Oral and Maxillo-Facial Manifestations of Systemic Diseases: an Overview
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lumps and Swellings
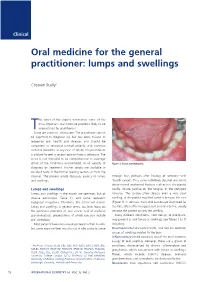
Clinical Oral medicine for the general practitioner: lumps and swellings Crispian Scully 1 his series of five papers summarises some of the most important oral medicine problems likely to be Tencountered by practitioners. Some are common, others rare. The practitioner cannot be expected to diagnose all, but has been trained to recognise oral health and disease, and should be competent to recognise normal variants, and common orofacial disorders. In any case of doubt, the practitioner is advised to seek a second opinion from a colleague. The series is not intended to be comprehensive in coverage either of the conditions encountered, or all aspects of Figure 1: Torus mandibularis. diagnosis or treatment: further details are available in standard texts, in the further reading section, or from the internet. The present article discusses aspects of lumps through fear, perhaps after hearing of someone with and swellings. ‘mouth cancer’. Thus some individuals discover and worry about normal anatomical features such as tori, the parotid Lumps and swellings papilla, foliate papillae on the tongue, or the pterygoid Lumps and swellings in the mouth are common, but of hamulus. The tongue often detects even a very small diverse aetiologies (Table 1), and some represent swelling, or the patient may first notice it because it is sore malignant neoplasms. Therefore, this article will discuss (Figure 1). In contrast, many oral cancers are diagnosed far lumps and swellings in general terms, but later focus on too late, often after being present several months, usually the particular problems of oral cancer and of orofacial because the patient ignores the swelling. -

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

Related Osteonecrosis of the Jaw in Patients with Sjögren's Syndrome
Open access Research BMJ Open: first published as 10.1136/bmjopen-2018-024655 on 13 February 2019. Downloaded from Increased risk of bisphosphonate- related osteonecrosis of the jaw in patients with Sjögren’s syndrome: nationwide population-based cohort study Min-Tser Liao,1,2 Wu-Chien Chien,3,4,5 Jen-Chun Wang,6 Chi-Hsiang Chung,3,4,7 Shi-Jye Chu,8 Shih-Hung Tsai6,9 To cite: Liao M-T, Chien W-C, ABSTRACT Strengths and limitations of this study Wang J-C, et al. Increased Objective The aim of this study was to explore whether risk of bisphosphonate- patients with Sjögren’s syndrome (SS) were susceptible ► The strength of our study is its population-based related osteonecrosis of to bisphosphonate (BP)-related osteonecrosis of the jaw the jaw in patients with cohort design with a large number of patients and (BRONJ) after tooth extraction in the entire population of Sjögren’s syndrome: long-term follow-up, which aims to evaluate the Taiwan. nationwide population-based association between Sjögren’s syndrome and os- Design A nationwide population-based retrospective cohort study. BMJ Open teonecrosis of the jaw (ONJ) after tooth extraction. 2019;9:e024655. doi:10.1136/ cohort study. ► The National Health Insurance Research Database Setting Data were extracted from Taiwan’s National bmjopen-2018-024655 registry could not provide detailed information re- Health Insurance Research Database (NHIRD). Prepublication history and garding laboratory results, family histories and ► Methodology Medical conditions for both the study and additional material for this health-related lifestyle factors. control group were categorised using the International paper are available online. -

Psoriasis, a Systemic Disease Beyond the Skin, As Evidenced by Psoriatic Arthritis and Many Comorbities
1 Psoriasis, a Systemic Disease Beyond the Skin, as Evidenced by Psoriatic Arthritis and Many Comorbities – Clinical Remission with a Leishmania Amastigotes Vaccine, a Serendipity Finding J.A. O’Daly Astralis Ltd, Irvington, NJ USA 1. Introduction Psoriasis is a systemic chronic, relapsing inflammatory skin disorder, with worldwide distribution, affects 1–3% of the world population, prevalence varies according to race, geographic location, and environmental factors (Chandran & Raychaudhuri, 2010; Christophers & Mrowietz, 2003; Farber & Nall, 1974). In Germany, 33,981 from 1,344,071 continuously insured persons in 2005 were diagnosed with psoriasis; thus the one year prevalence was 2.53% in the study group. Up to the age of 80 years the prevalence rate (range: 3.99-4.18%) was increasing with increasing age and highest for the age groups from 50 to 79 years The total rate of psoriasis in children younger than 18 years was 0.71%. The prevalence rates increased in an approximately linear manner from 0.12% at the age of 1 year to 1.2% at the age of 18 years (Schäfer et al., 2011). In France, a case-control study in 6,887 persons, 356 cases were identified (5.16%), who declared having had psoriasis during the previous 12 months (Wolkenstein et al., 2009). The prevalence of psoriasis analyzed across Italy showed that 2.9% of Italians declared suffering from psoriasis (regional range: 0.8-4.5%) in a total of 4109 individuals (Saraceno et al., 2008). The overall rate of comorbidity in subjects with psoriasis aged less than 20 years was twice as high as in subjects without psoriasis. -

• Acute Pericoronitis • End-Stage Renal Disease • Acute Infectious Stomatitis an Acute Apical Abscess Should Not Be a Contraindication to Extraction
• acute pericoronitis • end-stage renal disease • acute infectious stomatitis An acute apical abscess should not be a contraindication to extraction. It has been shown that these infections can resolve very quickly when the affected tooth is removed. However, it may be diffi - cult to extract such a tooth, either because the patient is unable to open sufficiently wide enough or because adequate local anesthesia cannot be obtained. There are few true contraindications to the extraction of teeth. Note: In some instances, the pa - tients’ health may be so compromised that they cannot withstand the surgical procedure. Examples of contraindications include: • End-stage renal disease • Severe uncontrolled metabolic diseases (i.e., uncontrolled diabetes mellitus) • Advanced cardiac conditions (unstable angina) • Patients with leukemia and lymphoma should be treated before extraction of teeth • Patients with hemophilia or platelet disorders should be treated before extraction of teeth • Patients with a history of head and neck cancer need to be treated with care because even minor surgery can lead to osteoradionecrosis. Note: These patients are often treated with hyperbaric oxygen therapy prior to (20 sessions) and following extractions (10 sessions). • Pericoronitis: infection of the soft tissues around a partially erupted mandibular third molar Note: This infection should be treated prior to removal of the maxillary third molar. • Acute infectious stomatitis and malignant disease are relative contraindications • Treatment with IV bisphosphonates increases the risk of osteonecrosis of the jaw Note: Causes of excessive bleeding after dental extractions include: injury to the inferior alveolar artery during extraction of a mandibular tooth (usually the third molar), a muscular arteriolar bleed from a flap procedure, or bleeding related to the patient’s history (i.e., patients who are on warfarin or drugs for platelet inhibition, patients who have hemophilia or von Willebrand disease, or who have chronic liver insufficiency).. -

Pediatric Oral Pathology. Soft Tissue and Periodontal Conditions
PEDIATRIC ORAL HEALTH 0031-3955100 $15.00 + .OO PEDIATRIC ORAL PATHOLOGY Soft Tissue and Periodontal Conditions Jayne E. Delaney, DDS, MSD, and Martha Ann Keels, DDS, PhD Parents often are concerned with “lumps and bumps” that appear in the mouths of children. Pediatricians should be able to distinguish the normal clinical appearance of the intraoral tissues in children from gingivitis, periodontal abnormalities, and oral lesions. Recognizing early primary tooth mobility or early primary tooth loss is critical because these dental findings may be indicative of a severe underlying medical illness. Diagnostic criteria and .treatment recommendations are reviewed for many commonly encountered oral conditions. INTRAORAL SOFT-TISSUE ABNORMALITIES Congenital Lesions Ankyloglossia Ankyloglossia, or “tongue-tied,” is a common congenital condition characterized by an abnormally short lingual frenum and the inability to extend the tongue. The frenum may lengthen with growth to produce normal function. If the extent of the ankyloglossia is severe, speech may be affected, mandating speech therapy or surgical correction. If a child is able to extend his or her tongue sufficiently far to moisten the lower lip, then a frenectomy usually is not indicated (Fig. 1). From Private Practice, Waldorf, Maryland (JED); and Department of Pediatrics, Division of Pediatric Dentistry, Duke Children’s Hospital, Duke University Medical Center, Durham, North Carolina (MAK) ~~ ~ ~ ~ ~ ~ ~ PEDIATRIC CLINICS OF NORTH AMERICA VOLUME 47 * NUMBER 5 OCTOBER 2000 1125 1126 DELANEY & KEELS Figure 1. A, Short lingual frenum in a 4-year-old child. B, Child demonstrating the ability to lick his lower lip. Developmental Lesions Geographic Tongue Benign migratory glossitis, or geographic tongue, is a common finding during routine clinical examination of children. -

Two Cases of Nevoid Basal Cell Carcinoma Syndrome in One Family
221 Two Cases of Nevoid Basal Cell Carcinoma Syndrome in One Family Dong Jin Ryu, M.D., Yeon Sook Kwon, M.D., Mi Ryung Roh, M.D., Min-Geol Lee, M.D., Ph.D. Department of Dermatology and Cutaneous Biology Research Institute, Yonsei University College of Medicine, Seoul, Korea The nevoid basal cell carcinoma syndrome, or Gorlin-Goltz syndrome, is an autosomal dominant multiple system disorder with high penetrance and variable expressions, although it can also arise spontaneously. The diagnostic criteria for nevoid basal cell carcinoma syndrome include multiple basal cell carcinomas, palmoplantar pits, multiple odontogenic keratocysts, skeletal anomalies, positive family history, ectopic calcification and neurological anomalies. We report a brother and sister who were both diagnosed with nevoid basal cell carcinoma syndrome. (Ann Dermatol (Seoul) 20(4) 221∼225, 2008) Key Words: Basal cell carcinoma, Nevoid basal cell carcinoma syndrome, Odontogenic keratocyst INTRODUCTION cell carcinoma syndrome. The nevoid basal cell carcinoma syndrome (NBCCS), or Gorlin-Goltz syndrome, is an auto- CASE REPORT somal dominant multiple system disorder with high 1 penetrance and variable expressions . However, Case 1 60% of patients with NBCCS are sporadic cases. It An 11-year-old male was referred to our depart- has an estimated prevalence of 1 in 60,000 with ment for the evaluation of multiple miliary sized 2 equal distributions among males and females . The pigmented macules on the palm and sole that had well-defined diagnostic criteria include cutaneous increased in number over several years. He had an anomalies, dento-facial anomalies, skeletal ano- operation for inguinal hernia at 3 years of age, but malies, positive family history, neurological ano- no other medical problems. -

Oral Lesions in Sjögren's Syndrome
Med Oral Patol Oral Cir Bucal. 2018 Jul 1;23 (4):e391-400. Oral lesions in Sjögren’s syndrome patients Journal section: Oral Medicine and Pathology doi:10.4317/medoral.22286 Publication Types: Review http://dx.doi.org/doi:10.4317/medoral.22286 Oral lesions in Sjögren’s syndrome: A systematic review Julia Serrano 1, Rosa-María López-Pintor 1, José González-Serrano 1, Mónica Fernández-Castro 2, Elisabeth Casañas 1, Gonzalo Hernández 1 1 Department of Oral Medicine and Surgery, School of Dentistry, Complutense University, Madrid, Spain 2 Rheumatology Service, Hospital Infanta Sofía, Madrid, Spain Correspondence: Departamento de Especialidades Clínicas Odontológicas Facultad de Odontología Universidad Complutense de Madrid Plaza Ramón y Cajal s/n, 28040 Madrid. Spain [email protected] Serrano J, López-Pintor RM, González-Serrano J, Fernández-Castro M, Casañas E, Hernández G. Oral lesions in Sjögren’s syndrome: A system- atic review. Med Oral Patol Oral Cir Bucal. 2018 Jul 1;23 (4):e391-400. Received: 18/11/2017 http://www.medicinaoral.com/medoralfree01/v23i4/medoralv23i4p391.pdf Accepted: 09/05/2018 Article Number: 22291 http://www.medicinaoral.com/ © Medicina Oral S. L. C.I.F. B 96689336 - pISSN 1698-4447 - eISSN: 1698-6946 eMail: [email protected] Indexed in: Science Citation Index Expanded Journal Citation Reports Index Medicus, MEDLINE, PubMed Scopus, Embase and Emcare Indice Médico Español Abstract Background: Sjögren’s syndrome (SS) is an autoimmune disease related to two common symptoms: dry mouth and eyes. Although, xerostomia and hyposialia have been frequently reported in these patients, not many studies have evaluated other oral manifestations. -
Benign Migratory Glossitis: Case Report and Literature Review
Volume 1- Issue 5 : 2017 DOI: 10.26717/BJSTR.2017.01.000482 Sarfaraz Khan. Biomed J Sci & Tech Res ISSN: 2574-1241 Case Report Open Access Benign Migratory Glossitis: Case Report and Literature Review Sarfaraz Khan1*, Syed AsifHaider Shah2, Tanveer Ahmed Mujahid3 and Muhammad Ishaq4 1Consultant Oral and Maxillofacial Surgeon, Pak Field Hospital Darfur, Sudan 2MDC Gujranwala, Pakistan 3Consultant Dermatologist, Pak Field Hospital Darfur, Sudan 4Registrar Dermatologist, Pak Field Hospital Darfur, Sudan Received: October 25, 2017; Published: October 31, 2017 *Corresponding author: Sarfaraz Khan, Consultant Oral and Maxillofacial Surgeon, Pakistan Field Hospital Darfur, Sudan, Tel: ; Email: Abstract Benign migratory Glossitis (BMG) is a benign, usually asymptomatic mucosal lesion of dorsal surface of the tongue, characterized by depapillated erythematous patches separated by white irregular borders. Etiology of BMG is unknown. Risk factors include psoriasis, fissured tongue, diabetes mellitus, hypersensitivity and psychological factors. We report BMG in an Egyptian soldier of UN peace keeping force, with stressKeywords: as a possible Geographic etiological tongue; factor Benign and migratory provide literature Glossitis; reviewErythema of this migrans disorder. Introduction Benign migratory Glossitis (BMG) is a benign, immune- spicy/salty food and/or alcoholic drinks [4,5].The lesion typically usually characterized by asymptomatic erythematous patches changes its shape with time owing to the change in pattern of mediated, chronic inflammatory lesion of unknown etiology, depapillation.Similar lesions may also be seen in atrophic candidiasis, local chemical or mechanical trauma, drug induced reactions, psoriasis with whitish margins across the surface of the tongue. This condition is also known as geographic tongue, erythema migrans, Treatment of symptomatic BMG aims at provision of symptomatic Glossitis exfoliativa and wandering rash of the tongue. -

Case Report Treatment of Geographic Tongue
Scholars Journal of Dental Sciences (SJDS) ISSN 2394-496X (Online) Sch. J. Dent. Sci., 2015; 2(7):409-413 ISSN 2394-4951 (Print) ©Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources) www.saspublisher.com Case Report Treatment of Geographic Tongue Superimposing Fissured Tongue: A literature review with case report Jalaleddin H Hamissi1, Mahsa EsFehani2, Zahra Hamissi3 1Associate Professor in periodontics and Dental Caries Prevention Research Center, Qazvin University Medical Sciences, Qazvin, Iran. 2Assistant Professor, Department of Oral Medicine & Diagnosis, college dentistry, Qazvin University Medical Sciences, Qazvin, Iran. 3Dental Student, College of Dentistry, Shahied Behesti University of Medical Sciences, Teheran, Iran *Corresponding author Dr Jalaleddin H Hamissi Email: [email protected] ; [email protected] Abstract: Tongue is a most sensitive part of the oral cavity. It is responsible for many functions in the mouth like swallowing, speech, mastication, speaking and breathing. Geographic tongue (Benign migratory glossitis, erythema migrans) is an asymptomatic inflammatory disorder of tongue with controversial etiology. This disease is characterized by erythematous areas showing raised greyish or white circinate lines or bands with irregular pattern on the dorsal surface of the tongue and depapillation. The objective in presenting the case report and literature review is to discuss the clinical presentation, associated causative factors and management strategies of geographic tongue. Keywords: Asymptomatic; Characteristics; Fissured tongue; Geographic tongue; Migratory INTRODUCTION in approximately three percent (3%) majority of female Geographic tongue is an asymptomatic population [9]. On other aspects of oral mucosa, such as inflammatory condition of the dorsum of tongue on commissure of lip, floor of mouth, cheek etc., which occasionally extending towards the lateral borders. -

Oral Manifestations of Systemic Disease Their Clinical Practice
ARTICLE Oral manifestations of systemic disease ©corbac40/iStock/Getty Plus Images S. R. Porter,1 V. Mercadente2 and S. Fedele3 provide a succinct review of oral mucosal and salivary gland disorders that may arise as a consequence of systemic disease. While the majority of disorders of the mouth are centred upon the focus of therapy; and/or 3) the dominant cause of a lessening of the direct action of plaque, the oral tissues can be subject to change affected person’s quality of life. The oral features that an oral healthcare or damage as a consequence of disease that predominantly affects provider may witness will often be dependent upon the nature of other body systems. Such oral manifestations of systemic disease their clinical practice. For example, specialists of paediatric dentistry can be highly variable in both frequency and presentation. As and orthodontics are likely to encounter the oral features of patients lifespan increases and medical care becomes ever more complex with congenital disease while those specialties allied to disease of and effective it is likely that the numbers of individuals with adulthood may see manifestations of infectious, immunologically- oral manifestations of systemic disease will continue to rise. mediated or malignant disease. The present article aims to provide This article provides a succinct review of oral manifestations a succinct review of the oral manifestations of systemic disease of of systemic disease. It focuses upon oral mucosal and salivary patients likely to attend oral medicine services. The review will focus gland disorders that may arise as a consequence of systemic upon disorders affecting the oral mucosa and salivary glands – as disease. -

Acquired Bilateral Nevus of Ota–Like Macules (Hori's Nevus): a Case
Acquired Bilateral Nevus of Ota–like Macules (Hori’s Nevus): A Case Report and Treatment Update Jamie Hale, DO,* David Dorton, DO,** Kaisa van der Kooi, MD*** *Dermatology Resident, 2nd year, Largo Medical Center/NSUCOM, Largo, FL **Dermatologist, Teaching Faculty, Largo Medical Center/NSUCOM, Largo, FL ***Dermatopathologist, Teaching Faculty, Largo Medical Center/NSUCOM, Largo, FL Abstract This is a case of a 71-year-old African American female who presented with bilateral periorbital hyperpigmentation. After failing treatment with a topical retinoid and hydroquinone, a biopsy was performed and was consistent with acquired bilateral nevus of Ota-like macules, or Hori’s nevus. A review of histopathology, etiology, and treatment is discussed below. cream and tretinoin 0.05% gel. At this visit, a Introduction Figure 2 Acquired nevus of Ota-like macules (ABNOM), punch biopsy of her left zygoma was performed. or Hori’s nevus, clinically presents as bilateral, Histopathology reported sparse proliferation blue-gray to gray-brown macules of the zygomatic of irregularly shaped, haphazardly arranged melanocytes extending from the superficial area. It less often presents on the forehead, upper reticular dermis to mid-deep reticular dermis outer eyelids, and nose.1 It is most common in women of Asian descent and has been reported Figure 4 in ages 20 to 70. Classically, the eye and oral mucosa are uninvolved. This condition is commonly misdiagnosed as melasma.1 The etiology of this condition is not fully understood, and therefore no standardized treatment has been Figure 3 established. Case Report A 71-year-old African American female initially presented with a two week history of a pruritic, flaky rash with discoloration of her face.