Cinnamon Products As a Possible Etiologic Factor in Orofacial Granulomatosis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lumps and Swellings
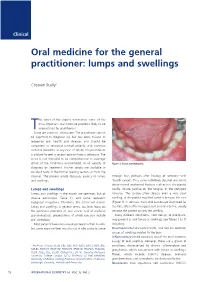
Clinical Oral medicine for the general practitioner: lumps and swellings Crispian Scully 1 his series of five papers summarises some of the most important oral medicine problems likely to be Tencountered by practitioners. Some are common, others rare. The practitioner cannot be expected to diagnose all, but has been trained to recognise oral health and disease, and should be competent to recognise normal variants, and common orofacial disorders. In any case of doubt, the practitioner is advised to seek a second opinion from a colleague. The series is not intended to be comprehensive in coverage either of the conditions encountered, or all aspects of Figure 1: Torus mandibularis. diagnosis or treatment: further details are available in standard texts, in the further reading section, or from the internet. The present article discusses aspects of lumps through fear, perhaps after hearing of someone with and swellings. ‘mouth cancer’. Thus some individuals discover and worry about normal anatomical features such as tori, the parotid Lumps and swellings papilla, foliate papillae on the tongue, or the pterygoid Lumps and swellings in the mouth are common, but of hamulus. The tongue often detects even a very small diverse aetiologies (Table 1), and some represent swelling, or the patient may first notice it because it is sore malignant neoplasms. Therefore, this article will discuss (Figure 1). In contrast, many oral cancers are diagnosed far lumps and swellings in general terms, but later focus on too late, often after being present several months, usually the particular problems of oral cancer and of orofacial because the patient ignores the swelling. -

Orofacial Granulomatosis
Al-Hamad, A; Porter, S; Fedele, S; (2015) Orofacial Granulomatosis. Dermatol Clin , 33 (3) pp. 433- 446. 10.1016/j.det.2015.03.008. Downloaded from UCL Discovery: http://discovery.ucl.ac.uk/1470143 ARTICLE Oro-facial Granulomatosis Arwa Al-Hamad1, 2, Stephen Porter1, Stefano Fedele1, 3 1 University College London, UCL Eastman Dental Institute, Oral Medicine Unit, 256 Gray’s Inn Road, WC1X 8LD, London UK. 2 Dental Services, King Abdulaziz Medical City-Riyadh, Ministry of National Guard, Riyadh, Saudi Arabia. 3 NIHR University College London Hospitals Biomedical Research Centre, London, UK. Acknowledgments: Part of this work was undertaken at University College London/University College London Hospital, which received a proportion of funding from the Department of Health’s National Institute for Health Research Biomedical Research Centre funding scheme. Conflicts of Interest: The authors declare that they have no affiliation with any organization with a financial interest, direct or indirect, in the subject matter or materials discussed in the manuscript that may affect the conduct or reporting of the work submitted. Authorship: all authors named above meet the following criteria of the International Committee of Medical Journal Editors: 1) Substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; 2) Drafting the article or revising it critically for important intellectual content; 3) Final approval of the version to be published. Corresponding author: Dr. Stefano Fedele DDS, PhD -

Orofacial Granulomatosis Presenting As Gingival Enlargement – Report of Three Cases
Open Access Journal of Dentistry & Oral Disorders Case Report Orofacial Granulomatosis Presenting as Gingival Enlargement – Report of Three Cases Savithri V*, Janardhanan M, Suresh R and Aravind T Abstract Department of Oral Pathology & Microbiology, Amrita Orofacial Granulomatosis (OFG) is an uncommon disease characterized School of Dentistry, Amrita VishwaVidyapeetham, Amrita by non-caseating granulomatous inflammation in the oral and maxillofacial University, India region. They present clinically as labial enlargement, perioral and/or mucosal *Corresponding author: Vindhya Savithri, swelling, angular cheilitis, mucosal tags, vertical fissures of lips, lingua plicata, Department of Oral Pathology & Microbiology, Amrita oral ulcerations and gingival enlargement. The term OFG was introduced by School of Dentistry, Amrita VishwaVidyapeetham, Amrita Wiesenfeld in 1985. The diagnosis of OFG is done by the clinical presentation University, India and histological picture and this may be further complicated by the fact that OFG may be the oral manifestation of a systemic condition, such as Crohn’s Received: October 16, 2017; Accepted: November 27, disease, sarcoidosis, or, more rarely, Wegener’s granulomatosis. In addition, 2017; Published: December 04, 2017 several conditions, including tuberculosis, leprosy, systemic fungal infections, and foreign body reactions may show granulomatous inflammation on histologic examination. They have to be excluded out by appropriate investigations. They have to be excluded out by appropriate investigations. -

Orofacial Granulomatosis: a Review
DOI Number: 10.5958/0974-1283.2019.00181.6 Orofacial Granulomatosis: A Review Saloni Banga1, M K Sunil2, Hina Padaliya1 1Intern, 2Professor and Head of Department, Department of Oral Medicine & Radiology, Teerthanker Mahaveer Dental College & Research Center Moradabad Abstract Orofacial Granulomatosis (OFG) is an uncommon clinicopathological entity characterized clinically by the presence of persistent enlargement of the soft tissues of the oral and maxillofacial region and histologically by non-caseating and non-necrotizing granulomatous inflammation. The term ‘orofacial granulomatosis’ has been introduced to denote the group of various disorders, including Melkersson-Rosenthal syndrome and granulomatous cheilitis and has been noted to be associated with Crohn’s disease, Sarcoidosis and infectious diseases such as Tuberculosis. Although, various etiological agents such as dental materials, food additives and microbial agents have been recommended in the disease process. Treatment of orofacial granulomatosis is by corticosteroids but it’s not so efficient. It is more important to identify the pathogen first to specify the appropriate treatment line. Keywords— orofacial granulomatosis, Melkersson Rosenthal syndrome, crohn,s disease. Introduction Definition and its associated to other granulomatous disorders Orofacial granulomatosis term was introduced by Wiesenfeld in 19851. Granulomatosis is any condition Orofacial granulomatosis is an uncommon disorder1 characterized by the formation of multiple nodules or but is increasingly recognized. Orofacial granulomatosis granulomas in soft tissues. It encompasses Melkersson (as defined by Wiesenfeld in 1985) is the specific Rosenthal syndrome and Cheilitis granulomatosa1. histological finding of granulomas in mucosal or skin The true prevalence of this disease is unknown but is biopsies taken from the mouth or face in the absence suggested to be 0.8% (Mahler and Kiesewetter, 1996)3. -

Oral and Maxillo-Facial Manifestations of Systemic Diseases: an Overview
medicina Review Oral and Maxillo-Facial Manifestations of Systemic Diseases: An Overview Saverio Capodiferro *,† , Luisa Limongelli *,† and Gianfranco Favia Department of Interdisciplinary Medicine, University of Bari Aldo Moro, Piazza G. Cesare, 11, 70124 Bari, Italy; [email protected] * Correspondence: [email protected] (S.C.); [email protected] (L.L.) † These authors contributed equally to the paper. Abstract: Many systemic (infective, genetic, autoimmune, neoplastic) diseases may involve the oral cavity and, more generally, the soft and hard tissues of the head and neck as primary or secondary localization. Primary onset in the oral cavity of both pediatric and adult diseases usually represents a true challenge for clinicians; their precocious detection is often difficult and requires a wide knowledge but surely results in the early diagnosis and therapy onset with an overall better prognosis and clinical outcomes. In the current paper, as for the topic of the current Special Issue, the authors present an overview on the most frequent clinical manifestations at the oral and maxillo-facial district of systemic disease. Keywords: oral cavity; head and neck; systemic disease; oral signs of systemic diseases; early diagnosis; differential diagnosis Citation: Capodiferro, S.; Limongelli, 1. Introduction L.; Favia, G. Oral and Maxillo-Facial Oral and maxillo-facial manifestations of systemic diseases represent an extensive and Manifestations of Systemic Diseases: fascinating study, which is mainly based on the knowledge that many signs and symptoms An Overview. Medicina 2021, 57, 271. as numerous systemic disorders may first present as or may be identified by head and https://doi.org/10.3390/ neck tissue changes. -

Orofacial Granulomatosis
Division of Oral Medicine and Dentistry Orofacial Granulomatosis What is orofacial granulomatosis? How do we know it is OFG? Orofacial granulomatosis (OFG) is an uncommon condition of A dental specialist can usually diagnose OFG based on a good the mouth that causes lip swelling, and sometimes swelling of history, a thorough clinical examination, and a biopsy to the face, inner cheeks, and the gums. Tis swelling may come confrm the diagnosis. You may be sent to a specialist who can and go at frst, but over time, becomes persistent if not treated. perform a patch test of your skin to see if you are sensitive to Patients will typically describe their symptoms as swelling and foods, food preservatives or other substances. Te results of the tightness and sometimes, soreness. In addition, there may be patch test may help your doctor to suggest the best treatment some folding of the inside of the mouth giving it a “cobblestone” option for your disease. Patients may be referred to appearance. OFG may be part of Melkersson-Rosenthal a gastrointestinal specialist if a diagnosis of Crohn disease syndrome, a rare condition that consists of OFG, fssured is suspected. tongue (tongue with deep grooves) and paralysis of the face. How do we treat OFG? What causes OFG? A food diary can be helpful if food sensitivity is suspected or It is likely that patients with OFG are reacting to something confrmed by patch testing, and completely avoiding such foods although this is not always easy to identify. Some common may substantially reduce swelling. Te doctor who patch tested triggers are foods and food preservatives such as chocolate, you will provide you with a list of substances to avoid if you cinnamon favorings, and preservatives such as benzoates and patch tested positive to them. -

Oral Leukoplakia Associated with Amalgam Restorations Zeynep B
445 Journal of Oral Science, Vol. 58, No. 3, 445-448, 2016 Case Report Oral leukoplakia associated with amalgam restorations Zeynep B. Gönen1,2), Canay Yılmaz Asan1), Osman Etöz1), and Alper Alkan1) 1)Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Erciyes University, Kayseri, Turkey 2)Genome and Stem Cell Center, Erciyes University, Kayseri, Turkey (Received January 27, 2016; Accepted March 18, 2016) Abstract: The World Health Organization has The etiological factors most commonly associated defined oral leukoplakia (OL) as “a white patch or with OL have been smoking, alcohol abuse, candidiasis, plaque of the oral mucosa that cannot be character- HPV infection, iron deficiency, and low serum levels of ized clinically or pathologically as any other disease”. vitamin A and beta-carotene (3). Zinsser-Cole Engman A 21-year-old male with OL presented with a bilateral syndrome, a genodermatosis commonly known as burning sensation in the buccal mucosa. The patient dyskeratosis congenita, includes oral manifestations such had amalgam restorations, and an epicutaneous as OL. Many different non-surgical and surgical modali- patch test indicated a positive response to amalgam. ties such as conventional surgery, electrocauterization, The amalgam restorations were therefore removed laser ablation, cryosurgery, and medications such as and the cavities were refilled with a composite resin vitamin A, vitamin B, and bleomycin, have been reported restorative material. During 5 years of follow-up, for treatment of OL (4). there was no recurrence of the oral lesions. This case Dental amalgams remain the most commonly used illustrates that amalgam fillings may cause OL lesions. posterior restorative material in dental practice. -

Oral Pathology Final Exam Review Table Tuanh Le & Enoch Ng, DDS
Oral Pathology Final Exam Review Table TuAnh Le & Enoch Ng, DDS 2014 Bump under tongue: cementoblastoma (50% 1st molar) Ranula (remove lesion and feeding gland) dermoid cyst (neoplasm from 3 germ layers) (surgical removal) cystic teratoma, cyst of blandin nuhn (surgical removal down to muscle, recurrence likely) Multilocular radiolucency: mucoepidermoid carcinoma cherubism ameloblastoma Bump anterior of palate: KOT minor salivary gland tumor odontogenic myxoma nasopalatine duct cyst (surgical removal, rare recurrence) torus palatinus Mixed radiolucencies: 4 P’s (excise for biopsy; curette vigorously!) calcifying odontogenic (Gorlin) cyst o Pyogenic granuloma (vascular; granulation tissue) periapical cemento-osseous dysplasia (nothing) o Peripheral giant cell granuloma (purple-blue lesions) florid cemento-osseous dysplasia (nothing) o Peripheral ossifying fibroma (bone, cartilage/ ossifying material) focal cemento-osseous dysplasia (biopsy then do nothing) o Peripheral fibroma (fibrous ct) Kertocystic Odontogenic Tumor (KOT): unique histology of cyst lining! (see histo notes below); 3 important things: (1) high Multiple bumps on skin: recurrence rate (2) highly aggressive (3) related to Gorlin syndrome Nevoid basal cell carcinoma (Gorlin syndrome) Hyperparathyroidism: excess PTH found via lab test Neurofibromatosis (see notes below) (refer to derm MD, tell family members) mucoepidermoid carcinoma (mixture of mucus-producing and squamous epidermoid cells; most common minor salivary Nevus gland tumor) (get it out!) -

A Rare Case of Orofacial Granulomatosis
A Rare Case of Orofacial Granulomatosis Dennis Keselman BA, David Swender D.O., Leah Chernin D.O., Robert Hostoffer D.O. and Haig Tcheurekdjian M.D. University Hospitals Richmond Medical Center Allergy/Immunology Fellowship, Cleveland, OH ABSTRACT CASE REPORT RESULTS SUMMARY DISCUSSION Introduction: Orofacial Granulomatosis(OFG) is a rarely occurring disease with greater propensity for Our patient is a 49y/o African American female with history of hypertension, DMII, glaucoma and asthma presented OFG is a rare but serious condition and must be a differential diagnosis in all patients presenting with chronic labial females which presents with swelling of the maxillofacial and oral tissue worsening overtime. It is often with paraoral and inner oral swelling over the past 10 years with recent worsening over the past 2-3 years. The patient • C1 esterase inhibitor and C4 were in normal limits to rule out possible hereditary angioedema. swelling. Do to the rarity of the condition as well as the sparse data available it may be overlooked by many considered as part of a spectrum of diseases including the more severe process, Chellitis Granulomatosa smokes half a pack of cigarettes daily. The swelling initially began with recurrent episodes which would last 1-2 days physicians (Johani, Moles, Hodgson, Porter, & Fedele, 2009). In our patient the definitive diagnosis took 10 years (CG) which may be a sign of Melkersson-Rosenthal Syndrome (MRS) which includes facial paralysis along and then resolve spontaneously. However over time the disease has evolved to the point of where her lip is always • Patient had an instance of elevated Anti-SM antibodies in 2006 with no other markers of autoimmune and in many a delay such as this may lead to debilitating problems with airway, eating or communication. -

Approach to Orofacial Granulomatosis and Review of Literature
Original Article Approach to orofacial granulomatosis and review of literature A. Javadzadeh 1, A. Pakfetrat 1, F. Falaki 2, S.A. Seyyedi 3 1 Associate Professor, Department of Oral Medicine, School of Dentistry, Mashhad University of Medical Sciences. Mashhad, Iran. 2 Assistant Professor, Department of Oral Medicine, School of Dentistry, Mashhad University of Medical Sciences. Mashhad, Iran. 3 Assistant Professor, Department of Oral Medicine, School of Dentistry, Urmia University of Medical Sciences. Urmia, Iran. Abstract Background and Aim: Orofacial granulomatosis (OFG) comprises a group of diseas- es characterized by non-caseating granulomatous inflammation affecting the soft tis- sues of the oral and maxillofacial region. Wiesenfeld introduced the term orofacial granulomatosis in 1985 for the first time. The precise cause of OFG is unknown; however, some theories have been suggested in- cluding allergy, infection and genetic predisposition. The clinical presentation can be highly variable, making the diagnosis difficult to es- tablish. The aim of this review was to define clinical features, differential diagnosis and treat- ment protocols of OFG. Materials and Methods: All English articles from 1950 to 2010 in Pubmed, InterS- cience, ScienceDirect, Google Scholar databases were searched using the keywords: orofacial granulomatosis, approach, and treatment. Persian articles were also selected from Iran Medex. Results and Conclusion: Because of the relatively nonspecific clinical findings asso- ciated with a variety of granulomatous diseases, the diagnosis of orofacial granulomat- ous often presents a dilemma for the clinician. The most common differential diagno- Corresponding author: sis includes Crohn's disease, sarcoidosis, and infection. However, a variety of other Dr. Seyyedi S.A., Associate conditions may be associated with granuloma formation. -

Intralesional Corticosteroid Injection As an Effective Treatment Method for Oral Lesions: a Meta-Analysis
Brazilian Journal of Pharmaceutical Sciences Review http://dx.doi.org/10.1590/s2175-97902019000418077 Intralesional corticosteroid injection as an effective treatment method for oral lesions: a meta-analysis Narges Gholizadeh1, Maryam-Sadat Sadrzadeh-Afshar 2, Nafiseh Sheykhbahaei3* 1Oral & Maxillofacial Medicine Department, School of Dentistry, Tehran University of Medical Sciences, Tehran, Iran, 2Oral & Maxillofacial Medicine Department, School of Dentistry, Aja University of Medical Sciences, Tehran, Iran, 3Oral & Maxillofacial Medicine Department, School of Dentistry, Tehran University of Medical Sciences, Tehran, Iran Intralesional corticosteroid injection (ICSI) is known as one of the main methods used for treating a wide range of lesions. It also results in a high concentration of drugs at lesion sites, with minimal systemic absorption. Thus, this study aimed to provide a review of the intralesional corticosteroid injection (ICSI) indications in the treatment of oral lesions. To this end; relevant key words were searched in the databases of PubMed, Google Scholar, Scopus, ScienceDirect, and UpToDate in the present study. Accordingly, the results of a total number of 62 case reports or case series articles were used in this study and the positive therapeutic effects of intralesional corticosteroid injection (ICSI) in 23 common oral lesions were reported. The most common type of intralesional steroid in the treatment of oral lesions was triamcinolone. No significant difference was also observed in terms of pain in patients following the use of steroid alone or in combination with anesthetic agents; moreover, the reported side effects of this method were exceptionally rare and transient. It was concluded that the intralesional corticosteroid injection (ICSI) could be one of the effective therapeutic methods with no significant problems in many oral lesions such as inflammatory, immunologic, and vascular ones due to its higher therapeutic effects than other topical forms of steroids and fewer side effects than systemic corticosteroid. -

Orofacial Granulomatosis and Oral Symptoms in a South Australian
OROFACIAL GRANULOMATOSIS AND ORAL SYMPTOMS IN A SOUTH AUSTRALIAN PAEDIATRIC POPULATION WITH CROHN’S DISEASE DOCTOR OF CLINICAL DENTISTRY (Paediatric Dentistry) By Evelyn Kar-Yun Yeung B.D.S (Adelaide) Department of Paediatric Dentistry School of Dentistry Faculty of Health Sciences The University of Adelaide South Australia August 2012 Preface Thesis Declaration This work contains no material which has been accepted for the award of any other degree or diploma in any university or other tertiary institution and, to the best of my knowledge and belief, contains no material previously published or written by another person, except where due reference has been made in the text. I give consent to this copy of my thesis, when deposited in the University Library, being made available for loan and photocopying, subject to the provisions of the Copyright Act 1968. I also give permission for the digital version of my thesis to be made available on the web, via the University’s digital research repository, the Library catalogue, the Australasian Digital Theses Program (ADTP) and also through web search engines, unless permission has been granted by the University to restrict access for a period of time. Evelyn Kar-Yun Yeung August 2012 ii Preface Table of Contents Thesis Declaration .......................................................................................................................... ii Table of Contents ..........................................................................................................................