Download Them
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Multicentricity of Breast Cancer
/ Int Soc Plastination, Vol 3:8-14, 1989 8 MULTICENTRICITY OF BREAST CANCER. RESULTS OF A STUDY USING SHEET PLASTINATION OF MASTECTOMY SPECIMENS Axel Müller, Andreas Guhr, Wolfgang Leucht (Frauenklinik) Gunther von Hagens (Anatomisches Institut) University of Heidelberg, 6900 Heidelberg 1, West Germany INTRODUCTION These questions may only be answered after complete histological Carcinomas of the female breast examination of breasts from total are judged to be mostly multicentric mastectomy patients suited for BCTh. (Fisher et al., 1975; Gallager and Martin, 1969; Morgenstern et al., Guhr and co-workers (1987) 1975) and only total breast removal described sheet plastination as the was recommended until about 1960. best method for fast, complete Since then, breast conserving therapy histological study of mastectomy (BCTh), i.e. surgical excision of the specimens. In the present study tumor in combination with radiotherapy using sheet plastination, frequency of the remaining breast, has been and topographical distribution of performed in selected patients. The tumor foci, which remain in the breast survival rate of BCTh patients is not after BCTh, were evaluated in 131 significantly different when compared patients. to total breast removal, and the local recurrence rate is about 4-8% in five years (Fisher and Wolmark, 1986; MATERIALS AND METHODS Veronesi et al., 1986). In 70-90% of local failures following BCTh, Between 1978 and 1981, modified carcinoma growth was found at the radical mastectomies with full primary tumor site. Four hypotheses axillary dissections were carried out may serve as possible reasons: for invasive carcinomas in 695 patients at the Division of Gynecology (1) Multicentricity is lower than and Obstetrics, University of claimed in the literature. -

View/Open: ETD Quigley.Pdf
TÇtàÉÅ|vtÄ \wxÇà|àç _xäxÄá Éy \wxÇà|àç Tààtv{xw àÉ cÜxáxÜäxw [âÅtÇ exÅt|Çá A Thesis submitted to the Faculty of the Graduate School of Arts and Sciences of Georgetown University in partial fulfillment of the requirements for the degree of Master of Arts in Communication, Culture & Technology by Christine Quigley, B.A., B.F.A. Washington, D.C. April 20, 2007 © 2007 by Christine Quigley ii TuáàÜtvà Head slice on table. Max Aguilera-Hellweg (1994). Sagittsl section, part of a series demonstrating the anatomy of the head, prepared for the Mutter Muaeum by Dr. Joseph P. Tunis (1866-1936), 1910 (www.blastbooks.com). When a human body part is removed and preserved after death, what kinds of identity remain attached to it? There are the extremes of complete anonymity and the named remains of a famous or infamous person, but there are many shades of gray in between. Is the specimen that of a known individual or recognizable only as a race and gender? What reason would someone have to designate the preservation of his remains and ensure that the narrative of his life stays permanently attached? Does a very personal part, like face or skin, commemorate the life of that particular body or can it still be used to represent universal human anatomy? The answers are in part determined by whether the donor wanted his or her identity associated with the specimen. I examine the gradations of identity as represented by three museum objects in three different time periods. The first is the autobiography of a nineteenth-century criminal bound at his request in iii his skin (at the Boston Athenaeum). -

To Download the Entire Volume 29 Issue 2 As
The Journal of Plastination The official publication of the International Society for Plastination ISSN 2311-7761 IN THIS ISSUE: S10 Plastination Technique for Preservation of Parasites – p5 Plastination Applied to The Conservation of Cultural Heritage – p11 The Challenges of Plastinating a Blue Whale (Balaenoptera musculus) Heart – p22 Rehabilitation of Plastinated Anatomical Prosections Using Silicone Adhesive and Pre-Cured S10/S3-Impregnated Fascia and Muscle – p30 Abstracts Presented at the 12th Interim Meeting of the ISP in Durban, South Africa – p37 Preview of ISP 2018, Dalian – p65 Volume 29 (2); December 2017 The Journal of Plastination ISSN 2311-7761 ISSN 2311-777X online The official publication of the International Society for Plastination Editorial Board: Rafael Latorre Philip J. Adds Murcia, Spain Editor-in-Chief Institute of Medical and Biomedical Education Scott Lozanoff (Anatomy) Honolulu, HI USA St. George’s, University of London London, UK Ameed Raoof. Ann Arbor, MI USA Robert W. Henry Associate Editor Mircea-Constantin Sora Department of Comparative Medicine Vienna, Austria College of Veterinary Medicine Hong Jin Sui Knoxville, Tennessee, USA Dalian, China Selcuk Tunali Carlos Baptista Assistant Editor Toledo, OH USA Department of Anatomy Hacettepe University Faculty of Medicine Ankara, Turkey Executive Committee: Rafael Latorre, President Dmitry Starchik, Vice-President Selcuk Tunali, Secretary Carlos Baptista, Treasurer Instructions for Authors Manuscripts and figures intended for publication in The Journal of Plastination should be sent via e-mail attachment to: [email protected]. Manuscript preparation guidelines are on the last two pages of this issue. On the Cover: Royal Ontario Museum Exhibit: Dilated, dissected, cured, plastinated blue whale heart. -

DOCUMENTING LONG-TERM CARE, INCAPACITY, and END-OF-LIFE DECISIONS1 by Jill A
DOCUMENTING LONG-TERM CARE, INCAPACITY, AND END-OF-LIFE DECISIONS1 By Jill A. Snyder, Esq.2 Law Office of Jill A. Snyder, LLC www.snyder-law.net I. Long-Term Care Options and Planning in a Nutshell3 A. Federal Programs and Public Housing: Federal government programs exist that provide both rental and mortgage assistance to the elderly.4 Some of the most-widely used programs include: 1. Section 202 Supportive Housing for the Elderly is a Housing and Urban Development (“HUD”)-administered program that provides supportive housing for very low-income persons age 62 and older. This program gives capital advances to non-profit organizations to construct or rehabilitate structures that will serve as supportive housing. Support services include activities such as cleaning, cooking, and transportation. Capital advances do not need to be repaid so long as supportive housing remains available for at least forty years. This program also includes funding to cover the difference between what the renter can pay and the cost of operating the project. To be eligible for residency in Section 202 housing, one occupant must be 62 years or older with a household income at or below 50% of the area median income. 2. Section 8 Housing Choice Voucher Program is a federally funded program that distributes vouchers through state, regional, and local housing agencies. Section 8 assists both renters and homeowners 1 Presented on behalf of the National Business Institute on December 6, 2012, in Baltimore, Maryland. 2 I would like to thank my Legal Assistant, Kristie Ehlers, for her assistance in preparing these materials. -

A Study on the Preservation of Exhumed Mummies by Plastination
20- J lnt Soc Plastination Vol 13, No 1: 20-22, 1998 A Study on the Preservation of Exhumed Mummies by Plastination Zheng Tianzhong, You Xuegui, Liu Jingren, Zhu Kerming Department of Anatomy, Shanghai Medical University, Shanghai, P. R. China. (received March 7, accepted April 14, 1998) Key Words: Su-Yi Chinese Silicone, Archeology, Paleopathology Abstract Due to the great importance of mummies for archeological research, methods have to be developed to preserve these specimens. Two preserved mummies (died 410 and 380 years ago) were exhumed and plastinated to avoid deterioration from exposure. They were first re-fixed with formalin and dehydrated at room temperature in a graded series of acetone solutions. The corpses were then pre- impregnated, force impregnated with silicone and subsequently cured all at room temperature. Histological studies were performed before and after plastination on pieces of lung, liver, kidney, heart, spleen and skin. Plastination improved the color and flexibility of the mummies and will permanently preserve them. Introduction of plastination of an archaeological human specimen has been reported (Wade and Lyons, 1995). In our laboratory, we suc- Mummies have an invaluable value for academic re- cessfully plastinated two ancient (400 years old) Chinese search of our national culture. Extensive research studies are corpses, through fixation, dehydration, pre-impregnation and conducted to develop methods for the preservation of these forced impregnation (Zheng et al., 1998). corpses. There are two types of mummies: dry type and wet type. For the dry type most scientists prefer to keep them in Materials and Methods a dry atmosphere, but for the wet type, scientists must dry them before keeping them in dry conditions or just immerse Case 1: ancient corpse discovered near Zhengjaing in them into bath of preservative solutions. -

95 CHAPTER 5 Looking at Science, Looking at You! the Feminist Re-Visions of Nature
CHAPTER 5 Looking at Science, Looking at You! The Feminist Re-visions of Nature (Brain and Genes) Cecilia Åsberg Vision has often been a central concern of feminist studies of science, medi- cine and technology. In cultural or social feminist analysis, the male gaze and the ways in which technoscience1 accommodates, and in effect organizes the watching of women, has been an important part of the feminist interrogation of the gender and power relations that produce the subjects and the objects of science.2 This attention is due to the intimate, and power-saturated, merge of processes of seeing and processes of knowing. Inherent in the notion of vision, there is always a politics to ways of seeing, ordering and observing, of organising the knowledge of the world. Historically, this can be exemplified by the eighteen-century Swedish “father” of biological classification, Linnaeus. Taking a leap away from Christian assumptions, Linnaeus placed human beings in a taxonomic order of nature together with other animals.3 In his large-scale vision, he located humans together with primates in the order of Homo sapiens, as Donna Haraway4 so eloquently describes it in her ground-breaking book Primate Visions. And as the “father” of a specific discourse on nature, one that was not understood biologically but rather representationally, and still within a highly Christian framework, he referred to himself as the second Adam, as the “eye” of God. As the second Adam, Linnaeus could give true representations and true names to nature’s creatures and in so doing also restore the purity of name-giving lost by the first, biblical Adam’s sin. -

Tracing the Body in Body Worlds, the Anatomical Exhibition of Real Human Bodies
ANATOMY OF SPECTATORSHIP: TRACING THE BODY IN BODY WORLDS, THE ANATOMICAL EXHIBITION OF REAL HUMAN BODIES by Rebecca Scott Bachelor of Arts, Simon Fraser University, 2005 THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF ARTS In the School of Communication © Rebecca Scott 2008 SIMON FRASER UNIVERSITY Summer 2008 All rights reserved. This work may not be reproduced in whole or in part, by photocopy or other means, without permission of the author. APPROVAL Name: Rebecca Scott Degree: MA Titles: Anatomy of Spectatorship: Tracing the Body in Body Worlds, the Anatomical Exhibition of Real Human Bodies Examining Committee: Chair: Dr. Peter Chow-White Assistant Professor, School of Communication Dr. Kirsten McAllister Assistant Professor School of Communication Dr. Zoe Druick Associate Professor School of Communication Dr Kimberly Sawchuk Associate Professor Department of Communication Studies Concordia University Date: ii SIMON FRASER UNIVERSITY LIBRARY Declaration of Partial Copyright Licence The author, whose copyright is declared on the title page of this work, has granted to Simon Fraser University the right to lend this thesis, project or extended essay to users of the Simon Fraser University Library, and to make partial or single copies only for such users or in response to a request from the library of any other university, or other educational institution, on its own behalf or for one of its users The author has further granted permission to Simon Fraser University to keep or make a digital copy for use in its circulating collection (currently available to the pUblic at the "Institutional Repository" link of the SFU Library website <www.lib.sfu.ca> at: <http://ir.lib.sfu.ca/handle/1892/112>) and, without changing the content, to translate the thesis/project or extended essays, if technically possible, to any medium or format for the purpose of preservation of the digital work. -

Advanced Sectioned Images of a Cadaver Head with Voxel Size Of
J Korean Med Sci. 2019 Sep 2;34(34):e218 https://doi.org/10.3346/jkms.2019.34.e218 eISSN 1598-6357·pISSN 1011-8934 Original Article Advanced Sectioned Images of a Cadaver Basic Medical Sciences Head with Voxel Size of 0.04 mm Beom Sun Chung ,1 Miran Han ,2 Donghwan Har ,3 and Jin Seo Park 4 1Department of Anatomy, Ajou University School of Medicine, Suwon, Korea 2Department of Radiology, Ajou University School of Medicine, Suwon, Korea 3College of ICT Engineering, Chung Ang University, Seoul, Korea 4Department of Anatomy, Dongguk University School of Medicine, Gyeongju, Korea Received: Jun 14, 2019 Accepted: Jul 22, 2019 ABSTRACT Address for Correspondence: Background: The sectioned images of a cadaver head made from the Visible Korean project Jin Seo Park, PhD have been used for research and educational purposes. However, the image resolution Department of Anatomy, Dongguk University is insufficient to observe detailed structures suitable for experts. In this study, advanced School of Medicine, 87 Dongdae-ro, Gyeongju sectioned images with higher resolution were produced for the identification of more 38067, Republic of Korea. E-mail: [email protected] detailed structures. Methods: The head of a donated female cadaver was scanned for 3 Tesla magnetic resonance © 2019 The Korean Academy of Medical images and diffusion tensor images (DTIs). After the head was frozen, the head was Sciences. sectioned serially at 0.04-mm intervals and photographed repeatedly using a digital camera. This is an Open Access article distributed Results: On the resulting 4,000 sectioned images (intervals and pixel size, 0.04 mm3; color under the terms of the Creative Commons Attribution Non-Commercial License (https:// depth, 48 bits color; a file size, 288 Mbytes), minute brain structures, which can be observed creativecommons.org/licenses/by-nc/4.0/) not on previous sectioned images but on microscopic slides, were observed. -

The Virtual Hip: an Anatomically Accurate Finite Element Model Based on the Visible Human Dataset
University of South Florida Scholar Commons Graduate Theses and Dissertations Graduate School 10-4-2010 The Virtual Hip: An Anatomically Accurate Finite Element Model Based on the Visible Human Dataset Jonathan M. Ford University of South Florida Follow this and additional works at: https://scholarcommons.usf.edu/etd Part of the American Studies Commons, Biomedical Engineering and Bioengineering Commons, and the Chemical Engineering Commons Scholar Commons Citation Ford, Jonathan M., "The Virtual Hip: An Anatomically Accurate Finite Element Model Based on the Visible Human Dataset" (2010). Graduate Theses and Dissertations. https://scholarcommons.usf.edu/etd/3451 This Thesis is brought to you for free and open access by the Graduate School at Scholar Commons. It has been accepted for inclusion in Graduate Theses and Dissertations by an authorized administrator of Scholar Commons. For more information, please contact [email protected]. The Virtual Hip: An Anatomically Accurate Finite Element Model Based on the Visible Human Dataset by Jonathan M. Ford A thesis submitted in partial fulfillment of the requirements for the degree of Master of Science in Biomedical Engineering Department of Chemical and Biomedical Engineering College of Engineering University of South Florida Co-Major Professor: Don Hilbelink, Ph.D. Co-Major Professor: Les Piegl, Ph.D. William Lee III, Ph.D., P.E. Karl Muffly, Ph.D. Date of Approval: October 4, 2010 Keywords: Quantitative Anatomy, Gluteus Minimus, COMSOL, Model Error Copyright © 2010, Jonathan M. Ford DEDICATION I would like to dedicate this thesis to “B” and Vegas. They pushed me to reach for the stars and when I lost my direction they were the ones to point me the way. -

BODY WORLDS Family Guide
FAMILYGUIDE CONTENTS Planning your visit 3 FAQ 4 Q&A with kids 9 What is Plastination 11 WELCOME—a letter from BODY WORLDS 13 EXHIBITION OVERVIEW 14 The Locomotive System 15 The Nervous System 16 The Respiratory System 17 The Cardiovascular System 18 The Digestive System 19 Embryonic & Fetal Development 20 Post-visit activities 21 Discussion questions 23 Additional resources 24 This material is protected under copyright laws and may not be reproduced in any manner without the express written permission of the Institute for Plastination. MARCH, 2017 US FAMILYGUIDE 2 PLANNING YOUR VISIT BEFORE + Read the note to parents and frequently asked questions in this family guide. + Visit the BODY WORLDS website: www.bodyworlds.com. + Discuss the visit with your children and explain what they are going to see and why. DURING + Consult this Family Guide for an overview of the exhibit. + Seek out the Museum Hosts for answers to your questions about the exhibition. AFTER + Discuss the experience with your family using some of the discussion questions included in this guide as prompts. + Try some of the Post-Visit Activities. + Visit some of the websites listed in the additional resources section. FAMILYGUIDE 3 FREQUENTLY ASKED QUESTIONS What is BODY WORLDS? How do the various BODY WORLDS The exhibition BODY WORLDS, internationally known exhibitions that are being shown differ as BODY WORLDS: The Original Exhibition of Real from each other? Human Bodies, is the first exhibition of its kind to While all of the BODY WORLDS exhibitions focus inform the visitor about anatomy, physiology, and on general anatomy revealed through Plastination, health by viewing real human bodies. -
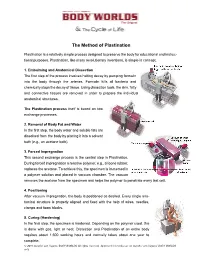
The Method of Plastination
The Method of Plastination Plastination is a relatively simple process designed to preserve the body for educational and instruc- tional purposes. Plastination, like many revolutionary inventions, is simple in concept: 1. Embalming and Anatomical Dissection The first step of the process involves halting decay by pumping formalin into the body through the arteries. Formalin kills all bacteria and chemically stops the decay of tissue. Using dissection tools, the skin, fatty and connective tissues are removed in order to prepare the individual anatomical structures. The Plastination process itself is based on two exchange processes. 2. Removal of Body Fat and Water In the first step, the body water and soluble fats are dissolved from the body by placing it into a solvent bath (e.g., an acetone bath). 3. Forced Impregnation This second exchange process is the central step in Plastination. During forced impregnation a reactive polymer, e.g., silicone rubber, replaces the acetone. To achieve this, the specimen is immersed in a polymer solution and placed in vacuum chamber. The vacuum removes the acetone from the specimen and helps the polymer to penetrate every last cell. 4. Positioning After vacuum impregnation, the body is positioned as desired. Every single ana- tomical structure is properly aligned and fixed with the help of wires, needles, clamps and foam blocks. 5. Curing (Hardening) In the final step, the specimen is hardened. Depending on the polymer used, this is done with gas, light or heat. Dissection and Plastination of an entire body requires about 1,500 working hours and normally takes about one year to complete. -
Educator Guide Grades 4-8
EDUCATOR GUIDE GRADES 4-8 Take one large dose of enlightenment during a visit to the world debut of BODY WORLDS RX. Real human bodies show you details of today’s common diseases and the inner workings of your anatomy. Be inspired and empowered to take steps toward a healthier life. MCWANE SCIENCE CENTER PRESENTED BY MCWANE.ORG Contents Welcome Letter .................................................................................................. 3 Mission of the Exhibitions ................................................................................... 4 Note to Educators ............................................................................................... 5 Planning Your Visit .............................................................................................. 6 Permission Form ................................................................................................. 7 Chaperone Responosibilites ................................................................................. 8 Frequently Asked Questions ................................................................................. 9 ACOSS Standerds ..................................................................................................... 12 Classroom Activities ............................................................................................ 13 Exhibition Overview including Human Facts .......................................................... 26 Additional Resources .........................................................................................