Multicentricity of Breast Cancer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

View/Open: ETD Quigley.Pdf
TÇtàÉÅ|vtÄ \wxÇà|àç _xäxÄá Éy \wxÇà|àç Tààtv{xw àÉ cÜxáxÜäxw [âÅtÇ exÅt|Çá A Thesis submitted to the Faculty of the Graduate School of Arts and Sciences of Georgetown University in partial fulfillment of the requirements for the degree of Master of Arts in Communication, Culture & Technology by Christine Quigley, B.A., B.F.A. Washington, D.C. April 20, 2007 © 2007 by Christine Quigley ii TuáàÜtvà Head slice on table. Max Aguilera-Hellweg (1994). Sagittsl section, part of a series demonstrating the anatomy of the head, prepared for the Mutter Muaeum by Dr. Joseph P. Tunis (1866-1936), 1910 (www.blastbooks.com). When a human body part is removed and preserved after death, what kinds of identity remain attached to it? There are the extremes of complete anonymity and the named remains of a famous or infamous person, but there are many shades of gray in between. Is the specimen that of a known individual or recognizable only as a race and gender? What reason would someone have to designate the preservation of his remains and ensure that the narrative of his life stays permanently attached? Does a very personal part, like face or skin, commemorate the life of that particular body or can it still be used to represent universal human anatomy? The answers are in part determined by whether the donor wanted his or her identity associated with the specimen. I examine the gradations of identity as represented by three museum objects in three different time periods. The first is the autobiography of a nineteenth-century criminal bound at his request in iii his skin (at the Boston Athenaeum). -

To Download the Entire Volume 29 Issue 2 As
The Journal of Plastination The official publication of the International Society for Plastination ISSN 2311-7761 IN THIS ISSUE: S10 Plastination Technique for Preservation of Parasites – p5 Plastination Applied to The Conservation of Cultural Heritage – p11 The Challenges of Plastinating a Blue Whale (Balaenoptera musculus) Heart – p22 Rehabilitation of Plastinated Anatomical Prosections Using Silicone Adhesive and Pre-Cured S10/S3-Impregnated Fascia and Muscle – p30 Abstracts Presented at the 12th Interim Meeting of the ISP in Durban, South Africa – p37 Preview of ISP 2018, Dalian – p65 Volume 29 (2); December 2017 The Journal of Plastination ISSN 2311-7761 ISSN 2311-777X online The official publication of the International Society for Plastination Editorial Board: Rafael Latorre Philip J. Adds Murcia, Spain Editor-in-Chief Institute of Medical and Biomedical Education Scott Lozanoff (Anatomy) Honolulu, HI USA St. George’s, University of London London, UK Ameed Raoof. Ann Arbor, MI USA Robert W. Henry Associate Editor Mircea-Constantin Sora Department of Comparative Medicine Vienna, Austria College of Veterinary Medicine Hong Jin Sui Knoxville, Tennessee, USA Dalian, China Selcuk Tunali Carlos Baptista Assistant Editor Toledo, OH USA Department of Anatomy Hacettepe University Faculty of Medicine Ankara, Turkey Executive Committee: Rafael Latorre, President Dmitry Starchik, Vice-President Selcuk Tunali, Secretary Carlos Baptista, Treasurer Instructions for Authors Manuscripts and figures intended for publication in The Journal of Plastination should be sent via e-mail attachment to: [email protected]. Manuscript preparation guidelines are on the last two pages of this issue. On the Cover: Royal Ontario Museum Exhibit: Dilated, dissected, cured, plastinated blue whale heart. -

DOCUMENTING LONG-TERM CARE, INCAPACITY, and END-OF-LIFE DECISIONS1 by Jill A
DOCUMENTING LONG-TERM CARE, INCAPACITY, AND END-OF-LIFE DECISIONS1 By Jill A. Snyder, Esq.2 Law Office of Jill A. Snyder, LLC www.snyder-law.net I. Long-Term Care Options and Planning in a Nutshell3 A. Federal Programs and Public Housing: Federal government programs exist that provide both rental and mortgage assistance to the elderly.4 Some of the most-widely used programs include: 1. Section 202 Supportive Housing for the Elderly is a Housing and Urban Development (“HUD”)-administered program that provides supportive housing for very low-income persons age 62 and older. This program gives capital advances to non-profit organizations to construct or rehabilitate structures that will serve as supportive housing. Support services include activities such as cleaning, cooking, and transportation. Capital advances do not need to be repaid so long as supportive housing remains available for at least forty years. This program also includes funding to cover the difference between what the renter can pay and the cost of operating the project. To be eligible for residency in Section 202 housing, one occupant must be 62 years or older with a household income at or below 50% of the area median income. 2. Section 8 Housing Choice Voucher Program is a federally funded program that distributes vouchers through state, regional, and local housing agencies. Section 8 assists both renters and homeowners 1 Presented on behalf of the National Business Institute on December 6, 2012, in Baltimore, Maryland. 2 I would like to thank my Legal Assistant, Kristie Ehlers, for her assistance in preparing these materials. -

A Study on the Preservation of Exhumed Mummies by Plastination
20- J lnt Soc Plastination Vol 13, No 1: 20-22, 1998 A Study on the Preservation of Exhumed Mummies by Plastination Zheng Tianzhong, You Xuegui, Liu Jingren, Zhu Kerming Department of Anatomy, Shanghai Medical University, Shanghai, P. R. China. (received March 7, accepted April 14, 1998) Key Words: Su-Yi Chinese Silicone, Archeology, Paleopathology Abstract Due to the great importance of mummies for archeological research, methods have to be developed to preserve these specimens. Two preserved mummies (died 410 and 380 years ago) were exhumed and plastinated to avoid deterioration from exposure. They were first re-fixed with formalin and dehydrated at room temperature in a graded series of acetone solutions. The corpses were then pre- impregnated, force impregnated with silicone and subsequently cured all at room temperature. Histological studies were performed before and after plastination on pieces of lung, liver, kidney, heart, spleen and skin. Plastination improved the color and flexibility of the mummies and will permanently preserve them. Introduction of plastination of an archaeological human specimen has been reported (Wade and Lyons, 1995). In our laboratory, we suc- Mummies have an invaluable value for academic re- cessfully plastinated two ancient (400 years old) Chinese search of our national culture. Extensive research studies are corpses, through fixation, dehydration, pre-impregnation and conducted to develop methods for the preservation of these forced impregnation (Zheng et al., 1998). corpses. There are two types of mummies: dry type and wet type. For the dry type most scientists prefer to keep them in Materials and Methods a dry atmosphere, but for the wet type, scientists must dry them before keeping them in dry conditions or just immerse Case 1: ancient corpse discovered near Zhengjaing in them into bath of preservative solutions. -

Tracing the Body in Body Worlds, the Anatomical Exhibition of Real Human Bodies
ANATOMY OF SPECTATORSHIP: TRACING THE BODY IN BODY WORLDS, THE ANATOMICAL EXHIBITION OF REAL HUMAN BODIES by Rebecca Scott Bachelor of Arts, Simon Fraser University, 2005 THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF ARTS In the School of Communication © Rebecca Scott 2008 SIMON FRASER UNIVERSITY Summer 2008 All rights reserved. This work may not be reproduced in whole or in part, by photocopy or other means, without permission of the author. APPROVAL Name: Rebecca Scott Degree: MA Titles: Anatomy of Spectatorship: Tracing the Body in Body Worlds, the Anatomical Exhibition of Real Human Bodies Examining Committee: Chair: Dr. Peter Chow-White Assistant Professor, School of Communication Dr. Kirsten McAllister Assistant Professor School of Communication Dr. Zoe Druick Associate Professor School of Communication Dr Kimberly Sawchuk Associate Professor Department of Communication Studies Concordia University Date: ii SIMON FRASER UNIVERSITY LIBRARY Declaration of Partial Copyright Licence The author, whose copyright is declared on the title page of this work, has granted to Simon Fraser University the right to lend this thesis, project or extended essay to users of the Simon Fraser University Library, and to make partial or single copies only for such users or in response to a request from the library of any other university, or other educational institution, on its own behalf or for one of its users The author has further granted permission to Simon Fraser University to keep or make a digital copy for use in its circulating collection (currently available to the pUblic at the "Institutional Repository" link of the SFU Library website <www.lib.sfu.ca> at: <http://ir.lib.sfu.ca/handle/1892/112>) and, without changing the content, to translate the thesis/project or extended essays, if technically possible, to any medium or format for the purpose of preservation of the digital work. -

BODY WORLDS Family Guide
FAMILYGUIDE CONTENTS Planning your visit 3 FAQ 4 Q&A with kids 9 What is Plastination 11 WELCOME—a letter from BODY WORLDS 13 EXHIBITION OVERVIEW 14 The Locomotive System 15 The Nervous System 16 The Respiratory System 17 The Cardiovascular System 18 The Digestive System 19 Embryonic & Fetal Development 20 Post-visit activities 21 Discussion questions 23 Additional resources 24 This material is protected under copyright laws and may not be reproduced in any manner without the express written permission of the Institute for Plastination. MARCH, 2017 US FAMILYGUIDE 2 PLANNING YOUR VISIT BEFORE + Read the note to parents and frequently asked questions in this family guide. + Visit the BODY WORLDS website: www.bodyworlds.com. + Discuss the visit with your children and explain what they are going to see and why. DURING + Consult this Family Guide for an overview of the exhibit. + Seek out the Museum Hosts for answers to your questions about the exhibition. AFTER + Discuss the experience with your family using some of the discussion questions included in this guide as prompts. + Try some of the Post-Visit Activities. + Visit some of the websites listed in the additional resources section. FAMILYGUIDE 3 FREQUENTLY ASKED QUESTIONS What is BODY WORLDS? How do the various BODY WORLDS The exhibition BODY WORLDS, internationally known exhibitions that are being shown differ as BODY WORLDS: The Original Exhibition of Real from each other? Human Bodies, is the first exhibition of its kind to While all of the BODY WORLDS exhibitions focus inform the visitor about anatomy, physiology, and on general anatomy revealed through Plastination, health by viewing real human bodies. -
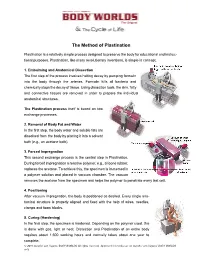
The Method of Plastination
The Method of Plastination Plastination is a relatively simple process designed to preserve the body for educational and instruc- tional purposes. Plastination, like many revolutionary inventions, is simple in concept: 1. Embalming and Anatomical Dissection The first step of the process involves halting decay by pumping formalin into the body through the arteries. Formalin kills all bacteria and chemically stops the decay of tissue. Using dissection tools, the skin, fatty and connective tissues are removed in order to prepare the individual anatomical structures. The Plastination process itself is based on two exchange processes. 2. Removal of Body Fat and Water In the first step, the body water and soluble fats are dissolved from the body by placing it into a solvent bath (e.g., an acetone bath). 3. Forced Impregnation This second exchange process is the central step in Plastination. During forced impregnation a reactive polymer, e.g., silicone rubber, replaces the acetone. To achieve this, the specimen is immersed in a polymer solution and placed in vacuum chamber. The vacuum removes the acetone from the specimen and helps the polymer to penetrate every last cell. 4. Positioning After vacuum impregnation, the body is positioned as desired. Every single ana- tomical structure is properly aligned and fixed with the help of wires, needles, clamps and foam blocks. 5. Curing (Hardening) In the final step, the specimen is hardened. Depending on the polymer used, this is done with gas, light or heat. Dissection and Plastination of an entire body requires about 1,500 working hours and normally takes about one year to complete. -
Educator Guide Grades 4-8
EDUCATOR GUIDE GRADES 4-8 Take one large dose of enlightenment during a visit to the world debut of BODY WORLDS RX. Real human bodies show you details of today’s common diseases and the inner workings of your anatomy. Be inspired and empowered to take steps toward a healthier life. MCWANE SCIENCE CENTER PRESENTED BY MCWANE.ORG Contents Welcome Letter .................................................................................................. 3 Mission of the Exhibitions ................................................................................... 4 Note to Educators ............................................................................................... 5 Planning Your Visit .............................................................................................. 6 Permission Form ................................................................................................. 7 Chaperone Responosibilites ................................................................................. 8 Frequently Asked Questions ................................................................................. 9 ACOSS Standerds ..................................................................................................... 12 Classroom Activities ............................................................................................ 13 Exhibition Overview including Human Facts .......................................................... 26 Additional Resources ......................................................................................... -

The Use of Animals in Higher Education
THE USE OF P R O B L E M S, A L T E R N A T I V E S , & RECOMMENDA T I O N S HUMANE SOCIETY PR E S S by Jonathan Balcombe, Ph.D. PUBLIC PO L I C Y SE R I E S Public Policy Series THE USE OF An i m a l s IN Higher Ed u c a t i o n P R O B L E M S, A L T E R N A T I V E S , & RECOMMENDA T I O N S by Jonathan Balcombe, Ph.D. Humane Society Press an affiliate of Jonathan Balcombe, Ph.D., has been associate director for education in the Animal Res e a r ch Issues section of The Humane Society of the United States since 1993. Born in England and raised in New Zealand and Canada, Dr . Balcombe studied biology at York University in Tor onto before obtaining his masters of science degree from Carleton University in Ottawa and his Ph.D. in ethology at the University of Tennessee. Ack n ow l e d g m e n t s The author wishes to thank Andrew Rowan, Martin Stephens, Gretchen Yost, Marilyn Balcombe, and Francine Dolins for reviewing and commenting on earlier versions of this monograph. Leslie Adams, Kathleen Conlee, Lori Do n l e y , Adrienne Gleason, Daniel Kos s o w , and Brandy Richardson helped with various aspects of its research and preparation. Copyright © 2000 by The Humane Society of the United States. -

Literary Plastination: from Body’S Objectification to the Ontological Representation of Death, Differences Between Sick-Literature and Tales by Amateur Writers
LITERARY PLASTINATION: FROM BODY’S OBJECTIFICATION TO THE ONTOLOGICAL REPRESENTATION OF DEATH, DIFFERENCES BETWEEN SICK-LITERATURE AND TALES BY AMATEUR WRITERS INES TESTONI GIULIA PARISE UNIVERSITY OF PADOVA EMILIO PAOLO VISINTIN UNIVERSITY OF LAUSANNE ADRIANO ZAMPERINI LUCIA RONCONI UNIVERSITY OF PADOVA This article presents a qualitative analysis of published and unpublished texts, aimed to understand a new narrative phenomenon named “sick-lit.” This is a genre of stories, written by professional novel- ists, rooted in disease, self-harm, suicide, sufferance from violence, death, and dying. In the Internet it has been considered as a trivialization of serious issues and even potentially encouraging readers to harm themselves. Our hypothesis is that this negative judgment is based on the ontological representa- tion of death and the objectification of the body depicted in these stories. In order to inquire into this possibility and to compare this anomalous form of story-telling with another kind of narration reflect- ing the wider common sensibility, a qualitative analysis was realized on six sick-lit novels (SLNs) and 21 unpublished tales written by amateur writers (AWTs). The results confirm the hypothesis: the SLNs represent death also as an absolute annihilation and the body is always reified through medical lan- guage, while the AWTs represent death only as a passage or reincarnation and the description of the de- teriorated body is minimal. Key words: Sick-lit; Ontological representation of death; Plastination; Death education; Grounded Theory Model. Correspondence concerning this article should be addressed to Ines Testoni, Department FISPPA – Section of Ap- plied Psychology, University of Padova, Via Venezia 8, 35131 Padova, Italy. -

The Journal of Plastination
The Journal of Plastination The official publication of the International Society for Plastination ISSN 2311-7761 IN THIS ISSUE: Influence of the Temperature on the Viscosity of Different Types of Silicone – p4 A Comparison of Different De-plastination Methodologies for Preparing Histological Sections – p10 Biomechanical Analysis of The Skin and Jejunum of Dog Cadavers Subjected To A New Anatomical Preservation Technique For Surgical Teaching – p16 Bleaching of Specimens Before Dehydration in Plastination: A Small-scale Pilot Study Using Human Intestine – p24 General Issues of Safety in Plastination – p27 Volume 30 (1); July 2018 The Journal of Plastination ISSN 2311-7761 ISSN 2311-777X online The official publication of the International Society for Plastination Editorial Board: Rafael Latorre Philip J. Adds Murcia, Spain Editor-in-Chief Institute of Medical and Biomedical Education Scott Lozanoff (Anatomy) Honolulu, HI USA St. George’s, University of London London, UK Ameed Raoof. Ann Arbor, MI USA Robert W. Henry Associate Editor Mircea-Constantin Sora Department of Comparative Medicine Vienna, Austria College of Veterinary Medicine Hong Jin Sui Knoxville, Tennessee, USA Dalian, China Selcuk Tunali Carlos Baptista Assistant Editor Toledo, OH USA Department of Anatomy Hacettepe University Faculty of Medicine Ankara, Turkey Executive Committee: Rafael Latorre, President Dmitry Starchik, Vice-President Selcuk Tunali, Secretary Carlos Baptista, Treasurer Instructions for Authors Manuscripts and figures intended for publication in The Journal of Plastination should be sent via e-mail attachment to: [email protected]. Manuscript preparation guidelines are on the last two pages of this issue. On the Cover: Right atrium of a plastinated human heart showing pectinate muscles and portion of the crista terminalis visualized by trans illumination. -

Download Them
Bodies of Information: Reinventing Bodies and Practice in Medical Education Rachel Prentice A.B., Comparative Literature, Columbia University New York, New York, 1987 Submitted to the Program in Science, Technology, and Society in Partial Fulfillment of the requirements for the Degree of Doctor of Philosophy In this History and Social Studies of Science and Technology At the Massachusetts Institute of Technology [:1.x'e d-e"X)t-U May 2004 © Copyright Rachel Prentice. All rights reserved. The author hereby grants to MIT permission to reproduce and distribute publicly paper and electronic copies of this document in whole or in part. /! /'1/7 /) Signature of Author . '(;611 ~ - - Program in the History aneOfucial Study of§cience and Technology r? /J . Certified by~ . _ Sherry Turkle, PreJfess6l{bf the Social Studies of Science and Technology May 27, 2004 ~~) Joseph Dumit Associate Professor ~~OPOI~dScience and Technology Studies. (S!S) /' ~ Hugh Gusterson -+--+--+-----.'''0---'---'''-------------===--- Associate Professor of A tmo a 0 y and ~~ience a ~~ Evelynn M. Hammonds _ ) Professor of the History of Science and "frican and African American Studies (Harvard) MASSACHUSETTS IN OF TECHNOLOGY ." ARCttIVES!, ';. , JC~ 0 1 200~ lt _._. _ ~ . ~ ~ ?/:.RIF:: S - --' ~.- .•_---- BODIES OF INFORMATION Reinventing Bodies and Practice in Medical Education By Rachel Prentice A.B., Comparative Literature Columbia University, 1987 SUBMITTED TO THE DEPARTMENT OF SCIENCE, TECHNOLOGY AND SOCIETY IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY IN SCIENCE, TECHNOLOGY AND SOCIETY AT THE MASSACHUSETTS INSTITUTE OF TECHNOLOGY June 2004 © Rachel Prentice. All rights reserved. The author hereby grants to MIT permission to reproduce and to distribute publicly paper and electronic copies ofthis thesis document in whole or in part.