Metrowest Region, Massachusetts 2016 Community Health Assessment
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Older Workers Rock! We’Re Not Done Yet!
TM TM Operation A.B.L.E. 174 Portland Street Tel: 617.542.4180 5th Floor E: [email protected] Boston, MA 02114 W: www.operationable.net Older Workers Rock! We’re Not Done Yet! A.B.L.E. SCSEP Office Locations: SCSEP Suffolk County, MA Workforce Central SCSEP Hillsborough County, NH 174 Portland Street, 5th Floor 340 Main Street 228 Maple Street., Ste 300 Boston, MA 02114 Ste.400 Manchester, NH 03103 Phone: 617.542.4180 Worcester, MA 01608 Phone: 603.206.4405 eMail: [email protected] Tel: 508.373.7685 eMail: [email protected] eMail: [email protected] SCSEP Norfolk, Metro West & SCSEP Coos County, NH Worcester Counties, MA Career Center 961 Main Street Quincy SCSEP Office of North Central MA Berlin, NH 03570 1509 Hancock Street, 4th Floor 100 Erdman Way Phone: 603.752.2600 Quincy, MA 02169 Leominster, MA 01453 eMail: [email protected] Phone: 617-302-2731 Tel: 978.534.1481 X261 and 617-302-3597 eMail: [email protected] eMail: [email protected] South Middlesex GETTING WORKERS 45+ BACK TO WORK SINCE 1982 SCSEP Essex & Middlesex Opportunity Council Counties, MA 7 Bishop Street Job Search Workshops | Coaching & Counseling | Training | ABLE Friendly Employers | Resource Room Framingham, MA 01702 280 Merrimack Street Internships | Apprenticeships | Professional Networking | Job Clubs | Job Seeker Events Building B, Ste. 400 Tel: 508.626.7142 Lawerence, MA 01843 eMail: [email protected] Phone: 978.651.3050 eMail: [email protected] 2018 Annual Report September 2018 At Operation A.B.L.E., we work very hard to Operation A.B.L.E. Addresses the Changing Needs keep the quality of our programs up and our costs down. -

Changes to Transit Service in the MBTA District 1964-Present
Changes to Transit Service in the MBTA district 1964-2021 By Jonathan Belcher with thanks to Richard Barber and Thomas J. Humphrey Compilation of this data would not have been possible without the information and input provided by Mr. Barber and Mr. Humphrey. Sources of data used in compiling this information include public timetables, maps, newspaper articles, MBTA press releases, Department of Public Utilities records, and MBTA records. Thanks also to Tadd Anderson, Charles Bahne, Alan Castaline, George Chiasson, Bradley Clarke, Robert Hussey, Scott Moore, Edward Ramsdell, George Sanborn, David Sindel, James Teed, and George Zeiba for additional comments and information. Thomas J. Humphrey’s original 1974 research on the origin and development of the MBTA bus network is now available here and has been updated through August 2020: http://www.transithistory.org/roster/MBTABUSDEV.pdf August 29, 2021 Version Discussion of changes is broken down into seven sections: 1) MBTA bus routes inherited from the MTA 2) MBTA bus routes inherited from the Eastern Mass. St. Ry. Co. Norwood Area Quincy Area Lynn Area Melrose Area Lowell Area Lawrence Area Brockton Area 3) MBTA bus routes inherited from the Middlesex and Boston St. Ry. Co 4) MBTA bus routes inherited from Service Bus Lines and Brush Hill Transportation 5) MBTA bus routes initiated by the MBTA 1964-present ROLLSIGN 3 5b) Silver Line bus rapid transit service 6) Private carrier transit and commuter bus routes within or to the MBTA district 7) The Suburban Transportation (mini-bus) Program 8) Rail routes 4 ROLLSIGN Changes in MBTA Bus Routes 1964-present Section 1) MBTA bus routes inherited from the MTA The Massachusetts Bay Transportation Authority (MBTA) succeeded the Metropolitan Transit Authority (MTA) on August 3, 1964. -

Community Partners Directory R
COMMUNITY PARTNERS DIRECTORY R 1 2 Table of Contents Message from the Executive Director………………………………………………………………………………….. 4 ORI Program Descriptions……………………………………………………………………………………………………. 6 ORI Providers Listed by Service Type…………………………………………………………………………………… 7 ORI Provider Service Map……………………………………………………………………………………………………. 11 Provider Summaries………………………………………………………………………………………………………..….. 12 EOHHS State Agencies…………………………………………………………………………………………………………. 34 3 The Commonwealth of Massachusetts Executive Office of Health and Human Services Office for Refugees and Immigrants 600 Washington Street, 4th Floor Boston, Massachusetts 02111 CHARLES D. BAKER Tel: (617) 727-7888 Governor Fax: (617) 727-1822 TTY: (617) 727-8147 KARYN E. POLITO Lieutenant Governor MARYLOU SUDDERS MARY TRUONG Secretary Executive Director March 15, 2018 Dear Community Partners and Friends, When we released our first edition of the Community Partners Directory, it delighted us to hear how well-received it was, especially by our community partners and stakeholders here in Massachusetts. It is with that same enthusiasm that we release an updated edition of the Community Partners Directory in a user-friendly format. This new edition features a list of all ORI programs with a brief description of each, followed by a list of the providers that offer each program. After, the directory lists each provider more thoroughly, including their contact information and location. It is our hope that this directory will allow community partners and stakeholders to collaborate in order to best serve the immigrants and refugees residing in Massachusetts. Every effort has been made to ensure that this directory is accurate and up to date. This second edition is special because it includes ORI’s new partners for the newest addition to ORI’s portfolio of programs, the Financial Literacy for Newcomers (FLNP). -

Emergency Services Program (Esps)
Emergency Services Program (ESPs) Emergency Service Programs (ESPs) provide community-based assessment, intervention, and stabilization services for people experiencing mental health or substance use related crisis. hey can tal! to people "ho feel they are in or near crisis, and try to help them find the supports they need to manage the crisis. ESPs are available #$ hours a day, % days a "ee!, &'( days a year. Statewide ESP )umber Call 1-877-382-1609 and enter your zipcode (or use the direct number belo") )ortheastern *assachusetts +mesbury, ,everly, ,oxford, -anvers, Essex, .eorgeto"n, .loucester, 3ahey4)ortheast .roveland, /amilton, /averhill, 0ps"ich, *anchester by the Sea, North Essex *arblehead, *errimac, *iddleton, )e"bury, )e"buryport, Peabody, ,ehavioral /ealth 1oc!port, 1o"ley, Salem, Salisbury, opsfield, 2enham, 2est )e"bury 1-866-523-1216 +ndover, 3a"rence, *ethuen, )orth +ndover 3ahey4)ortheast a!rence ,ehavioral /ealth area 1-877-255-1261 ,illerica, 5helmsford, -racut, -unstable, 3o"ell, e"!sbury, yngsboro, 3ahey4)ortheast o!ell area 2estford ,ehavioral /ealth 1-800-830-5177 Everett, 3ynn, 3ynnfield, *alden, *edford, *elrose, )ahant, )orth 1eading, Eliot Community "ri-City 1eading, Saugus, Stoneham, S"ampscott, 2a!efield /uman Services 1-800-988-1111 *etro ,oston ,oston Boston, Broo!line, Chelsea, Revere, Winthrop ,oston Emergency #oston area Services eam 1-800-981-$357 5ambridge, Somerville Cambridge Somerville Ca%&rid'e ( Emergency Services So%er*ille 1-800-981-$357 Southeastern *assachusetts ,raintree, Cohasset, Hingham, -

TOWN of ACTON 2020 ANNUAL TOWN REPORT Town of Acton
TOWN TOWN ACTON OF 2020 ANNUAL TOWN REPORT TOWN ANNUAL 2020 TOWN OF ACTON 2020 ANNUAL TOWN REPORT Town of Acton Incorporated as a Town: July 3, 1735 Type of Government: Town Meetings ~ Board of Selectmen/Town Manager Location: Eastern Massachusetts, Middlesex County, bordered on the east by Carlisle and Concord, on the west by Boxborough, on the north by Westford and Littleton, on the south by Sudbury, and on the southwest by Stow and Maynard. Elevation at Town Hall: 268’ above mean sea level Land Area: Approximately 20 square miles Population: Year Persons 1950 3,510 1960 7.238 1970 14,770 1980 19,000 1990 18,144 2000 20,331 2010 21,936 2020 22,170 Report Cover: (Top and Bottom Left) Groundbreaking at the North Acton Fire Station; (Top and Bottom Right) Ribbon Cutting Ceremony for the Miracle Field Sports Pavilion Photos courtesy of Town Staff 2020 Annual Reports Town of Acton, Massachusetts Two Hundred and Eighty Fifth Municipal Year For the year ending December 31, 2020 TABLE OF CONTENTS 1. Administrative Services 8. Public Works Board of Selectmen 4 DPW/Highway 96 Town Manager 5 Green Advisory Board 97 Public Facilities 99 2. Financial Management Services Board of Assessors 8 9. Community Safety House Sales 9 Animal Control Officer 101 Finance Committee 18 Animal Inspector 101 Town Accountant 18 Emergency Management Agency 101 Fire Department 101 3. Human Services Auxiliary Fire Department 109 Acton Housing Authority 28 Police Department 109 Acton Nursing Services 29 Commission on Disabilities 31 10. Legislative Community Housing Corporation 32 Annual Town Meeting, June 29, 2020 116 Community Services Coordinator 35 Special Town Meeting, September 8, 2020 127 Council on Aging 35 Health Insurance Trust 37 11. -
FORM B BUILDING Assessor’S Number USGS Quad Area(S) Form Number
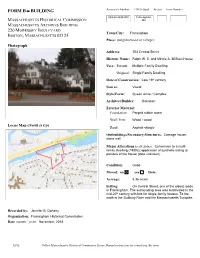
FORM B BUILDING Assessor’s Number USGS Quad Area(s) Form Number 069-68-4339-000 Framingham, MASSACHUSETTS HISTORICAL COMMISSION MA MASSACHUSETTS ARCHIVES BUILDING 220 MORRISSEY BOULEVARD Town/City: Framingham BOSTON, MASSACHUSETTS 02125 Place: (neighborhood or village): Photograph Address: 703 Central Street Historic Name: Ralph W. E. and Minnie A. Milliken House Uses: Present: Multiple Family Dwelling Original: Single Family Dwelling Date of Construction: Late 19th century Source: Visual Style/Form: Queen Anne / Complex Architect/Builder: Unknown Exterior Material: Foundation: Parged rubble stone Wall/Trim: Wood / wood Locus Map (North is Up) Roof: Asphalt shingle Outbuildings/Secondary Structures: Carriage house, stone wall Major Alterations (with dates): Conversion to a multi- family dwelling (1980s); application of synthetic siding to portions of the house (date unknown) Condition: Good Moved: no yes Date: Acreage: 5.36 acres On Central Street, one of the oldest roads Setting: in Framingham. The surrounding area was subdivided in the mid-20th century with lots for single-family houses. To the north is the Sudbury River and the Massachusetts Turnpike. Recorded by: Jennifer B. Doherty Organization: Framingham Historical Commission Date (month / year): November, 2018 12/12 Follow Massachusetts Historical Commission Survey Manual instructions for completing this form. INVENTORY FORM B CONTINUATION SHEET FRAMINGHAM 703 CENTRAL STREET MASSACHUSETTS HISTORICAL COMMISSION Area(s) Form No. 220 MORRISSEY BOULEVARD, BOSTON, MASSACHUSETTS 02125 Recommended for listing in the National Register of Historic Places. If checked, you must attach a completed National Register Criteria Statement form. Use as much space as necessary to complete the following entries, allowing text to flow onto additional continuation sheets. -
CHANGING FACES of GREATER BOSTON a REPORT from BOSTON INDICATORS, the BOSTON FOUNDATION, UMASS BOSTON and the UMASS DONAHUE INSTITUTE the PROJECT TEAM
CHANGING FACES of GREATER BOSTON A REPORT FROM BOSTON INDICATORS, THE BOSTON FOUNDATION, UMASS BOSTON AND THE UMASS DONAHUE INSTITUTE THE PROJECT TEAM BOSTON INDICATORS is the research center at the UMASS BOSTON (UMB) is one of only two universities in Boston Foundation, which works to advance a thriving Greater the country with free-standing research institutes dedicated to Boston for all residents across all neighborhoods. We do this four major communities of color in the U.S. Working together by analyzing key indicators of well-being and by researching and individually, these institutes offer thought leadership to promising ideas for making our city more prosperous, equitable help shape public understanding of the evolving racial and and just. To ensure that our work informs active efforts to ethnic diversities in Boston, Massachusetts, and beyond. improve our city, we work in deep partnership with community The four research institutes are: groups, civic leaders and Boston’s civic data community to THE INSTITUTE FOR ASIAN AMERICAN produce special reports and host public convenings. STUDIES (IAAS) utilizes resources and expertise from THE BOSTON FOUNDATION is is one of the largest the university and the community to conduct research and oldest community foundations in America, with net assets on Asian Americans; to strengthen and further Asian of $1.3 billion. The Foundation is a partner in philanthropy, with American involvement in political, economic, social, and some 1,100 charitable funds established for the general benefit cultural life; and to improve opportunities and campus of the community or for special purposes. It also serves as a life for Asian American faculty, staff, and students and for major civic leader, think tank and advocacy organization dedi- those interested in Asian Americans. -

2019 Annual Report
2019 ANNUAL REPORT OUR M ISSION The Boys & Girls Clubs of MetroWest provides social, educational, physical, and cultural programming for boys and girls in the MetroWest area. The intent of these programs is to enhance the development of children and to prepare young adults to be responsible and productive members of the community. OUR PROGRAM S Character & Leadership Keystone Club Torch Club Youth of the Year Education & Career Project Learn Money Matters Power Hour Career Launch Club Tech Healt h & Life Skills SMART Mo ves SMART Girls Passport to Manhood Sports, Fitness & Recreation Triple Play Youth Basketball Program Happy Hours Preschool Happy Hours Preschool, located in the Marlborough Clubhouse, is fully licensed by the Department of Early Education and Care. Our group of teachers provide a safe and nurturing environment where opportunities for small group, as well as large group, activities focus on developing physical, intellectual, social, and emotional growth. Classes are offered for children 2.9 years to 5 years of age. Discovery Club The Discovery Club before and after-school child care program at the Marlborough Clubhouse and four Marlborough public schools is fully licensed by the Department of Early Education and Care. We m aintain a 1:13 staff to child ratio, provide a diverse program curriculum, and offer daily healthy snacks. The program curriculum offers structured activities and classes designed to create a balance between having fun and working to enrich educational and life experiences. Faces of the Future Framingham Clubhouse Nathan R., Age 8, Third Grade Member since 2019 What is your favorite thing to do at the club? “Playing air hockey and pool in the Games Rooms with my friends.” What is your favorite Club memory? “When I won my first game of air hockey!” What do you want to be when you grow up? “A construction worker.” Argeo R. -
Density Through Design
DENSITY THROUGH DESIGN A SUMMARY OF THE 495/METROWEST PARTNERSHIP’S HOUSING DENSITY PROJECT A PUBLICATION OF THE 495/METROWEST PARTNERSHIP, INC. 200 Friberg Parkway, Suite 1003 • Westborough, MA 01581 • Phone: 774.760.0495 • Fax: 774.760.0017 • www.495Partnership.org 200 Friberg Parkway, Suite 1003 • Westborough, MA 01581 • Phone: 774.760.0495 • Fax: 774.760.0017 • www.495Partnership.org Acknowledgements This report was written by Adam Ploetz, AICP, the Partnership’s Manager of Sustainable Development Programs. The author wishes to express his thanks to the graduate students from the University of Massachusetts Amherst’s Department of Landscape Architecture and Regional Planning for the extensive research that provided the foundation for this summary. Special thanks are given to the University of Massachusetts faculty who advised on this project including: Assistant Professor Elisabeth Hamin, Professor Dean Cardasis, Michael DiPasquale of the Community Planners Training Collaborative and Graduate Assistant, Nedim Kemer. The author would also like to thank the following individuals for providing review and insight throughout this project and to drafts of this report: Susy Affleck Childs, Administrator, Town of Medway Planning Board; Elisabeth Hamin, Assistant Professor, University of Massachusetts Amherst, Department of Landscape Architecture and Regional Planning; Kathy Joubert, Town Planner, Town of Northborough; Jody Kablack, AICP, Director of Planning and Community Development, Town of Sudbury; Mark Kablack, M.A. Kablack & Associates, P.C.; David LaPointe, RLA, Beals and Thomas, Inc.; Lauren Rosenzwieg, Selectwoman, Town of Acton; Senator Pam Resor; Andy Rodenhiser, Chairman, Town of Medway Planning Board; Ron Roux, Owner, Hallmark Companies; Beth Rust, Community Housing Specialist, Town of Sudbury; Glenn Trindade, Selectman, Town of Medway; Chris Vericker, Vice President, Middlesex Savings Bank; and Ralph Wilmer, AICP, Senior Planner and Project Manager, Vanasse, Hangen, Brustlin, Inc. -
The Greater Lowell Trauma Resource Directory
The Greater Lowell Trauma Resource Directory August 2019 Created by Merrimack Valley Trauma Services and funded by the Commonwealth Preschool Partnership Initiative P a g e | 2 Alternative House P.O. Box 2100, Lowell, MA 01853 978-937-5777 Hotline: 888-291-6228 alternative-house.org Comprehensive, free, and confidential domestic violence services for the Greater Lowell community. Twenty-four hour hotline. Emergency confidential shelter for victims of domestic violence, community- based support groups, education and training, legal advocacy and support to assist in the restraining order process, and connections to local resources for survivors (e.g., immigration resources, relocation, safety planning, and finding shelter). Mary Rita's House is a two-year residential program for survivors of domestic violence that provides assistance with enrolling in job training, GED classes, and/or classes at local colleges, permanent housing searches, specialized job certification programs, and support to help participants gain the skills to enter the job market and live a life free from violence. Center for Hope and Healing 21 George Street, Suite 400, Lowell, MA 01852 978-452-7721 chhinc.org Founded in 1976 by a group of physicians, social workers and students, who came together out of a concern for the number of rapes occurring in Lowell. CHH is committed to eradicating sexual violence in Lowell and the surrounding communities. Provides Individual and group counseling, legal and medical advocacy, resources and referrals, and a 24-hour crisis hotline for survivors of sexual assault and their loved ones. All services are free and confidential, regardless of insurance, income, citizenship, or any other barriers. -

495/Metrowest Biotech Companies
LIFE SCIENCES IN 495/METROWEST: EXISTING IMPORTANCE & FUTURE POSSIBILITY February 15, 2018 Special thanks to our event host: •Any one of the branches of science concerned with the structure and Definition of Life behavior of living organisms, such as Science biology, botany, zoology, physiology, or biochemistry. 1993 - Governor Weld’s Choosing to Compete: A Statewide Strategy for Job Creation and Economic Definition of Life Growth Science 2002 – Governor Swift’s Toward a New Prosperity: for Massachusetts Building Regional Competitiveness Across the Commonwealth Economic 2011 – Governor Patrick’s Choosing to Compete in Development the 21st Century: An Economic Development Policy and Strategic Plan for the Commonwealth of Massachusetts 2015 – Governor Baker’s Opportunities for All: The Baker-Polito Strategy & Plan for Making Massachusetts Great Everywhere Perceptions of Massachusetts in Life Sciences • “The Commonwealth is now arguably the biotech capital of the world.” – Rafael Reif, President of M.I.T. • “Conscious of its role as the world’s life sciences epicenter, the Greater Boston area leads by example. The Massachusetts Life Sciences Center … offers the nation’s most comprehensive set of incentives and programs, and it helps to create jobs and support industry advancement.” • “Human capital is what keeps the wheels turning at life sciences companies, both big and small, and it is vital to growth” 495/MetroWest: Affordability & Access • Commercial real estate average a 37% discount when compared to Boston • Availability of skilled -

Land-Use Planning in the Doldrums: Growth Management in Massachusetts’ I-495 Region
LAND-USE PLANNING Land-Use Planning in the Doldrums: Growth Management in Massachusetts’ I-495 Region By Christina Rosan and Lawrence Susskind (Massachusetts Institute of Technology) September 2007 RAPPAPORT Institute for Greater Boston Kennedy School of Government, Harvard University Land-Use Planning in the Doldrums Authors Christina Rosan is currently a Postdoctoral Fellow in urban planning at the Massachusetts Institute of Technology (MIT). She received her Ph.D. in Urban and Regional Planning from MIT in September 2007. Her dissertation compares metropolitan governance and local land-use planning in Boston, Denver, and Portland. Christina was a Rappaport Public Policy Fellow in the Summer of 2005. Lawrence Susskind is Ford Professor of Urban and Environmental Planning at the Massachusetts Institute of Technology, director of the Public Disputes Program at Harvard Law School, and founder of the Consensus Building Institute. Acknowledgements The authors wish to thank the Rappaport Institute for Greater Boston for funding this research. In particular, we would like to thank David Luberoff, Executive Director of the Rappaport Institute for Greater Boston, for all his edits and comments to this work. We also would like to thank Phil Primack, Martha Rounds, and Molly Wilson-Murphy for their editing assistance. We want to express our appreciation to David Fairman and Ona Ferguson at the Consensus Building Institute, and Marina Psaros, a former MIT student, for all their help in organizing this research effort and preparing the case studies. We also want to acknowledge former and current MIT students, Pankaj Kumar, Jiawen Yang, and Ye Ding, who helped conduct some of the initial research for the cases.