonateBisphosphonate OsteoclastOsteoclast 3535 mg/wk mg/wk OralOral 1%1% As dentists specializing in treat- (Actonel Toxicity (Actonel Toxicity ment of diseases of the oral cavity atients present frequently with Treating Cold Sores Atelvia)Atelvia) and associated structures, we are painful oral lesions. They are often also called upon to treat pain- IbandronateIbandronate BisphosphonateBisphosphonate OsteoclastOsteoclast 150150 mg/mos mg/mos OralOral 1%1% usually not serious, but patients And Canker Sores (Boniva) Toxicity IV ful oral lesions in the mouth. -

On the Tip of the Tongue
KNOWLEDGE TO PRACTICE DES CONNAISSANCES ÀLA PRATIQUE Diagnostic Challenge On the tip of the tongue . Rachel Orchard, MD*; Sheena Belisle, MD†; Rodrick Lim, MD†‡ Keywords: pediatric, rash, tongue, vesicle right-sided wheeze. Cardiovascular, abdominal, and neurological (including cranial nerve) examinations were unremarkable. CASE HISTORY What is the most likely diagnosis? A 14-year-old male presented to the pediatric emer- a) Drug eruption gency department (ED) with a chief complaint of b) Varicella zoster virus (VZV) changes to his tongue. He described a 3-day history of a c) Oral candidiasis gradually worsening sore, swollen tongue associated with a white plaque. This was accompanied by a 3-day d) Epstein-Barr virus history of a gradually worsening left-sided facial rash e) Oral lichen planus that had an intermittent mild tingling sensation. He also had a 1-week history of a productive cough with yellow mucus and generalized malaise. He had been seen at a walk-in clinic 2 days prior to presentation and was prescribed amoxicillin for presumed pneumo- nia, which he began the same day. He denied any history of fevers, facial weakness, neck stiffness, or eye symptoms. He was an otherwise well child, with up-to-date immunizations and a past medical history of chickenpox and recurrent furuncles as a younger child. On examination, he appeared well with the following vital signs: blood pressure 122/64 mm Hg, heart rate 73 beats per minute, respiratory rate 18 breaths per minute, temperature 36.8°C, and oxygen saturation of 99% on room air. Examination of his tongue revealed a symmetric white plaque along with ulcerative lesions on the left tongue and buccal mucosa (Figure 1). -

Pathogenic Viruses Commonly Present in the Oral Cavity and Relevant Antiviral Compounds Derived from Natural Products
medicines Review Pathogenic Viruses Commonly Present in the Oral Cavity and Relevant Antiviral Compounds Derived from Natural Products Daisuke Asai and Hideki Nakashima * Department of Microbiology, St. Marianna University School of Medicine, Kawasaki 216-8511, Japan * Correspondence: [email protected]; Tel.: +81-44-977-8111 Received: 24 October 2018; Accepted: 7 November 2018; Published: 12 November 2018 Abstract: Many viruses, such as human herpesviruses, may be present in the human oral cavity, but most are usually asymptomatic. However, if individuals become immunocompromised by age, illness, or as a side effect of therapy, these dormant viruses can be activated and produce a variety of pathological changes in the oral mucosa. Unfortunately, available treatments for viral infectious diseases are limited, because (1) there are diseases for which no treatment is available; (2) drug-resistant strains of virus may appear; (3) incomplete eradication of virus may lead to recurrence. Rational design strategies are widely used to optimize the potency and selectivity of drug candidates, but discovery of leads for new antiviral agents, especially leads with novel structures, still relies mostly on large-scale screening programs, and many hits are found among natural products, such as extracts of marine sponges, sea algae, plants, and arthropods. Here, we review representative viruses found in the human oral cavity and their effects, together with relevant antiviral compounds derived from natural products. We also highlight some recent emerging pharmaceutical technologies with potential to deliver antivirals more effectively for disease prevention and therapy. Keywords: anti-human immunodeficiency virus (HIV); antiviral; natural product; human virus 1. Introduction The human oral cavity is home to a rich microbial flora, including bacteria, fungi, and viruses.