Increased Expression of Annexin A7 in Temporal Lobe Tissue of Patients
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Annexin A7 Is Required for ESCRT III-Mediated Plasma Membrane Repair
Annexin A7 is required for ESCRT III-mediated plasma membrane repair Sønder, Stine Lauritzen; Boye, Theresa Louise; Tölle, Regine; Dengjel, Jörn; Maeda, Kenji; Jäättelä, Marja; Simonsen, Adam Cohen; Jaiswal, Jyoti K.; Nylandsted, Jesper Published in: Scientific Reports DOI: 10.1038/s41598-019-43143-4 Publication date: 2019 Document version Publisher's PDF, also known as Version of record Document license: CC BY Citation for published version (APA): Sønder, S. L., Boye, T. L., Tölle, R., Dengjel, J., Maeda, K., Jäättelä, M., ... Nylandsted, J. (2019). Annexin A7 is required for ESCRT III-mediated plasma membrane repair. Scientific Reports, 9(1), [6726]. https://doi.org/10.1038/s41598-019-43143-4 Download date: 09. apr.. 2020 www.nature.com/scientificreports OPEN Annexin A7 is required for ESCRT III-mediated plasma membrane repair Received: 16 November 2018 Stine Lauritzen Sønder1, Theresa Louise Boye1, Regine Tölle2,3, Jörn Dengjel 2,3, Accepted: 15 April 2019 Kenji Maeda1, Marja Jäättelä 1,4, Adam Cohen Simonsen 5, Jyoti K. Jaiswal 6,7 & Published: xx xx xxxx Jesper Nylandsted 1,4 The plasma membrane of eukaryotic cells forms the essential barrier to the extracellular environment, and thus plasma membrane disruptions pose a fatal threat to cells. Here, using invasive breast cancer cells we show that the Ca2+ - and phospholipid-binding protein annexin A7 is part of the plasma membrane repair response by enabling assembly of the endosomal sorting complex required for transport (ESCRT) III. Following injury to the plasma membrane and Ca2+ fux into the cytoplasm, annexin A7 forms a complex with apoptosis linked gene-2 (ALG-2) to facilitate proper recruitment and binding of ALG-2 and ALG-2-interacting protein X (ALIX) to the damaged membrane. -

Supplemental Information
Supplemental information Dissection of the genomic structure of the miR-183/96/182 gene. Previously, we showed that the miR-183/96/182 cluster is an intergenic miRNA cluster, located in a ~60-kb interval between the genes encoding nuclear respiratory factor-1 (Nrf1) and ubiquitin-conjugating enzyme E2H (Ube2h) on mouse chr6qA3.3 (1). To start to uncover the genomic structure of the miR- 183/96/182 gene, we first studied genomic features around miR-183/96/182 in the UCSC genome browser (http://genome.UCSC.edu/), and identified two CpG islands 3.4-6.5 kb 5’ of pre-miR-183, the most 5’ miRNA of the cluster (Fig. 1A; Fig. S1 and Seq. S1). A cDNA clone, AK044220, located at 3.2-4.6 kb 5’ to pre-miR-183, encompasses the second CpG island (Fig. 1A; Fig. S1). We hypothesized that this cDNA clone was derived from 5’ exon(s) of the primary transcript of the miR-183/96/182 gene, as CpG islands are often associated with promoters (2). Supporting this hypothesis, multiple expressed sequences detected by gene-trap clones, including clone D016D06 (3, 4), were co-localized with the cDNA clone AK044220 (Fig. 1A; Fig. S1). Clone D016D06, deposited by the German GeneTrap Consortium (GGTC) (http://tikus.gsf.de) (3, 4), was derived from insertion of a retroviral construct, rFlpROSAβgeo in 129S2 ES cells (Fig. 1A and C). The rFlpROSAβgeo construct carries a promoterless reporter gene, the β−geo cassette - an in-frame fusion of the β-galactosidase and neomycin resistance (Neor) gene (5), with a splicing acceptor (SA) immediately upstream, and a polyA signal downstream of the β−geo cassette (Fig. -

Downloaded from URL: Δ Δ Nated ALG-2 GF122) and GST-ALG-2 GF122 Was Cium.Uhnres.Utoronto.Ca/Vgm
Inuzuka et al. BMC Structural Biology 2010, 10:25 http://www.biomedcentral.com/1472-6807/10/25 RESEARCH ARTICLE Open Access Molecular basis for defect in Alix-binding by alternatively spliced isoform of ALG-2 (ALG-2ΔGF122) and structural roles of F122 in target recognition Tatsutoshi Inuzuka1, Hironori Suzuki1,2, Masato Kawasaki2, Hideki Shibata1, Soichi Wakatsuki2, Masatoshi Maki1* Abstract Background: ALG-2 (a gene product of PDCD6) belongs to the penta-EF-hand (PEF) protein family and Ca2 +-dependently interacts with various intracellular proteins including mammalian Alix, an adaptor protein in the ESCRT system. Our previous X-ray crystal structural analyses revealed that binding of Ca2+ to EF3 enables the side chain of R125 to move enough to make a primary hydrophobic pocket (Pocket 1) accessible to a short fragment of Alix. The side chain of F122, facing a secondary hydrophobic pocket (Pocket 2), interacts with the Alix peptide. An alternatively spliced shorter isoform, designated ALG-2ΔGF122, lacks Gly121Phe122 and does not bind Alix, but the structural basis of the incompetence has remained to be elucidated. Results: We solved the X-ray crystal structure of the PEF domain of ALG-2ΔGF122 in the Ca2+-bound form and compared it with that of ALG-2. Deletion of the two residues shortened a-helix 5 (a5) and changed the configuration of the R125 side chain so that it partially blocked Pocket 1. A wall created by the main chain of 121- GFG-123 and facing the two pockets was destroyed. Surprisingly, however, substitution of F122 with Ala or Gly, but not with Trp, increased the Alix-binding capacity in binding assays. -

Human Induced Pluripotent Stem Cell–Derived Podocytes Mature Into Vascularized Glomeruli Upon Experimental Transplantation
BASIC RESEARCH www.jasn.org Human Induced Pluripotent Stem Cell–Derived Podocytes Mature into Vascularized Glomeruli upon Experimental Transplantation † Sazia Sharmin,* Atsuhiro Taguchi,* Yusuke Kaku,* Yasuhiro Yoshimura,* Tomoko Ohmori,* ‡ † ‡ Tetsushi Sakuma, Masashi Mukoyama, Takashi Yamamoto, Hidetake Kurihara,§ and | Ryuichi Nishinakamura* *Department of Kidney Development, Institute of Molecular Embryology and Genetics, and †Department of Nephrology, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan; ‡Department of Mathematical and Life Sciences, Graduate School of Science, Hiroshima University, Hiroshima, Japan; §Division of Anatomy, Juntendo University School of Medicine, Tokyo, Japan; and |Japan Science and Technology Agency, CREST, Kumamoto, Japan ABSTRACT Glomerular podocytes express proteins, such as nephrin, that constitute the slit diaphragm, thereby contributing to the filtration process in the kidney. Glomerular development has been analyzed mainly in mice, whereas analysis of human kidney development has been minimal because of limited access to embryonic kidneys. We previously reported the induction of three-dimensional primordial glomeruli from human induced pluripotent stem (iPS) cells. Here, using transcription activator–like effector nuclease-mediated homologous recombination, we generated human iPS cell lines that express green fluorescent protein (GFP) in the NPHS1 locus, which encodes nephrin, and we show that GFP expression facilitated accurate visualization of nephrin-positive podocyte formation in -

Annexin 7 Mobilizes Calcium from Endoplasmic Reticulum Stores in Brainb
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Biochimica et Biophysica Acta 1742 (2004) 151–160 http://www.elsevier.com/locate/bba Review Annexin 7 mobilizes calcium from endoplasmic reticulum stores in brainB W.D. Watsona,1, M. Srivastavab,1, X. Leightonb, M. Glasmanb, M. Faradayc, L.H. Fossamd, H.B. Pollardb,*, A. Vermae aNeurology Department, National Naval Medical Center, Bethesda, MD 20814, United States bDepartment of Anatomy, Physiology, and Genetics, 4301 Jones Bridge Road, Bethesda, MD 20814, United States cDepartment of Medical Psychology, Bethesda, MD 20814, United States dDivision of Neuropharmacological Drug Products, CDER, FDA, Rockville, MD 20852, United States eDepartment of Neurology, Uniformed Services University of the Health Sciences, Bethesda, MD 20814, United States Received 18 September 2004; received in revised form 5 October 2004; accepted 12 October 2004 Available online 29 October 2004 Abstract Mobilization of intracellular calcium from inositol-1,4,5-triphosphate (IP3)-sensitive endoplasmic reticulum (ER) stores plays a prominent role in brain function. Mice heterozygous for the annexin A7 (Anx7) gene have a profound reduction in IP3 receptor function in pancreatic islets along with defective insulin secretion. We examined IP3-sensitive calcium pools in the brains of Anx7 (+/À) mice by utilizing ATP/Mg2+-dependent 45Ca2+ uptake into brain membrane preparations and tissue sections. Although the Anx7 (+/À) mouse brain displayed similar levels of IP3 binding sites and thapsigargin-sensitive 45Ca2+ uptake as that seen in wild-type mouse brain, the Anx7 (+/À) mouse brain Ca2+ pools showed markedly reduced sensitivity to IP3. -
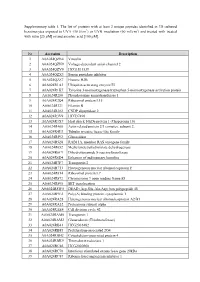
Supplementary Table 1. the List of Proteins with at Least 2 Unique
Supplementary table 1. The list of proteins with at least 2 unique peptides identified in 3D cultured keratinocytes exposed to UVA (30 J/cm2) or UVB irradiation (60 mJ/cm2) and treated with treated with rutin [25 µM] or/and ascorbic acid [100 µM]. Nr Accession Description 1 A0A024QZN4 Vinculin 2 A0A024QZN9 Voltage-dependent anion channel 2 3 A0A024QZV0 HCG1811539 4 A0A024QZX3 Serpin peptidase inhibitor 5 A0A024QZZ7 Histone H2B 6 A0A024R1A3 Ubiquitin-activating enzyme E1 7 A0A024R1K7 Tyrosine 3-monooxygenase/tryptophan 5-monooxygenase activation protein 8 A0A024R280 Phosphoserine aminotransferase 1 9 A0A024R2Q4 Ribosomal protein L15 10 A0A024R321 Filamin B 11 A0A024R382 CNDP dipeptidase 2 12 A0A024R3V9 HCG37498 13 A0A024R3X7 Heat shock 10kDa protein 1 (Chaperonin 10) 14 A0A024R408 Actin related protein 2/3 complex, subunit 2, 15 A0A024R4U3 Tubulin tyrosine ligase-like family 16 A0A024R592 Glucosidase 17 A0A024R5Z8 RAB11A, member RAS oncogene family 18 A0A024R652 Methylenetetrahydrofolate dehydrogenase 19 A0A024R6C9 Dihydrolipoamide S-succinyltransferase 20 A0A024R6D4 Enhancer of rudimentary homolog 21 A0A024R7F7 Transportin 2 22 A0A024R7T3 Heterogeneous nuclear ribonucleoprotein F 23 A0A024R814 Ribosomal protein L7 24 A0A024R872 Chromosome 9 open reading frame 88 25 A0A024R895 SET translocation 26 A0A024R8W0 DEAD (Asp-Glu-Ala-Asp) box polypeptide 48 27 A0A024R9E2 Poly(A) binding protein, cytoplasmic 1 28 A0A024RA28 Heterogeneous nuclear ribonucleoprotein A2/B1 29 A0A024RA52 Proteasome subunit alpha 30 A0A024RAE4 Cell division cycle 42 31 -

Directional Exosome Proteomes Reflect Polarity-Specific Functions in Retinal Pigmented Epithelium Monolayers
www.nature.com/scientificreports Correction: Author Correction OPEN Directional Exosome Proteomes Refect Polarity-Specifc Functions in Retinal Pigmented Epithelium Received: 9 February 2017 Accepted: 30 May 2017 Monolayers Published online: 07 July 2017 Mikael Klingeborn1, W. Michael Dismuke1, Nikolai P. Skiba1, Una Kelly1, W. Daniel Stamer1,2 & Catherine Bowes Rickman1,3 The retinal pigmented epithelium (RPE) forms the outer blood-retinal barrier in the eye and its polarity is responsible for directional secretion and uptake of proteins, lipoprotein particles and extracellular vesicles (EVs). Such a secretional division dictates directed interactions between the systemic circulation (basolateral) and the retina (apical). Our goal is to defne the polarized proteomes and physical characteristics of EVs released from the RPE. Primary cultures of porcine RPE cells were diferentiated into polarized RPE monolayers on permeable supports. EVs were isolated from media bathing either apical or basolateral RPE surfaces, and two subpopulations of small EVs including exosomes, and dense EVs, were purifed and processed for proteomic profling. In parallel, EV size distribution and concentration were determined. Using protein correlation profling mass spectrometry, a total of 631 proteins were identifed in exosome preparations, 299 of which were uniquely released apically, and 94 uniquely released basolaterally. Selected proteins were validated by Western blot. The proteomes of these exosome and dense EVs preparations suggest that epithelial polarity impacts directional release. These data serve as a foundation for comparative studies aimed at elucidating the role of exosomes in the molecular pathophysiology of retinal diseases and help identify potential therapeutic targets and biomarkers. Te retinal pigmented epithelium (RPE) is a cell monolayer that is situated between the photoreceptors and the systemic circulation of the choroid. -

The Dynamic Phagosomal Proteome and the Contribution of the Endoplasmic Reticulum
The dynamic phagosomal proteome and the contribution of the endoplasmic reticulum Lindsay D. Rogers and Leonard J. Foster* Centre for Proteomics, Department of Biochemistry and Molecular Biology, University of British Columbia, 301-2185 East Mall, Vancouver, BC, Canada V6T 1Z4 Edited by Emil R. Unanue, Washington University School of Medicine, St. Louis, MO, and approved October 4, 2007 (received for review June 23, 2007) Macrophages use phagocytosis to control the spread of pathogens LTQ-Orbitrap to measure the dynamics of the maturing phago- in the body, to clear apoptotic cells, and to aid in tissue remodeling. somal proteome with unparalleled accuracy. The phagosomal membrane is traditionally thought to originate IgG was chosen as an opsonin rather than whole serum (6) to from the plasmalemma and then go through a series of maturation reduce potentially confounding effects of phagocytosis through steps involving sequential fusion with endosomal compartments, different receptor systems. IgG-opsonized latex beads were leading to the formation of a phagolysosome. A recent model allowed to internalize for 10 min, and then latex bead-containing suggests that the endoplasmic reticulum (ER) is involved in the vacuoles (LBVs) were harvested at seven different time points maturation as well. Here we use stable isotope labeling and (Fig. 1). We focused on events within2hofphagocytosis because multiple quantitative proteomic approaches to follow the dynamic most internalized objects are dead or destroyed by this time and composition of the maturing phagosome in RAW 264.7 macro- there is no apparent physiological relevance to allowing vacuoles phage cells to a greater depth and higher temporal resolution than containing inert latex to mature for longer periods. -
Genetic Analysis of Hematological Parameters in Incipient Lines of the Collaborative Cross
MOUSE GENETIC RESOURCES Genetic Analysis of Hematological Parameters in Incipient Lines of the Collaborative Cross Samir N. P. Kelada,*,1 David L. Aylor,†,1 Bailey C. E. Peck,* Joseph F. Ryan,* Urraca Tavarez,* Ryan J. Buus,† Darla R. Miller,†,‡ Elissa J. Chesler,‡,§ David W. Threadgill,** Gary A. Churchill,§ Fernando Pardo-Manuel de Villena,§ and Francis S. Collins,*,2 *Genome Technology Branch, National Human Genome Research Institute, National Institutes of Health, Bethesda, Maryland 20892, †Department of Genetics, The University of North Carolina, Chapel Hill, North Carolina 27599, ‡Oak § Ridge National Laboratory, Oak Ridge, Tennessee 37831, The Jackson Laboratory, Bar Harbor, Maine 04609, and **Department of Genetics, North Carolina State University, Raleigh, North Carolina 27695 ABSTRACT Hematological parameters, including red and white blood cell counts and hemoglobin KEYWORDS concentration, are widely used clinical indicators of health and disease. These traits are tightly regulated Mouse Genetic in healthy individuals and are under genetic control. Mutations in key genes that affect hematological Resource parameters have important phenotypic consequences, including multiple variants that affect susceptibility Mouse to malarial disease. However, most variation in hematological traits is continuous and is presumably Collaborative influenced by multiple loci and variants with small phenotypic effects. We used a newly developed mouse Cross resource population, the Collaborative Cross (CC), to identify genetic determinants of hematological hematology parameters. We surveyed the eight founder strains of the CC and performed a mapping study using 131 hemoglobin b incipient lines of the CC. Genome scans identified quantitative trait loci for several hematological mean red cell parameters, including mean red cell volume (Chr 7 and Chr 14), white blood cell count (Chr 18), percent volume neutrophils/lymphocytes (Chr 11), and monocyte number (Chr 1). -

Annexins: Putative Linkers in Dynamic Membrane–Cytoskeleton
Protoplasma (2007) 230: 203–215 DOI 10.1007/s00709-006-0234-7 PROTOPLASMA Printed in Austria Annexins: putative linkers in dynamic membrane–cytoskeleton interactions in plant cells D. Konopka-Postupolska Laboratory of Plant Pathogenesis, Institute of Biochemistry and Biophysics, Polish Academy of Sciences, Warsaw Received January 10, 2006; accepted March 14, 2006; published online April 24, 2007 © Springer-Verlag 2007 Summary. The plasma membrane, the most external cellular structure, proteins with similar characteristics in plant cells (Boustead is at the forefront between the plant cell and its environment. Hence, it is et al. 1989, Blackbourn et al. 1991). In vertebrates the annex- naturally adapted to function in detection of external signals, their trans- duction throughout the cell, and finally, in cell reactions. Membrane ins were grouped into 13 families. In contrast, plant annexins lipids and the cytoskeleton, once regarded as simple and static structures, seem to represent a relatively simpler, smaller, and less have recently been recognized as significant players in signal transduc- diverse family of proteins. Nevertheless, in all analysed tion. Proteins involved in signal detection and transduction are organised in specific domains at the plasma membrane. Their aggregation allows to plant species, at least two distinct proteins with molecular bring together and orient the downstream and upstream members of sig- masses between 33 and 36 kDa have been discovered nalling pathways. The cortical cytoskeleton provides a structural frame- (Smallwood et al. 1990, Shin et al. 1995, Proust et al. 1996, work for rapid signal transduction from the cell periphery into the Thonat et al. 1997). However, a search through the nucleus. -

Annexin Animal Models—From Fundamental Principles to Translational Research
International Journal of Molecular Sciences Review Annexin Animal Models—From Fundamental Principles to Translational Research Thomas Grewal 1,* , Carles Rentero 2,3 , Carlos Enrich 2,3 , Mohamed Wahba 1, Carsten A. Raabe 4 and Ursula Rescher 4,* 1 School of Pharmacy, Faculty of Medicine and Health, University of Sydney, Sydney, NSW 2006, Australia; [email protected] 2 Departament de Biomedicina, Unitat de Biologia Cel·lular, Facultat de Medicina i Ciències de la Salut, Universitat de Barcelona, 08036 Barcelona, Spain; [email protected] (C.R.); [email protected] (C.E.) 3 Centre de Recerca Biomèdica CELLEX, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), 08036 Barcelona, Spain 4 Research Group Regulatory Mechanisms of Inflammation, Center for Molecular Biology of Inflammation (ZMBE) and Cells in Motion Interfaculty Center (CiM), Institute of Medical Biochemistry, University of Muenster, 48149 Muenster, Germany; [email protected] * Correspondence: [email protected] (T.G.); [email protected] (U.R.); Tel.: +61-(0)2-9351-8496 (T.G.); +49-(0)251-83-52121 (U.R.) Abstract: Routine manipulation of the mouse genome has become a landmark in biomedical research. Traits that are only associated with advanced developmental stages can now be investigated within a living organism, and the in vivo analysis of corresponding phenotypes and functions advances the translation into the clinical setting. The annexins, a family of closely related calcium (Ca2+)- and lipid- binding proteins, are found at various intra- and extracellular locations, and interact with a broad range of membrane lipids and proteins. Their impacts on cellular functions has been extensively Citation: Grewal, T.; Rentero, C.; Enrich, C.; Wahba, M.; Raabe, C.A.; assessed in vitro, yet annexin-deficient mouse models generally develop normally and do not display Rescher, U. -

Program in Human Neutrophils Fails To
Downloaded from http://www.jimmunol.org/ by guest on September 25, 2021 is online at: average * The Journal of Immunology Anaplasma phagocytophilum , 20 of which you can access for free at: 2005; 174:6364-6372; ; from submission to initial decision 4 weeks from acceptance to publication J Immunol doi: 10.4049/jimmunol.174.10.6364 http://www.jimmunol.org/content/174/10/6364 Insights into Pathogen Immune Evasion Mechanisms: Fails to Induce an Apoptosis Differentiation Program in Human Neutrophils Dori L. Borjesson, Scott D. Kobayashi, Adeline R. Whitney, Jovanka M. Voyich, Cynthia M. Argue and Frank R. DeLeo cites 28 articles Submit online. Every submission reviewed by practicing scientists ? is published twice each month by Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts http://jimmunol.org/subscription Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html http://www.jimmunol.org/content/suppl/2005/05/03/174.10.6364.DC1 This article http://www.jimmunol.org/content/174/10/6364.full#ref-list-1 Information about subscribing to The JI No Triage! Fast Publication! Rapid Reviews! 30 days* • Why • • Material References Permissions Email Alerts Subscription Supplementary The Journal of Immunology The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2005 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. This information is current as of September 25, 2021. The Journal of Immunology Insights into Pathogen Immune Evasion Mechanisms: Anaplasma phagocytophilum Fails to Induce an Apoptosis Differentiation Program in Human Neutrophils1 Dori L.