Orofacial Granulomatosis Presenting As Gingival Enlargement – Report of Three Cases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lumps and Swellings
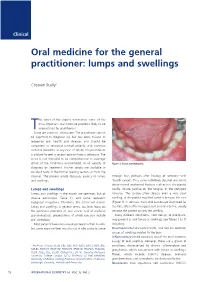
Clinical Oral medicine for the general practitioner: lumps and swellings Crispian Scully 1 his series of five papers summarises some of the most important oral medicine problems likely to be Tencountered by practitioners. Some are common, others rare. The practitioner cannot be expected to diagnose all, but has been trained to recognise oral health and disease, and should be competent to recognise normal variants, and common orofacial disorders. In any case of doubt, the practitioner is advised to seek a second opinion from a colleague. The series is not intended to be comprehensive in coverage either of the conditions encountered, or all aspects of Figure 1: Torus mandibularis. diagnosis or treatment: further details are available in standard texts, in the further reading section, or from the internet. The present article discusses aspects of lumps through fear, perhaps after hearing of someone with and swellings. ‘mouth cancer’. Thus some individuals discover and worry about normal anatomical features such as tori, the parotid Lumps and swellings papilla, foliate papillae on the tongue, or the pterygoid Lumps and swellings in the mouth are common, but of hamulus. The tongue often detects even a very small diverse aetiologies (Table 1), and some represent swelling, or the patient may first notice it because it is sore malignant neoplasms. Therefore, this article will discuss (Figure 1). In contrast, many oral cancers are diagnosed far lumps and swellings in general terms, but later focus on too late, often after being present several months, usually the particular problems of oral cancer and of orofacial because the patient ignores the swelling. -

Review: Differential Diagnosis of Drug-Induced Gingival Hyperplasia and Other Oral Lesions
ISSN: 2469-5734 Moshe. Int J Oral Dent Health 2020, 6:108 DOI: 10.23937/2469-5734/1510108 Volume 6 | Issue 2 International Journal of Open Access Oral and Dental Health REVIEW ARTICLE Review: Differential Diagnosis of Drug-Induced Gingival Hyper- plasia and Other Oral Lesions Einhorn Omer Moshe* Private Dental Office, Israel Check for *Corresponding author: Einhorn Omer Moshe, Private Dental Office, Dr. Einhorn, 89 Medinat Hayehudim updates street, Herzliya, Israel tooth discoloration, alteration of taste sensation and Abstract even appearance of lesions on the tissues of the oral Chronic medication usage is a major component of the cavity. Early recognition and diagnosis of these effects medical diagnosis of patients. Nowadays, some of the most common diseases such as cancer, hypertension, diabetes can largely assist in the prevention of further destruc- and etc., are treated with drugs which cause a variety of oral tive consequences in patients’ health status. As life ex- side-effects including gingival over growth and appearance pectancy increases, the number of elderly patients in of lesions on the tissues of the oral cavity. As such, drug-in- the dental practice also rises. Individuals of this popula- duced oral reactions are an ordinary sight in the dental prac- tice. This review will point out the main therapeutic agents tion are usually subjected to chronic medication intake causing gingival hyperplasia and other pathologic lesions which requires the clinician to be aware of the various in the oral cavity. Some frequently used medications, in side-effects accompanying these medications. This re- particular antihypertensives, nonsteroidal anti-inflammatory view will point out the main therapeutic agents causing drugs and even antibiotics, can lead to overgrowth of the gingival hyperplasia and other pathologic lesions in the gingiva and to the multiple unwanted conditions, namely: Lupus erythematosus, erythema multiforme, mucositis, oral oral cavity. -

Orofacial Granulomatosis
Al-Hamad, A; Porter, S; Fedele, S; (2015) Orofacial Granulomatosis. Dermatol Clin , 33 (3) pp. 433- 446. 10.1016/j.det.2015.03.008. Downloaded from UCL Discovery: http://discovery.ucl.ac.uk/1470143 ARTICLE Oro-facial Granulomatosis Arwa Al-Hamad1, 2, Stephen Porter1, Stefano Fedele1, 3 1 University College London, UCL Eastman Dental Institute, Oral Medicine Unit, 256 Gray’s Inn Road, WC1X 8LD, London UK. 2 Dental Services, King Abdulaziz Medical City-Riyadh, Ministry of National Guard, Riyadh, Saudi Arabia. 3 NIHR University College London Hospitals Biomedical Research Centre, London, UK. Acknowledgments: Part of this work was undertaken at University College London/University College London Hospital, which received a proportion of funding from the Department of Health’s National Institute for Health Research Biomedical Research Centre funding scheme. Conflicts of Interest: The authors declare that they have no affiliation with any organization with a financial interest, direct or indirect, in the subject matter or materials discussed in the manuscript that may affect the conduct or reporting of the work submitted. Authorship: all authors named above meet the following criteria of the International Committee of Medical Journal Editors: 1) Substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; 2) Drafting the article or revising it critically for important intellectual content; 3) Final approval of the version to be published. Corresponding author: Dr. Stefano Fedele DDS, PhD -

Chronic Inflammatory Gingival Enlargement and Treatment: a Case Report
Case Report Adv Dent & Oral Health Volume 9 Issue 4- July 2018 Copyright © All rights are reserved by Mehmet Özgöz DOI: 10.19080/ADOH.2018.09.555766 Chronic Inflammatory Gingival Enlargement and Treatment: A Case Report Mehmet Özgöz1* and Taner Arabaci2 1Department of Periodontology, Akdeniz University, Turkey 2Department of Periodontology, Atatürk University, Turkey Submission: June 14, 2018; Published: July 18, 2018 *Corresponding author: Özgöz, Department of Periodontology, Akdeniz University Faculty of Dentistry, Antalya, Turkey, Fax:+902423106967; Email: Abstract Gingival enlargement is a common feature in gingival disease. If gingival enlargement isn’t treated, it may some aesthetic problems, plaque accumulation,Keywords: Gingival gingival enlargement; bleeding, and Periodontal periodontitis. treatments; In this paper, Etiological inflammatory factors; Plasma gingival cell enlargement gingivitis and treatment was presented. Introduction and retention include poor oral hygiene, abnormal relationship of Gingival enlargement is a common feature in gingival disease adjacent teeth, lack of tooth function, cervical cavities, improperly contoured dental restorations, food impaction, nasal obstruction, connection with etiological factors and pathological changes [3-5]. [1,2]. Many types of gingival enlargement can be classified in orthodontic therapy involving repositioning of the teeth, and habits such as mouth breathing and pressing the tongue against the gingival [18-20]. a)b) InflammatoryDrug-induced enlargement:enlargement [7-12]. chronic and acute [6]. c) Gingival enlargements associated with systemic diseases: patients to maintain oral hygiene [9,21]. Surgical correction of Overgrowth of the gingival tissue makes it more difficult for i. Conditioned enlargement (pregnancy, puberty, vitamin the gingival overgrowth is still the most frequent treatment. Such treatment is only advocated when the overgrowth is severe. -

Orofacial Granulomatosis: a Review
DOI Number: 10.5958/0974-1283.2019.00181.6 Orofacial Granulomatosis: A Review Saloni Banga1, M K Sunil2, Hina Padaliya1 1Intern, 2Professor and Head of Department, Department of Oral Medicine & Radiology, Teerthanker Mahaveer Dental College & Research Center Moradabad Abstract Orofacial Granulomatosis (OFG) is an uncommon clinicopathological entity characterized clinically by the presence of persistent enlargement of the soft tissues of the oral and maxillofacial region and histologically by non-caseating and non-necrotizing granulomatous inflammation. The term ‘orofacial granulomatosis’ has been introduced to denote the group of various disorders, including Melkersson-Rosenthal syndrome and granulomatous cheilitis and has been noted to be associated with Crohn’s disease, Sarcoidosis and infectious diseases such as Tuberculosis. Although, various etiological agents such as dental materials, food additives and microbial agents have been recommended in the disease process. Treatment of orofacial granulomatosis is by corticosteroids but it’s not so efficient. It is more important to identify the pathogen first to specify the appropriate treatment line. Keywords— orofacial granulomatosis, Melkersson Rosenthal syndrome, crohn,s disease. Introduction Definition and its associated to other granulomatous disorders Orofacial granulomatosis term was introduced by Wiesenfeld in 19851. Granulomatosis is any condition Orofacial granulomatosis is an uncommon disorder1 characterized by the formation of multiple nodules or but is increasingly recognized. Orofacial granulomatosis granulomas in soft tissues. It encompasses Melkersson (as defined by Wiesenfeld in 1985) is the specific Rosenthal syndrome and Cheilitis granulomatosa1. histological finding of granulomas in mucosal or skin The true prevalence of this disease is unknown but is biopsies taken from the mouth or face in the absence suggested to be 0.8% (Mahler and Kiesewetter, 1996)3. -

Generalized Aggressive Periodontitis Associated with Plasma Cell Gingivitis Lesion: a Case Report and Non-Surgical Treatment
Clinical Advances in Periodontics; Copyright 2013 DOI: 10.1902/cap.2013.130050 Generalized Aggressive Periodontitis Associated With Plasma Cell Gingivitis Lesion: A Case Report and Non-Surgical Treatment * Andreas O. Parashis, Emmanouil Vardas, † Konstantinos Tosios, ‡ * Private practice limited to Periodontics, Athens, Greece; and, Department of Periodontology, School of Dental Medicine, Tufts University, Boston, MA, United States of America. †Clinic of Hospital Dentistry, Dental Oncology Unit, University of Athens, Greece. ‡ Private practice limited to Oral Pathology, Athens, Greece. Introduction: Plasma cell gingivitis (PCG) is an unusual inflammatory condition characterized by dense, band-like polyclonal plasmacytic infiltration of the lamina propria. Clinically, appears as gingival enlargement with erythema and swelling of the attached and free gingiva, and is not associated with any loss of attachment. The aim of this report is to present a rare case of severe generalized aggressive periodontitis (GAP) associated with a PCG lesion that was successfully treated and maintained non-surgically. Case presentation: A 32-year-old white male with a non-contributory medical history presented with gingival enlargement with diffuse erythema and edematous swelling, predominantly around teeth #5-8. Clinical and radiographic examination revealed generalized severe periodontal destruction. A complete blood count and biochemical tests were within normal limits. Histological and immunohistochemical examination were consistent with PCG. A diagnosis of severe GAP associated with a PCG lesion was assigned. Treatment included elimination of possible allergens and non- surgical periodontal treatment in combination with azithromycin. Clinical examination at re-evaluation revealed complete resolution of gingival enlargement, erythema and edema and localized residual probing depths 5 mm. One year post-treatment the clinical condition was stable. -

Periodontal Health, Gingival Diseases and Conditions 99 Section 1 Periodontal Health
CHAPTER Periodontal Health, Gingival Diseases 6 and Conditions Section 1 Periodontal Health 99 Section 2 Dental Plaque-Induced Gingival Conditions 101 Classification of Plaque-Induced Gingivitis and Modifying Factors Plaque-Induced Gingivitis Modifying Factors of Plaque-Induced Gingivitis Drug-Influenced Gingival Enlargements Section 3 Non–Plaque-Induced Gingival Diseases 111 Description of Selected Disease Disorders Description of Selected Inflammatory and Immune Conditions and Lesions Section 4 Focus on Patients 117 Clinical Patient Care Ethical Dilemma Clinical Application. Examination of the gingiva is part of every patient visit. In this context, a thorough clinical and radiographic assessment of the patient’s gingival tissues provides the dental practitioner with invaluable diagnostic information that is critical to determining the health status of the gingiva. The dental hygienist is often the first member of the dental team to be able to detect the early signs of periodontal disease. In 2017, the American Academy of Periodontology (AAP) and the European Federation of Periodontology (EFP) developed a new worldwide classification scheme for periodontal and peri-implant diseases and conditions. Included in the new classification scheme is the category called “periodontal health, gingival diseases/conditions.” Therefore, this chapter will first review the parameters that define periodontal health. Appreciating what constitutes as periodontal health serves as the basis for the dental provider to have a stronger understanding of the different categories of gingival diseases and conditions that are commonly encountered in clinical practice. Learning Objectives • Define periodontal health and be able to describe the clinical features that are consistent with signs of periodontal health. • List the two major subdivisions of gingival disease as established by the American Academy of Periodontology and the European Federation of Periodontology. -

Gingival Diseases in Children and Adolescents
8932 Indian Journal of Forensic Medicine & Toxicology, October-December 2020, Vol. 14, No. 4 Gingival Diseases in Children and Adolescents Sulagna Pradhan1, Sushant Mohanty2, Sonu Acharya3, Mrinali Shukla1, Sonali Bhuyan1 1Post Graduate Trainee, 2Professor & Head, 3Professor, Department of Paediatric and Preventive Dentistry, Institute of Dental Sciences, Siksha O Anusandhan (Deemed to be University), Bhubaneswar 751003, Odisha, India Abstract Gingival diseases are prevalent in both children and adolescents. These diseases may or may not be associated with plaques, maybe familial in some cases, or may coexist with systemic illness. However, gingiva and periodontium receive scant attention as the primary dentition does not last for a considerable duration. As gingival diseases result in the marked breakdown of periodontal tissue, and premature tooth loss affecting the nutrition and global development of a child/adolescent, precise identification and management of gingival diseases is of paramount importance. This article comprehensively discusses the nature, spectrum, and management of gingival diseases. Keywords: Gingival diseases; children and adolescents; spectrum, and management. Introduction reddish epithelium with mild keratinization may be misdiagnosed as inflammation. Lesser variability in the Children are more susceptible to several gingival width of the attached gingiva in the primary dentition diseases, paralleling to those observed in adults, though results in fewer mucogingival problems. The interdental vary in numerous aspects. Occasionally, natural variations papilla is broad buccolingual, and narrow mesiodistally. in the gingiva can masquerade as genuine pathology.1 The junctional epithelium associated with the deciduous On the contrary, a manifestation of a life-threatening dentition is thicker than the permanent dentition. underlying condition is misdiagnosed as normal gingiva. -

Cinnamon Products As a Possible Etiologic Factor in Orofacial Granulomatosis
Med Oral Patol Oral Cir Bucal. 2007 Oct 1;12(6):E440-4. Orofacial granulomatosis caused by cinnamon flavoring Med Oral Patol Oral Cir Bucal 2007;12:E440-4. Orofacial granulomatosis caused by cinnamon flavoring Cinnamon products as a possible etiologic factor in orofacial granulomatosis Hiroyasu Endo 1, Terry D. Rees 2 (1) Assistant Professor, Department of Periodontology, Nihon University, School of Dentistry at Matsudo, Japan (2) Professor and Former Chairman, Director of Stomatology, Department of Periodontics, Baylor College of Dentistry, Texas A&M University Health Science Center, Dallas, TX, USA Correspondence: Dr. Hiroyasu Endo Dept. of Periodontology Nihon University School of Dentistry at Matsudo 2-870-1 Sakaecho Nishi, Matsudo Chiba, Japan. 271-8587 E-mail: [email protected] Endo H, Rees TD. Cinnamon products as a possible etiologic factor Received: 17-09-2006 Accepted: 25-03-2007 in orofacial granulomatosis. Med Oral Patol Oral Cir Bucal. 2007 Oct 1;12(6):E440-4. © Medicina Oral S. L. C.I.F. B 96689336 - ISSN 1698-6946 Indexed in: -Index Medicus / MEDLINE / PubMed -EMBASE, Excerpta Medica -SCOPUS -Indice Médico Español -IBECS ABStract Objectives: It has been reported that clinical changes due to hypersensitivity reactions to various foods, preservatives, and oral hygiene products may be consistent with the characteristic signs of orofacial granulomatosis (OFG). The ob- jective of this study was to examine 37 well-documented cases of cinnamon-induced contact stomatitis for clinical and histological features consistent with a diagnosis of OFG. Study design: We reviewed the records of the 37 cases to screen them for the clinical and histopathologic features of OFG. -

A Concurrence of Periodontitis, Gingival Overgrowth and Plasma Cell Gingivitis: a Case Report
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 19, Issue 4 Ser.4 (April. 2020), PP 51-55 www.iosrjournals.org A Concurrence of Periodontitis, Gingival overgrowth and Plasma cell gingivitis: a case report Dr Yogesh Kumar Chanania1 Post Graduate Student, Dr C S Baiju2 MDS Professor & Head of Department, Dr Sumidha Bansal3 MDS Professor, Dr Karuna Joshi4 MDS Senior Lecturer 1(Department of Periodontics, Sudha Rustagi College of Dental Sciences & Research Faridabad, Pt. B. D. Sharma University of Health Sciences Rohtak, India) 2(Department of Periodontics, Sudha Rustagi College of Dental Sciences & Research Faridabad, Pt. B. D. Sharma University of Health Sciences Rohtak, India) 3(Department of Periodontics, Sudha Rustagi College of Dental Sciences & Research Faridabad, Pt. B. D. Sharma University of Health Sciences Rohtak, India) 4(Department of Periodontics, Sudha Rustagi College of Dental Sciences & Research Faridabad, Pt. B. D. Sharma University of Health Sciences Rohtak, India) Abstract: Periodontitis is inflammation of supporting tissues of the teeth, it causes destructive change that leads to loss of bone and periodontal ligament. Gingival overgrowth is increase in the size of gingiva. Gingival overgrowth may be associated with hormonal, nutritional imbalance or other local factors and systemic diseases. Plasma cell gingivitis is a condition that is clinically characterized by diffuse reddening and edematous swelling of gingiva. A non-smoker systemically healthy 35-year-old female patient reported with the chief complaint of swollen gums since 3 years. Clinically patient presented with generalized gingival overgrowth and was diagnosed as a stage IV grade ‘C’ periodontitis. -

Gingival Overgrowth As a Complication of Kidney Transplantation - Nepali Perspective
Nepalese Medical Journal, (2019) Vol. 2, 259 - 264 Review Article Gingival Overgrowth as a Complication of Kidney Transplantation - Nepali Perspective Swosti Thapa1, Robin Bahadur Basnet2, Bikal Shrestha3, Amresh Thakur4, Neesha Shrestha5, Anup Lal Shrestha6, Nabin Bahadur Basnet7 1Department of Burn, Plastic, and Reconstructive Surgery, Kirtipur Hospital, Kirtipur, Nepal 2Department of Urology, National Academy of Medical Sciences, Bir Hospital, Kathmandu, Nepal 3Department of Conservative and Endodontics, Nepal Police Hospital, Kathmandu, Nepal 4Department of Orthodontics and Dentofacial Orthopaedics, Nepal Armed Police Hospital, Kathmandu, Nepal 5Department of Dental Surgery, Kanti Children’s Hospital, Kathmandu, Nepal 6Orthodontics and Dentofacial Orthopaedics 7Department of Nephrology and Transplantation, Sumeru Hospital, Lalitpur, Nepal ABSTRACT Gingival Overgrowth is a known and common complication with multifactorial etiology Correspondence: seen in kidney transplant recipients. Gingival Overgrowth is induced in kidney transplant Dr. Nabin Bahadur Basnet, MBBS, PhD recipients by Cyclosporin A and Calcium Channel Blockers that are frequently prescribed to Department of Nephrology and Transplantation, them as immunosuppressive and antihypertensive, respectively. There have been 1477 kidney Sumeru Hospital, Lalitpur, Nepal ORCID ID: 0000-0002-3382-8176 transplantations in Nepal since the first kidney transplantation in 2008, but cases of gingival Email: [email protected] overgrowth have not been reported in any publications. The aim of this review is to discuss the different aspects of gingival overgrowth and its relevance to kidney transplant recipients of Nepal. Submitted : 1 5 th November 2019 This review will emphasize the need to examine the oral cavity of kidney transplant recipients. Accepted : 20th December 2019 Genetic predisposition, oral health, and offending drugs are involved in the pathogenesis of gingival overgrowth. -

Nonsurgical Management of Amlodipine
International Journal of Dental and Health Sciences Case Report Volume 02, Issue 05 SUBMANDIBULAR BACTERIAL SIALADENITIS: A CASE REPORT R. Pradeepalakshmi Ganesh1, Ramasamy2, Ravi David Austin3 1. Post Graduate student, Department of Oral Medicine and Radiology, Rajah Muthiah Dental College and Hospital, Annamalai University 2. Professor, Department of Oral Medicine and Radiology, Rajah Muthiah Dental college and Hospital, Annamalai University. 3. Professor & Head, Department of Oral Medicine and Radiology, Rajah Muthiah Dental college and Hospital, Annamalai University. ABSTRACT: Acute bacterial Sialadenitis, a painful and inflammatory infection preferentially affects parotid and submandibular gland. Though commonly caused by bacteria, the etiology ranges from simple infection to autoimmune disorders. Though it affects both parotid and submandibular gland, submandibular sialadenitis is an uncommon condition with an infrequent discussion in literature, unlike sialadenitis of the parotid gland. The management belies mainly on early administration of antimicrobial therapy and surgical drainage if deemed necessary. This case report describes a case of acute suppurative submandibular sialadenitis without a common predisposing factor, and its management. Key words: Submandibular gland, Bacterial sialadenitis, Suppurative sialadenitis, infection. INTRODUCTION: opening the mouth and pus exudation through duct orifice in suppurative A variety of factors affect the conditions. susceptibility of the salivary glands to bacterial infection, among them salivary CASE DETAIL: flow rate, composition of saliva and A 35 year old female patient reported to varying damage to their ductal systems the Department of Oral Medicine and are the most common predisposing Radiology, Rajah Muthiah Dental College, factors [1]. Deterioration of host defence Annamalai University, Chidambaram, inevitably renders the salivary glands Tamil Nadu with a complaint of painful susceptible to haematogenous infections.