Gingival Manifestations of Orofacial Granulomatosis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lumps and Swellings
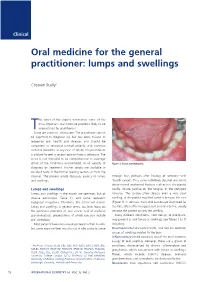
Clinical Oral medicine for the general practitioner: lumps and swellings Crispian Scully 1 his series of five papers summarises some of the most important oral medicine problems likely to be Tencountered by practitioners. Some are common, others rare. The practitioner cannot be expected to diagnose all, but has been trained to recognise oral health and disease, and should be competent to recognise normal variants, and common orofacial disorders. In any case of doubt, the practitioner is advised to seek a second opinion from a colleague. The series is not intended to be comprehensive in coverage either of the conditions encountered, or all aspects of Figure 1: Torus mandibularis. diagnosis or treatment: further details are available in standard texts, in the further reading section, or from the internet. The present article discusses aspects of lumps through fear, perhaps after hearing of someone with and swellings. ‘mouth cancer’. Thus some individuals discover and worry about normal anatomical features such as tori, the parotid Lumps and swellings papilla, foliate papillae on the tongue, or the pterygoid Lumps and swellings in the mouth are common, but of hamulus. The tongue often detects even a very small diverse aetiologies (Table 1), and some represent swelling, or the patient may first notice it because it is sore malignant neoplasms. Therefore, this article will discuss (Figure 1). In contrast, many oral cancers are diagnosed far lumps and swellings in general terms, but later focus on too late, often after being present several months, usually the particular problems of oral cancer and of orofacial because the patient ignores the swelling. -

Oral Lesions in Sjögren's Syndrome
Med Oral Patol Oral Cir Bucal. 2018 Jul 1;23 (4):e391-400. Oral lesions in Sjögren’s syndrome patients Journal section: Oral Medicine and Pathology doi:10.4317/medoral.22286 Publication Types: Review http://dx.doi.org/doi:10.4317/medoral.22286 Oral lesions in Sjögren’s syndrome: A systematic review Julia Serrano 1, Rosa-María López-Pintor 1, José González-Serrano 1, Mónica Fernández-Castro 2, Elisabeth Casañas 1, Gonzalo Hernández 1 1 Department of Oral Medicine and Surgery, School of Dentistry, Complutense University, Madrid, Spain 2 Rheumatology Service, Hospital Infanta Sofía, Madrid, Spain Correspondence: Departamento de Especialidades Clínicas Odontológicas Facultad de Odontología Universidad Complutense de Madrid Plaza Ramón y Cajal s/n, 28040 Madrid. Spain [email protected] Serrano J, López-Pintor RM, González-Serrano J, Fernández-Castro M, Casañas E, Hernández G. Oral lesions in Sjögren’s syndrome: A system- atic review. Med Oral Patol Oral Cir Bucal. 2018 Jul 1;23 (4):e391-400. Received: 18/11/2017 http://www.medicinaoral.com/medoralfree01/v23i4/medoralv23i4p391.pdf Accepted: 09/05/2018 Article Number: 22291 http://www.medicinaoral.com/ © Medicina Oral S. L. C.I.F. B 96689336 - pISSN 1698-4447 - eISSN: 1698-6946 eMail: [email protected] Indexed in: Science Citation Index Expanded Journal Citation Reports Index Medicus, MEDLINE, PubMed Scopus, Embase and Emcare Indice Médico Español Abstract Background: Sjögren’s syndrome (SS) is an autoimmune disease related to two common symptoms: dry mouth and eyes. Although, xerostomia and hyposialia have been frequently reported in these patients, not many studies have evaluated other oral manifestations. -
Benign Migratory Glossitis: Case Report and Literature Review
Volume 1- Issue 5 : 2017 DOI: 10.26717/BJSTR.2017.01.000482 Sarfaraz Khan. Biomed J Sci & Tech Res ISSN: 2574-1241 Case Report Open Access Benign Migratory Glossitis: Case Report and Literature Review Sarfaraz Khan1*, Syed AsifHaider Shah2, Tanveer Ahmed Mujahid3 and Muhammad Ishaq4 1Consultant Oral and Maxillofacial Surgeon, Pak Field Hospital Darfur, Sudan 2MDC Gujranwala, Pakistan 3Consultant Dermatologist, Pak Field Hospital Darfur, Sudan 4Registrar Dermatologist, Pak Field Hospital Darfur, Sudan Received: October 25, 2017; Published: October 31, 2017 *Corresponding author: Sarfaraz Khan, Consultant Oral and Maxillofacial Surgeon, Pakistan Field Hospital Darfur, Sudan, Tel: ; Email: Abstract Benign migratory Glossitis (BMG) is a benign, usually asymptomatic mucosal lesion of dorsal surface of the tongue, characterized by depapillated erythematous patches separated by white irregular borders. Etiology of BMG is unknown. Risk factors include psoriasis, fissured tongue, diabetes mellitus, hypersensitivity and psychological factors. We report BMG in an Egyptian soldier of UN peace keeping force, with stressKeywords: as a possible Geographic etiological tongue; factor Benign and migratory provide literature Glossitis; reviewErythema of this migrans disorder. Introduction Benign migratory Glossitis (BMG) is a benign, immune- spicy/salty food and/or alcoholic drinks [4,5].The lesion typically usually characterized by asymptomatic erythematous patches changes its shape with time owing to the change in pattern of mediated, chronic inflammatory lesion of unknown etiology, depapillation.Similar lesions may also be seen in atrophic candidiasis, local chemical or mechanical trauma, drug induced reactions, psoriasis with whitish margins across the surface of the tongue. This condition is also known as geographic tongue, erythema migrans, Treatment of symptomatic BMG aims at provision of symptomatic Glossitis exfoliativa and wandering rash of the tongue. -

Review: Differential Diagnosis of Drug-Induced Gingival Hyperplasia and Other Oral Lesions
ISSN: 2469-5734 Moshe. Int J Oral Dent Health 2020, 6:108 DOI: 10.23937/2469-5734/1510108 Volume 6 | Issue 2 International Journal of Open Access Oral and Dental Health REVIEW ARTICLE Review: Differential Diagnosis of Drug-Induced Gingival Hyper- plasia and Other Oral Lesions Einhorn Omer Moshe* Private Dental Office, Israel Check for *Corresponding author: Einhorn Omer Moshe, Private Dental Office, Dr. Einhorn, 89 Medinat Hayehudim updates street, Herzliya, Israel tooth discoloration, alteration of taste sensation and Abstract even appearance of lesions on the tissues of the oral Chronic medication usage is a major component of the cavity. Early recognition and diagnosis of these effects medical diagnosis of patients. Nowadays, some of the most common diseases such as cancer, hypertension, diabetes can largely assist in the prevention of further destruc- and etc., are treated with drugs which cause a variety of oral tive consequences in patients’ health status. As life ex- side-effects including gingival over growth and appearance pectancy increases, the number of elderly patients in of lesions on the tissues of the oral cavity. As such, drug-in- the dental practice also rises. Individuals of this popula- duced oral reactions are an ordinary sight in the dental prac- tice. This review will point out the main therapeutic agents tion are usually subjected to chronic medication intake causing gingival hyperplasia and other pathologic lesions which requires the clinician to be aware of the various in the oral cavity. Some frequently used medications, in side-effects accompanying these medications. This re- particular antihypertensives, nonsteroidal anti-inflammatory view will point out the main therapeutic agents causing drugs and even antibiotics, can lead to overgrowth of the gingival hyperplasia and other pathologic lesions in the gingiva and to the multiple unwanted conditions, namely: Lupus erythematosus, erythema multiforme, mucositis, oral oral cavity. -

Case Report Treatment of Geographic Tongue
Scholars Journal of Dental Sciences (SJDS) ISSN 2394-496X (Online) Sch. J. Dent. Sci., 2015; 2(7):409-413 ISSN 2394-4951 (Print) ©Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources) www.saspublisher.com Case Report Treatment of Geographic Tongue Superimposing Fissured Tongue: A literature review with case report Jalaleddin H Hamissi1, Mahsa EsFehani2, Zahra Hamissi3 1Associate Professor in periodontics and Dental Caries Prevention Research Center, Qazvin University Medical Sciences, Qazvin, Iran. 2Assistant Professor, Department of Oral Medicine & Diagnosis, college dentistry, Qazvin University Medical Sciences, Qazvin, Iran. 3Dental Student, College of Dentistry, Shahied Behesti University of Medical Sciences, Teheran, Iran *Corresponding author Dr Jalaleddin H Hamissi Email: [email protected] ; [email protected] Abstract: Tongue is a most sensitive part of the oral cavity. It is responsible for many functions in the mouth like swallowing, speech, mastication, speaking and breathing. Geographic tongue (Benign migratory glossitis, erythema migrans) is an asymptomatic inflammatory disorder of tongue with controversial etiology. This disease is characterized by erythematous areas showing raised greyish or white circinate lines or bands with irregular pattern on the dorsal surface of the tongue and depapillation. The objective in presenting the case report and literature review is to discuss the clinical presentation, associated causative factors and management strategies of geographic tongue. Keywords: Asymptomatic; Characteristics; Fissured tongue; Geographic tongue; Migratory INTRODUCTION in approximately three percent (3%) majority of female Geographic tongue is an asymptomatic population [9]. On other aspects of oral mucosa, such as inflammatory condition of the dorsum of tongue on commissure of lip, floor of mouth, cheek etc., which occasionally extending towards the lateral borders. -

Orofacial Granulomatosis
Al-Hamad, A; Porter, S; Fedele, S; (2015) Orofacial Granulomatosis. Dermatol Clin , 33 (3) pp. 433- 446. 10.1016/j.det.2015.03.008. Downloaded from UCL Discovery: http://discovery.ucl.ac.uk/1470143 ARTICLE Oro-facial Granulomatosis Arwa Al-Hamad1, 2, Stephen Porter1, Stefano Fedele1, 3 1 University College London, UCL Eastman Dental Institute, Oral Medicine Unit, 256 Gray’s Inn Road, WC1X 8LD, London UK. 2 Dental Services, King Abdulaziz Medical City-Riyadh, Ministry of National Guard, Riyadh, Saudi Arabia. 3 NIHR University College London Hospitals Biomedical Research Centre, London, UK. Acknowledgments: Part of this work was undertaken at University College London/University College London Hospital, which received a proportion of funding from the Department of Health’s National Institute for Health Research Biomedical Research Centre funding scheme. Conflicts of Interest: The authors declare that they have no affiliation with any organization with a financial interest, direct or indirect, in the subject matter or materials discussed in the manuscript that may affect the conduct or reporting of the work submitted. Authorship: all authors named above meet the following criteria of the International Committee of Medical Journal Editors: 1) Substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; 2) Drafting the article or revising it critically for important intellectual content; 3) Final approval of the version to be published. Corresponding author: Dr. Stefano Fedele DDS, PhD -

Orofacial Granulomatosis Presenting As Gingival Enlargement – Report of Three Cases
Open Access Journal of Dentistry & Oral Disorders Case Report Orofacial Granulomatosis Presenting as Gingival Enlargement – Report of Three Cases Savithri V*, Janardhanan M, Suresh R and Aravind T Abstract Department of Oral Pathology & Microbiology, Amrita Orofacial Granulomatosis (OFG) is an uncommon disease characterized School of Dentistry, Amrita VishwaVidyapeetham, Amrita by non-caseating granulomatous inflammation in the oral and maxillofacial University, India region. They present clinically as labial enlargement, perioral and/or mucosal *Corresponding author: Vindhya Savithri, swelling, angular cheilitis, mucosal tags, vertical fissures of lips, lingua plicata, Department of Oral Pathology & Microbiology, Amrita oral ulcerations and gingival enlargement. The term OFG was introduced by School of Dentistry, Amrita VishwaVidyapeetham, Amrita Wiesenfeld in 1985. The diagnosis of OFG is done by the clinical presentation University, India and histological picture and this may be further complicated by the fact that OFG may be the oral manifestation of a systemic condition, such as Crohn’s Received: October 16, 2017; Accepted: November 27, disease, sarcoidosis, or, more rarely, Wegener’s granulomatosis. In addition, 2017; Published: December 04, 2017 several conditions, including tuberculosis, leprosy, systemic fungal infections, and foreign body reactions may show granulomatous inflammation on histologic examination. They have to be excluded out by appropriate investigations. They have to be excluded out by appropriate investigations. -

Chronic Inflammatory Gingival Enlargement and Treatment: a Case Report
Case Report Adv Dent & Oral Health Volume 9 Issue 4- July 2018 Copyright © All rights are reserved by Mehmet Özgöz DOI: 10.19080/ADOH.2018.09.555766 Chronic Inflammatory Gingival Enlargement and Treatment: A Case Report Mehmet Özgöz1* and Taner Arabaci2 1Department of Periodontology, Akdeniz University, Turkey 2Department of Periodontology, Atatürk University, Turkey Submission: June 14, 2018; Published: July 18, 2018 *Corresponding author: Özgöz, Department of Periodontology, Akdeniz University Faculty of Dentistry, Antalya, Turkey, Fax:+902423106967; Email: Abstract Gingival enlargement is a common feature in gingival disease. If gingival enlargement isn’t treated, it may some aesthetic problems, plaque accumulation,Keywords: Gingival gingival enlargement; bleeding, and Periodontal periodontitis. treatments; In this paper, Etiological inflammatory factors; Plasma gingival cell enlargement gingivitis and treatment was presented. Introduction and retention include poor oral hygiene, abnormal relationship of Gingival enlargement is a common feature in gingival disease adjacent teeth, lack of tooth function, cervical cavities, improperly contoured dental restorations, food impaction, nasal obstruction, connection with etiological factors and pathological changes [3-5]. [1,2]. Many types of gingival enlargement can be classified in orthodontic therapy involving repositioning of the teeth, and habits such as mouth breathing and pressing the tongue against the gingival [18-20]. a)b) InflammatoryDrug-induced enlargement:enlargement [7-12]. chronic and acute [6]. c) Gingival enlargements associated with systemic diseases: patients to maintain oral hygiene [9,21]. Surgical correction of Overgrowth of the gingival tissue makes it more difficult for i. Conditioned enlargement (pregnancy, puberty, vitamin the gingival overgrowth is still the most frequent treatment. Such treatment is only advocated when the overgrowth is severe. -

Orofacial Granulomatosis: a Review
DOI Number: 10.5958/0974-1283.2019.00181.6 Orofacial Granulomatosis: A Review Saloni Banga1, M K Sunil2, Hina Padaliya1 1Intern, 2Professor and Head of Department, Department of Oral Medicine & Radiology, Teerthanker Mahaveer Dental College & Research Center Moradabad Abstract Orofacial Granulomatosis (OFG) is an uncommon clinicopathological entity characterized clinically by the presence of persistent enlargement of the soft tissues of the oral and maxillofacial region and histologically by non-caseating and non-necrotizing granulomatous inflammation. The term ‘orofacial granulomatosis’ has been introduced to denote the group of various disorders, including Melkersson-Rosenthal syndrome and granulomatous cheilitis and has been noted to be associated with Crohn’s disease, Sarcoidosis and infectious diseases such as Tuberculosis. Although, various etiological agents such as dental materials, food additives and microbial agents have been recommended in the disease process. Treatment of orofacial granulomatosis is by corticosteroids but it’s not so efficient. It is more important to identify the pathogen first to specify the appropriate treatment line. Keywords— orofacial granulomatosis, Melkersson Rosenthal syndrome, crohn,s disease. Introduction Definition and its associated to other granulomatous disorders Orofacial granulomatosis term was introduced by Wiesenfeld in 19851. Granulomatosis is any condition Orofacial granulomatosis is an uncommon disorder1 characterized by the formation of multiple nodules or but is increasingly recognized. Orofacial granulomatosis granulomas in soft tissues. It encompasses Melkersson (as defined by Wiesenfeld in 1985) is the specific Rosenthal syndrome and Cheilitis granulomatosa1. histological finding of granulomas in mucosal or skin The true prevalence of this disease is unknown but is biopsies taken from the mouth or face in the absence suggested to be 0.8% (Mahler and Kiesewetter, 1996)3. -

Generalized Aggressive Periodontitis Associated with Plasma Cell Gingivitis Lesion: a Case Report and Non-Surgical Treatment
Clinical Advances in Periodontics; Copyright 2013 DOI: 10.1902/cap.2013.130050 Generalized Aggressive Periodontitis Associated With Plasma Cell Gingivitis Lesion: A Case Report and Non-Surgical Treatment * Andreas O. Parashis, Emmanouil Vardas, † Konstantinos Tosios, ‡ * Private practice limited to Periodontics, Athens, Greece; and, Department of Periodontology, School of Dental Medicine, Tufts University, Boston, MA, United States of America. †Clinic of Hospital Dentistry, Dental Oncology Unit, University of Athens, Greece. ‡ Private practice limited to Oral Pathology, Athens, Greece. Introduction: Plasma cell gingivitis (PCG) is an unusual inflammatory condition characterized by dense, band-like polyclonal plasmacytic infiltration of the lamina propria. Clinically, appears as gingival enlargement with erythema and swelling of the attached and free gingiva, and is not associated with any loss of attachment. The aim of this report is to present a rare case of severe generalized aggressive periodontitis (GAP) associated with a PCG lesion that was successfully treated and maintained non-surgically. Case presentation: A 32-year-old white male with a non-contributory medical history presented with gingival enlargement with diffuse erythema and edematous swelling, predominantly around teeth #5-8. Clinical and radiographic examination revealed generalized severe periodontal destruction. A complete blood count and biochemical tests were within normal limits. Histological and immunohistochemical examination were consistent with PCG. A diagnosis of severe GAP associated with a PCG lesion was assigned. Treatment included elimination of possible allergens and non- surgical periodontal treatment in combination with azithromycin. Clinical examination at re-evaluation revealed complete resolution of gingival enlargement, erythema and edema and localized residual probing depths 5 mm. One year post-treatment the clinical condition was stable. -

Periodontal Health, Gingival Diseases and Conditions 99 Section 1 Periodontal Health
CHAPTER Periodontal Health, Gingival Diseases 6 and Conditions Section 1 Periodontal Health 99 Section 2 Dental Plaque-Induced Gingival Conditions 101 Classification of Plaque-Induced Gingivitis and Modifying Factors Plaque-Induced Gingivitis Modifying Factors of Plaque-Induced Gingivitis Drug-Influenced Gingival Enlargements Section 3 Non–Plaque-Induced Gingival Diseases 111 Description of Selected Disease Disorders Description of Selected Inflammatory and Immune Conditions and Lesions Section 4 Focus on Patients 117 Clinical Patient Care Ethical Dilemma Clinical Application. Examination of the gingiva is part of every patient visit. In this context, a thorough clinical and radiographic assessment of the patient’s gingival tissues provides the dental practitioner with invaluable diagnostic information that is critical to determining the health status of the gingiva. The dental hygienist is often the first member of the dental team to be able to detect the early signs of periodontal disease. In 2017, the American Academy of Periodontology (AAP) and the European Federation of Periodontology (EFP) developed a new worldwide classification scheme for periodontal and peri-implant diseases and conditions. Included in the new classification scheme is the category called “periodontal health, gingival diseases/conditions.” Therefore, this chapter will first review the parameters that define periodontal health. Appreciating what constitutes as periodontal health serves as the basis for the dental provider to have a stronger understanding of the different categories of gingival diseases and conditions that are commonly encountered in clinical practice. Learning Objectives • Define periodontal health and be able to describe the clinical features that are consistent with signs of periodontal health. • List the two major subdivisions of gingival disease as established by the American Academy of Periodontology and the European Federation of Periodontology. -

Gingival Diseases in Children and Adolescents
8932 Indian Journal of Forensic Medicine & Toxicology, October-December 2020, Vol. 14, No. 4 Gingival Diseases in Children and Adolescents Sulagna Pradhan1, Sushant Mohanty2, Sonu Acharya3, Mrinali Shukla1, Sonali Bhuyan1 1Post Graduate Trainee, 2Professor & Head, 3Professor, Department of Paediatric and Preventive Dentistry, Institute of Dental Sciences, Siksha O Anusandhan (Deemed to be University), Bhubaneswar 751003, Odisha, India Abstract Gingival diseases are prevalent in both children and adolescents. These diseases may or may not be associated with plaques, maybe familial in some cases, or may coexist with systemic illness. However, gingiva and periodontium receive scant attention as the primary dentition does not last for a considerable duration. As gingival diseases result in the marked breakdown of periodontal tissue, and premature tooth loss affecting the nutrition and global development of a child/adolescent, precise identification and management of gingival diseases is of paramount importance. This article comprehensively discusses the nature, spectrum, and management of gingival diseases. Keywords: Gingival diseases; children and adolescents; spectrum, and management. Introduction reddish epithelium with mild keratinization may be misdiagnosed as inflammation. Lesser variability in the Children are more susceptible to several gingival width of the attached gingiva in the primary dentition diseases, paralleling to those observed in adults, though results in fewer mucogingival problems. The interdental vary in numerous aspects. Occasionally, natural variations papilla is broad buccolingual, and narrow mesiodistally. in the gingiva can masquerade as genuine pathology.1 The junctional epithelium associated with the deciduous On the contrary, a manifestation of a life-threatening dentition is thicker than the permanent dentition. underlying condition is misdiagnosed as normal gingiva.