Identification of Rare Variants of DSP Gene in Sudden Unexplained Nocturnal Death Syndrome in the Southern Chinese Han Population
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PSPC1 Potentiates IGF1R Expression to Augment Cell Adhesion and Motility
1 Supplementary information 2 PSPC1 potentiates IGF1R expression to augment cell 3 adhesion and motility 4 Hsin-Wei Jen1,2 , De-Leung Gu 2, Yaw-Dong Lang 2 and Yuh-Shan Jou 1,2,* 5 1 Graduate Institute of Life Sciences, National Defense Medical Center, Taipei, Taiwan 6 2 Institute of Biomedical Sciences, Academia Sinica, Taipei, Taiwan 7 * Author to whom correspondence should be addressed 8 Cells 2020, 9, x; doi: FOR PEER REVIEW www.mdpi.com/journal/cells Cells 2020, 9, x FOR PEER REVIEW 2 of 10 9 10 11 Supplementary Figure S1: Expression of IGF1R and integrin in PSPC1-expressing or PSPC1-depleted 12 HCC cells by Western blotting analysis 13 (A) Detection of IGF1R protein levels in three PSPC1-knockdown cells Huh7, HepG2 and Mahlavu. (B) 14 Detection of selected integrin expression in PSPC1-overexpressing or PSPC1-depleted HCC cells by using 15 their total cell lysates immunoblotted with specific integrin antibodies as shown. 16 17 18 Supplementary Figure S2: PSPC1-modulated IGF1R downstream signaling in HCC cells. Cells 2020, 9, x FOR PEER REVIEW 3 of 10 19 (A, B) Immunoblotting of IGF1R expression in PSPC1-overexpressing SK-Hep1 and PLC5 cells 20 treated with IGF1R shRNAs. (C, D) Cell migration and adhesion were measured in PSPC1- 21 knockdown Hep3B cells rescued with exogenous expression of IGF1R. Exogenous expression of 22 IGF1R in PSPC1-knockdown Hep3B cells were then applied for detection of altered AKT/ERK 23 signaling including (E) total PSPC1, IGF1R, AKT, ERK, p-IGF1R, p-AKT(S473), and 24 p-ERK(T202/Y204) as well as altered FAK/Src signaling including (F) total FAK, Src, p-FAK(Y397) 25 and p-Src(Y416) by immunoblotting assay. -

Novel Association of Hypertrophic Cardiomyopathy, Sensorineural Deafness, and a Mutation in Unconventional Myosin VI (MYO6)
309 LETTER TO JMG J Med Genet: first published as 10.1136/jmg.2003.011973 on 1 April 2004. Downloaded from Novel association of hypertrophic cardiomyopathy, sensorineural deafness, and a mutation in unconventional myosin VI (MYO6) S A Mohiddin, Z M Ahmed, A J Griffith, D Tripodi, T B Friedman, L Fananapazir, R J Morell ............................................................................................................................... J Med Genet 2004;41:309–314. doi: 10.1136/jmg.2003.011973 amilial hypertrophic cardiomyopathy (FHC) is typically Key points characterised by left ventricular hypertrophy, diastolic Fdysfunction, and hypercontractility, and is often asso- ciated with disabling symptoms, arrhythmias, and sudden N Familial hypertrophic cardiomyopathy (FHC) is typi- death.1 FHC shows both non-allelic and allelic genetic cally confined to a cardiac phenotype and is caused by heterogeneity, and results from any one of more than 100 mutations in genes encoding sarcomeric proteins. mutations in genes encoding sarcomeric proteins.2 Identified Occasionally FHC may be one component of a genes include those encoding b myosin heavy chain, the hereditary multisystem disorder. myosin regulatory and essential light chains, myosin bind- N Sensorineural hearing loss is genetically heteroge- ing protein C, troponin I, troponin C, a cardiac actin, and neous. Mutations in the MYO6 gene, encoding 23 titin. The FHC phenotype is characterised by hypertrophy, unconventional myosin VI, have been found to cause myocyte disarray and fibrosis, and results from the dominant non-syndromic sensorineural hearing loss—that is, negative expression of one of these (mainly missense) sensorineural hearing loss in the absence of any other mutations. The resulting sarcomeric dysfunction leads related clinical features. ultimately, through mechanisms that remain obscure, to pathological left ventricular remodelling. -

Notch-Wnt-Bmp Crosstalk Regulates Radial Patterning in the Mouse Cochlea in a Spatiotemporal Manner Vidhya Munnamalai1,2 and Donna M
© 2016. Published by The Company of Biologists Ltd | Development (2016) 143, 4003-4015 doi:10.1242/dev.139469 RESEARCH ARTICLE Notch-Wnt-Bmp crosstalk regulates radial patterning in the mouse cochlea in a spatiotemporal manner Vidhya Munnamalai1,2 and Donna M. Fekete1,2,3,* ABSTRACT development progresses (Munnamalai and Fekete, 2013). Wnt- The sensory cells of the mammalian organ of Corti assume a precise mediated regulation of cell proliferation is well known in many mosaic arrangement during embryonic development. Manipulation of organ systems, including the cochlea (Jacques et al., 2012). Whether Wnt signaling can modulate the proliferation of cochlear progenitors, the canonical Wnt signaling pathway intersects with the Notch, but whether Wnts are responsible for patterning compartments, or Bmp or Fgf pathways to regulate cochlear patterning remains specific hair cells within them, is unclear. To address how the precise relatively unexplored. timing of Wnt signaling impacts patterning across the radial axis, The Wnt and Notch pathways are known to crosstalk, a finding ‘ ’ mouse cochlear cultures were initiated at embryonic day 12.5 and that coined the term Wntch signaling. This interaction is context subjected to pharmacological treatments at different stages. Early dependent and can be bi-directional (Collu et al., 2014; Zak et al., changes in major patterning genes were assessed to understand the 2015). In the cochlea, Notch has a dual role in regulating lateral mechanisms underlying alterations of compartments. Results show induction early (to induce prosensory fate) and lateral inhibition that Wnt activation can promote medial cell fates by regulating later (to block HC fate) (Kiernan, 2013). Studies have shown that medially expressed Notch genes in a spatiotemporal manner. -
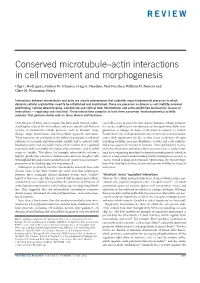
Conserved Microtubule–Actin Interactions in Cell Movement and Morphogenesis
REVIEW Conserved microtubule–actin interactions in cell movement and morphogenesis Olga C. Rodriguez, Andrew W. Schaefer, Craig A. Mandato, Paul Forscher, William M. Bement and Clare M. Waterman-Storer Interactions between microtubules and actin are a basic phenomenon that underlies many fundamental processes in which dynamic cellular asymmetries need to be established and maintained. These are processes as diverse as cell motility, neuronal pathfinding, cellular wound healing, cell division and cortical flow. Microtubules and actin exhibit two mechanistic classes of interactions — regulatory and structural. These interactions comprise at least three conserved ‘mechanochemical activity modules’ that perform similar roles in these diverse cell functions. Over the past 35 years, great progress has been made towards under- crosstalk occurs in processes that require dynamic cellular asymme- standing the roles of the microtubule and actin cytoskeletal filament tries to be established or maintained to allow rapid intracellular reor- systems in mechanical cellular processes such as dynamic shape ganization or changes in shape or direction in response to stimuli. change, shape maintenance and intracellular organelle movement. Furthermore, the widespread occurrence of these interactions under- These functions are attributed to the ability of polarized cytoskeletal scores their importance for life, as they occur in diverse cell types polymers to assemble and disassemble rapidly, and to interact with including epithelia, neurons, fibroblasts, oocytes and early embryos, binding proteins and molecular motors that mediate their regulated and across species from yeast to humans. Thus, defining the mecha- movement and/or assembly into higher order structures, such as radial nisms by which actin and microtubules interact is key to understand- arrays or bundles. -

Myosin Motors: Novel Regulators and Therapeutic Targets in Colorectal Cancer
cancers Review Myosin Motors: Novel Regulators and Therapeutic Targets in Colorectal Cancer Nayden G. Naydenov 1, Susana Lechuga 1, Emina H. Huang 2 and Andrei I. Ivanov 1,* 1 Department of Inflammation and Immunity, Lerner Research Institute, Cleveland Clinic Foundation, Cleveland, OH 44195, USA; [email protected] (N.G.N.); [email protected] (S.L.) 2 Departments of Cancer Biology and Colorectal Surgery, Cleveland Clinic Foundation, Cleveland, OH 44195, USA; [email protected] * Correspondence: [email protected]; Tel.: +1-216-445-5620 Simple Summary: Colorectal cancer (CRC) is a deadly disease that may go undiagnosed until it presents at an advanced metastatic stage for which few interventions are available. The develop- ment and metastatic spread of CRC is driven by remodeling of the actin cytoskeleton in cancer cells. Myosins represent a large family of actin motor proteins that play key roles in regulating actin cytoskeleton architecture and dynamics. Different myosins can move and cross-link actin filaments, attach them to the membrane organelles and translocate vesicles along the actin filaments. These diverse activities determine the key roles of myosins in regulating cell proliferation, differ- entiation and motility. Either mutations or the altered expression of different myosins have been well-documented in CRC; however, the roles of these actin motors in colon cancer development remain poorly understood. The present review aims at summarizing the evidence that implicate myosin motors in regulating CRC growth and metastasis and discusses the mechanisms underlying the oncogenic and tumor-suppressing activities of myosins. Abstract: Colorectal cancer (CRC) remains the third most common cause of cancer and the second most common cause of cancer deaths worldwide. -

Novel Myosin Mutations for Hereditary Hearing Loss Revealed by Targeted Genomic Capture and Massively Parallel Sequencing
European Journal of Human Genetics (2014) 22, 768–775 & 2014 Macmillan Publishers Limited All rights reserved 1018-4813/14 www.nature.com/ejhg ARTICLE Novel myosin mutations for hereditary hearing loss revealed by targeted genomic capture and massively parallel sequencing Zippora Brownstein1,6, Amal Abu-Rayyan2,6, Daphne Karfunkel-Doron1, Serena Sirigu3, Bella Davidov4, Mordechai Shohat1,4, Moshe Frydman1,5, Anne Houdusse3, Moien Kanaan2 and Karen B Avraham*,1 Hereditary hearing loss is genetically heterogeneous, with a large number of genes and mutations contributing to this sensory, often monogenic, disease. This number, as well as large size, precludes comprehensive genetic diagnosis of all known deafness genes. A combination of targeted genomic capture and massively parallel sequencing (MPS), also referred to as next-generation sequencing, was applied to determine the deafness-causing genes in hearing-impaired individuals from Israeli Jewish and Palestinian Arab families. Among the mutations detected, we identified nine novel mutations in the genes encoding myosin VI, myosin VIIA and myosin XVA, doubling the number of myosin mutations in the Middle East. Myosin VI mutations were identified in this population for the first time. Modeling of the mutations provided predicted mechanisms for the damage they inflict in the molecular motors, leading to impaired function and thus deafness. The myosin mutations span all regions of these molecular motors, leading to a wide range of hearing phenotypes, reinforcing the key role of this family of proteins in auditory function. This study demonstrates that multiple mutations responsible for hearing loss can be identified in a relatively straightforward manner by targeted-gene MPS technology and concludes that this is the optimal genetic diagnostic approach for identification of mutations responsible for hearing loss. -

Genome-Wide Identification, Characterization and Expression
G C A T T A C G G C A T genes Article Genome-Wide Identification, Characterization and Expression Profiling of myosin Family Genes in Sebastes schlegelii Chaofan Jin 1, Mengya Wang 1,2, Weihao Song 1 , Xiangfu Kong 1, Fengyan Zhang 1, Quanqi Zhang 1,2,3 and Yan He 1,2,* 1 MOE Key Laboratory of Molecular Genetics and Breeding, College of Marine Life Sciences, Ocean University of China, Qingdao 266003, China; [email protected] (C.J.); [email protected] (M.W.); [email protected] (W.S.); [email protected] (X.K.); [email protected] (F.Z.); [email protected] (Q.Z.) 2 Laboratory of Tropical Marine Germplasm Resources and Breeding Engineering, Sanya Oceanographic Institution, Ocean University of China, Sanya 572000, China 3 Laboratory for Marine Fisheries Science and Food Production Processes, Qingdao National Laboratory for Marine Science and Technology, Qingdao 266003, China * Correspondence: [email protected]; Tel.: +86-0532-82031986 Abstract: Myosins are important eukaryotic motor proteins that bind actin and utilize the energy of ATP hydrolysis to perform a broad range of functions such as muscle contraction, cell migration, cytokinesis, and intracellular trafficking. However, the characterization and function of myosin is poorly studied in teleost fish. In this study, we identified 60 myosin family genes in a marine teleost, black rockfish (Sebastes schlegelii), and further characterized their expression patterns. myosin showed divergent expression patterns in adult tissues, indicating they are involved in different types and Citation: Jin, C.; Wang, M.; Song, W.; compositions of muscle fibers. Among 12 subfamilies, S. schlegelii myo2 subfamily was significantly Kong, X.; Zhang, F.; Zhang, Q.; He, Y. -

Graf1 Regulates Myo6 Dependent Mitochondrial Actin Remodeling
GRAF1 REGULATES MYO6 DEPENDENT MITOCHONDRIAL ACTIN REMODELING Zachary Opheim A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master of Science in the Department of Pathology and Laboratory Medicine in the School of Medicine. Chapel Hill 2019 Approved by: Joan Taylor Chris Mack Jon Homeister © 2019 ZACHARY OPHEIM ALL RIGHTS RESERVED ii ABSTRACT Zachary Opheim: GRAF1 Regulates MYO6 Dependent Mitochondrial Actin Remodeling (Under the direction of Joan Taylor) Cardiomyocytes are long lived cells that require a constant supply of ATP generated by mitochondria. Mitochondrial dysfunction results in various diseases, highlighting the importance of mitochondrial quality control. Here we demonstrate that GRAF1 regulates mitochondrial quality via interaction with MYO6, a known regulator of mitophagy. Recent studies revealed MYO6 promotes the formation of actin “cages” around damaged mitochondria in response to stress. We show GRAF1 and MYO6 co- localize to depolarized mitochondria. Additionally, we reveal GRAF1 and MYO6 interact and is dependent upon actin polymerization. Knockdown of GRAF1 results in clustered mitochondrial network morphology following mitochondrial depolarization and subsequent recovery. Furthermore, we observe a lack of MYO6 dissociation from mitochondria following knockdown of GRAF1. In addition, GRAF1 was found to promote mitochondrial function in growth conditions requiring mitochondrial dependent oxidative phosphorylation. Our -

Cytoskeletal Remodeling in Cancer
biology Review Cytoskeletal Remodeling in Cancer Jaya Aseervatham Department of Ophthalmology, University of Texas Health Science Center at Houston, Houston, TX 77054, USA; [email protected]; Tel.: +146-9767-0166 Received: 15 October 2020; Accepted: 4 November 2020; Published: 7 November 2020 Simple Summary: Cell migration is an essential process from embryogenesis to cell death. This is tightly regulated by numerous proteins that help in proper functioning of the cell. In diseases like cancer, this process is deregulated and helps in the dissemination of tumor cells from the primary site to secondary sites initiating the process of metastasis. For metastasis to be efficient, cytoskeletal components like actin, myosin, and intermediate filaments and their associated proteins should co-ordinate in an orderly fashion leading to the formation of many cellular protrusions-like lamellipodia and filopodia and invadopodia. Knowledge of this process is the key to control metastasis of cancer cells that leads to death in 90% of the patients. The focus of this review is giving an overall understanding of these process, concentrating on the changes in protein association and regulation and how the tumor cells use it to their advantage. Since the expression of cytoskeletal proteins can be directly related to the degree of malignancy, knowledge about these proteins will provide powerful tools to improve both cancer prognosis and treatment. Abstract: Successful metastasis depends on cell invasion, migration, host immune escape, extravasation, and angiogenesis. The process of cell invasion and migration relies on the dynamic changes taking place in the cytoskeletal components; actin, tubulin and intermediate filaments. This is possible due to the plasticity of the cytoskeleton and coordinated action of all the three, is crucial for the process of metastasis from the primary site. -

Estradiol Activates B-Catenin Dependent Transcription in Neurons
Estradiol Activates b-Catenin Dependent Transcription in Neurons Olga Varea1, Juan Jose Garrido1,4, Ana Dopazo2, Pablo Mendez3, Luis Miguel Garcia-Segura3, Francisco Wandosell1* 1 Centro de Investigacio´n Biome´dica en Red sobre Enfermedades Neurodegenerativas (CIBERNED) and Centro de Biologı´a Molecular ‘‘Severo Ochoa’’, CSIC-UAM, Madrid, Spain, 2 Genomics Unit, Centro Nacional de Investigaciones Cardiovasculares (CNIC), Madrid, Spain, 3 Laboratory of Neuroactive Steroids, Instituto Cajal, CSIC, Madrid, Spain, 4 Laboratory of Neuronal Polarity, Instituto Cajal, CSIC, Madrid, Spain Abstract Estradiol may fulfill a plethora of functions in neurons, in which much of its activity is associated with its capacity to directly bind and dimerize estrogen receptors. This hormone-protein complex can either bind directly to estrogen response elements (ERE’s) in gene promoters, or it may act as a cofactor at non-ERE sites interacting with other DNA-binding elements such as AP- 1 or c-Jun. Many of the neuroprotective effects described for estrogen have been associated with this mode of action. However, recent evidence suggests that in addition to these ‘‘genomic effects’’, estrogen may also act as a more general ‘‘trophic factor’’ triggering cytoplasmic signals and extending the potential activity of this hormone. We demonstrated that estrogen receptor alpha associates with b-catenin and glycogen synthase kinase 3 in the brain and in neurons, which has since been confirmed by others. Here, we show that the action of estradiol activates b-catenin transcription in neuroblastoma cells and in primary cortical neurons. This activation is time and concentration-dependent, and it may be abolished by the estrogen receptor antagonist ICI 182780. -

Myosin VB in Intestinal Pathogenesis Fernando Cartón García
ADVERTIMENT. Lʼaccés als continguts dʼaquesta tesi queda condicionat a lʼacceptació de les condicions dʼús establertes per la següent llicència Creative Commons: http://cat.creativecommons.org/?page_id=184 ADVERTENCIA. El acceso a los contenidos de esta tesis queda condicionado a la aceptación de las condiciones de uso establecidas por la siguiente licencia Creative Commons: http://es.creativecommons.org/blog/licencias/ WARNING. The access to the contents of this doctoral thesis it is limited to the acceptance of the use conditions set by the following Creative Commons license: https://creativecommons.org/licenses/?lang=en Myosin VB in intestinal pathogenesis Doctoral thesis presented by Fernando Cartón García For the PhD degree Biochemistry, Molecular Biology and Biomedicine doctorate program Biochemistry and Molecular Biology Department Faculty of Medicine Universidad Autónoma de Barcelona Work carried out in Group of Biomedical Research in Digestive Tract Tumors Molecular Biology and Biochemistry Research Center (CIBBIM-Nanomedicine) Vall d’Hebron Research Institute June 2017 DIRECTOR ACADEMIC TUTOR Dr. Diego Arango Dr. Joan Seoane PhD STUDENT Fernando Cartón 2 INDEX RESUMEN ................................................................................. 6 ABSTRACT ............................................................................... 8 INTRODUCTION ..................................................................... 10 1. The human digestive tract .................................................. 10 1.1 Anatomy and Histology -

Conformational Distributions of Isolated Myosin Motor Domains
RESEARCH ARTICLE Conformational distributions of isolated myosin motor domains encode their mechanochemical properties Justin R Porter1, Artur Meller1, Maxwell I Zimmerman1, Michael J Greenberg1, Gregory R Bowman1,2* 1Department of Biochemistry and Molecular Biophysics, Washington University School of Medicine in St. Louis, St. Louis, United States; 2Center for the Science and Engineering of Living Systems, Washington University in St. Louis, St. Louis, United States Abstract Myosin motor domains perform an extraordinary diversity of biological functions despite sharing a common mechanochemical cycle. Motors are adapted to their function, in part, by tuning the thermodynamics and kinetics of steps in this cycle. However, it remains unclear how sequence encodes these differences, since biochemically distinct motors often have nearly indistinguishable crystal structures. We hypothesized that sequences produce distinct biochemical phenotypes by modulating the relative probabilities of an ensemble of conformations primed for different functional roles. To test this hypothesis, we modeled the distribution of conformations for 12 myosin motor domains by building Markov state models (MSMs) from an unprecedented two milliseconds of all-atom, explicit-solvent molecular dynamics simulations. Comparing motors reveals shifts in the balance between nucleotide-favorable and nucleotide-unfavorable P-loop conformations that predict experimentally measured duty ratios and ADP release rates better than sequence or individual structures. This result demonstrates the power of an ensemble perspective for interrogating sequence-function relationships. *For correspondence: [email protected] Competing interests: The authors declare that no Introduction competing interests exist. Myosin motors (Figure 1A) perform an extraordinary diversity of biological functions despite sharing Funding: See page 17 a common mechanochemical cycle.