District Health Action Plan 2011-12
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

DISTRICT : Muzaffarpur
District District District District District Sl. No. Name of Husband's/Father,s AddressDate of Catego Full Marks Percent Choice-1 Choice-2 Choice-3 Choice-4 Choice-5 Candidate Name Birth ry Marks Obtained age (With Rank) (With Rank) (With Rank) (With Rank) (With Rank) DISTRICT : Muzaffarpur 1 KIRAN KUMARIARVIND KUMAR kiran kumari c/o arvind 10-Dec-66 GEN 700 603 86.14 Muzaffarpur (1) Samastipur (1) Darbhanga (1) Vaishali (1) Champaran-E (1) kumar vill+po-parsara dis-muzaffarpur 2 ARCHANA SRI ARUN vill-ratanpur post- 11-Aug-85 ST 900 757 84.11 Muzaffarpur (2) KUMARI CHAUDHARY jagdishparn vhaya- kalyanapur dist- muzaffarpur pin-848302 3PREM LATA SHARI NAND LAL village raja bigha, p.s. 10-Jan-79 GEN 700 566 80.86 Saran (2) Muzaffarpur (3) Darbhanga (2) Gaya (4) Champaran-E (2) KUMARI PRASAD dhanarua. p.o barni district patna pin code 804452 4 REENA SINHASRI DINESH SINGH dinesh singh, d/o- sita 31-Dec-76 BC 900 721 80.11 Siwan (2) Begusarai (3) Muzaffarpur (4) Samastipur (4) Vaishali (5) sharan singh, vill- ruiya, post- ruiya bangra, p.s.- jiradei, distt- siwan 5NILAM SHRI GUJESHWER nilam srivastav c/o-shri 06-Jan-69 BC 700 554 79.14 Gopalganj (2) Siwan (3) Saran (3) Muzaffarpur (5) Patna (14) SRIVASTAV PRASAD akhilesh prasad vill-manichapar, po-hathua dis-gopalginj pin-841436 6 BEENA KUMARIMAHARANGHI vill-mahrana 01-Oct-75 BC 900 700 77.78 Munger (17) Lakhisarai (11) Bhagalpur (15) Muzaffarpur (6) Jamui (12) MATHO po-dahara dis-munger pin-811201 7 KANAK LATASRI ANIL KUMAR village+post- dahibhatta, 23-Dec-85 GEN 700 541 77.29 Gopalganj (5) -

Bhu-Jal News, Volume 24, No. 2 & 3, April-September, 2009
Quarterly Journal of Central Ground Water Board Ministry of Water Resources Government of India Editorial Board CHAIRMAN Sh. B.M.Jha Chairman, Central Ground Water Board MEMBERS Dr S.C.Dhiman Subrata Kunar T.M.Hunse Sushil Gupta Member (SML) Member ( T&TT) Member (ED&MM) Member(SAM) CGWB CGWB CGWB CGWB Dr A.K.Sinha Dr P.C.Chandra Dr Saumitra Mukherjee, Professor, Regional Director Head, Department of Geology Department of Geology CGWB, & Remote Sensing, University of Rajasthan, Mid-E astern Region, J.N.U, Jaipur Patna New Delhi EDITOR ASSISTANT EDITOR Dr S.K.Jain Dr S.Shekhar Scientist-D Scientist-B CGWB, HQ, Faridabad CGWB, HQ, Faridabad Manuscript Processing Dr. S. Shekhar Shri. M.Adil Scientist-B Scientist-C CGWB, HQ, Faridabad CGWB, HQ, Faridabad * The status of members of the editorial Board is as on 01.08.10 The Statement and opinions expressed by authors in this Journal are not necessarily those of the Government. Published by Chairman, Central Ground Water Board, Ministry of Water Resources, Bhu-Jal Bhawan, NH-IV, Faridabad-121 001 (Haryana). Contents of the “Bhu-Jal News” are freely reproducible with due acknowledgement. All Editorial correspondence in future may be addressed to Editor, “Bhu-Jal News”, Central Ground Water Board, Bhujal Bhawan, NH-IV, Faridabad-121 001 (Haryana). E-Mail : [email protected] Quarterly Journal Volume No.24 , Number 2&3, April- Sept,2009 Bhu-Jal News - Quarterly Journal of Central Ground Water Board with the objective to disseminate information and highlight various activities and latest technical advances in the field of Ground Water. -

Pradhan Mantri Krishi Sinchayee Yojana (Pmksy)
PRADHAN MANTRI KRISHI SINCHAYEE YOJANA (PMKSY) Sponsored by Ministry 0f Agriculture, Co-operation and farmer's welfare Government of India DISTRICT IRRIGATION PLAN (DIP) OF SARAN DISTRICT, BIHAR AGRICULTURAL TECHNOLOGY MANAGEMENT AGENCY (ATMA) SARAN 2015-16 Table of Content Executive Summary i-ix List of Tables x-xiii List of Figures xiv-xvii 1. Chapter- I General Information of Saran District 1 1.1 District Profile 1 1.2 Demography 32 1.3 Biomass & Livestock 39 1.4 Agro-Ecology 42 1.5 Climate 42 1.6 Hydrology 43 1.7 Topography and Drainage 45 1.8 Geomorphology and Soils 68 1.9 Land Use pattern 91 2. Chapter –II District Water Profile 115 2.1 Area wise, crop wise Irrigation Status 115 2.2 Production and Productivity of Major Crops 129 2.3 Irrigation Based Classification 141 3. Chapter-III Water Availability 146 3.1 Ground Water Scenario 146 3.1.1 Hydrogeology 146 3.1.2 Ground Water Resources 150 3.1.3 Chemical quality of ground water 150 3.1.4 Status of Ground Water Development 151 3.1.5 Water Conservation and Artificial Recharge 151 3.1.6 Ground water related issue and problems 152 3.1.7 Ground Water Development 153 3.2 Status of Water Availability 154 3.3 Status of Command Area 165 4. Chapter-IV Water Requirement/Demand 168 5. Chapter-V Strategic Action Plan for Irrigation in District under PMKSY 179 5.1 Action Plan for Saran District 179- 597 Executive Summary The major objective of PMKSY is to achieve convergence of investments in irrigation at the field level, expand cultivable area under assured irrigation, improve on-farm water use efficiency to reduce wastage of water, enhance the adoption of precision-irrigation and other water saving technologies (More crop per drop), enhance recharge of aquifers and introduce sustainable water conservation practices by exploring the feasibility of reusing treated municipal waste water for peri-urban agriculture and attract greater private investment in precision irrigation system. -
Saran Introduction
DISTRICT PROFILE SARAN INTRODUCTION Saran district is one of the thirty-eight districts of Bihar. Saran district is a part of Saran division. Saran district is also known as Chhapra district because the headquarters of this district is Chhapra. Saran district is bounded by the districts of Siwan, Gopalganj, West Champaran, Muzaffarpur, Patna, Vaishali and Bhojpur of Bihar and Ballia district of Uttar Pradesh. Important rivers flowing through Saran district are Ganga, Gandak, and Ghaghra which encircle the district from south, north east and west side respectively. HISTORICAL BACKGROUND Saran was earlier known as ‘SHARAN’ which means refuge in English, after the name given to a Stupa (pillar) built by Emperor Ashoka. Another view is that the name Saran has been derived from SARANGA- ARANYA or the deer forest since the district was famous for its forests and deer in pre-historic times. In ancient days, the present Saran division, formed a part of Kosala kingdom. According to 'Ain-E-Akbari’, Saran was one of the six Sarkars/ revenue divisions, constituting the province of Bihar. By 1666, the Dutch established their trade in saltpetre at Chhapra. Saran was one of the oldest and biggest districts of Bihar. In 1829, Saran along with Champaran, was included in the Patna Division. Saran was separated from Champaran in 1866 when Champaran district was constituted. In 1981, the three subdivisions of the old Saran district namely Saran, Siwan and Gopalganj became independent districts which formed a part of Saran division. There are a few villages in Saran which are known for their historical and social significance. -

ANSWERED ON:28.07.2005 DEVELOPMENT of RAILWAY STATIONS in BIHAR Modi Shri Sushil Kumar
GOVERNMENT OF INDIA RAILWAYS LOK SABHA UNSTARRED QUESTION NO:838 ANSWERED ON:28.07.2005 DEVELOPMENT OF RAILWAY STATIONS IN BIHAR Modi Shri Sushil Kumar Will the Minister of RAILWAYS be pleased to state: (a) the name of railway stations in Bihar proposed to be developed by the Government during the current year; (b) whether expansion/renovation works have been started at Pirpainti Railway Station; (c) if so, the time by which expansion/renovation works are likely to be completed at the said station; and (d) the funds earmarked for the purpose? Answer MINISTER OF STATE IN THE MINISTRY OF RAILWAYS (SHRI R. VELU) (a) to (d): A statement is attached. STATEMENT REFERRED TO IN REPLY TO PARTS (a) TO (d) OF UNSTARRED QUESTION NO. 838 BY SHRI SUSHIL KUMAR MODI TO BE ANSWERED IN LOK SABHA ON 28.07.2005 REGARDING DEVELOPMENT OF RAILWAY STATIONS IN BIHAR. (a) Upgradation/renovation/modernisation of railway stations is a continuous process and the same is undertaken every year in accordance with the laid down norms based on traffic growth and inter-se priorities. In addition, improvements at stations are also carried out as a part of Doublings, Traffic Facility works, Gauge Conversions and computerisation, etc. The names of stations in Bihar where works relating to development of Railway Stations are in progress are as under:- Abhaipur,Chausa,Hathua,Mahesh Khunte,Pussa Road, Akbarnagar,Chhapra Jn.,Hathua,Mahipal Road,Ragendranagar Bihar Amba Pindapur,Dalsingh Sarai,Hatidah,Malda Town,Rajnagar Ara,Danapur,Jamalpur,Mananpur,Rajta Halt, Aunta Halt,Darbhanga,Jangipur,Mandarhill,Ratanpur -

Bihar Eng 21 to 30 Set
Achievements of Railways LoPN Hkkjr in ,d dne LoPNrk dh vksj Nawada Lok Sabha Constituency ge lc dk gks ,d gh ukjkA lkiQ lqFkjk gks jsy gekjkAA of Bihar East Central Railway, Hajipur Works / Projects Completed : l Provision of ROB in lieu of level crossing l Stoppage of Train no. 15619/15620 no. 33 in Nawada Yard. l Gaya - Kamakhya Express (Weekly) at Provision of Limited Height Subways in lieu of level crossings no. 27, 29, 17, 19, Nawada and Warisaliganj Stations. 40 and 50. l Extension of Loop Line at Nawada Works / Projects planned in future : Station. l New Line between Koderma - Tilaiya. l Development of Nawada, Sheikh- pura, l New Line between Nawada - Lakhimpur Warisaliganj, Hisua as Adarsh Station. l Improvement work of circulating area, l Provision of benches and sheds at extension of FOB, renovation of station building, extension of PF No. 1, 2nd various halt stations. class waiting hall, Pay & Use Toilet l Electrification of Kiul - Gaya Section. along with passenger amenities at l Provision of additional loop line at Warisaliganj Station. Sheikhpura Station. l Improvement work of circulating area, replacement of old FOB by new 3 m l Improvement work of approach road wide FOB, renovation of station building and basic infrastructure at manned LCs along with passenger amenities at in Nawada. Nawada Station. l Provision of water supply with new deep l 30 bed running room at Tilaiya. tubewell with pipe line at Sheikhpura and Nawada Stations. l Improvement of various Halt stations Lean to shed with benches. Ongoing Works / Projects : l Doubling of Kiul - Gaya Section. -

Livelihood Pattern of Scheduled Castes of Saran District
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by ZENODO International Journal of Human Resource & Industrial Research, Vol.3, Issue 7, Dec, 2016, pp 01-11, ISSN: 2349 –3593 (Online), ISSN: 2349 –4816 (Print) LIVELIHOOD PATTERN OF SCHEDULED CASTES OF SARAN DISTRICT Dr. Rupa Kumari1 & Ms. Sweta Jyoti2 1 Associate Professor, HOD, Department of Geography, M.D.D.M College, B.R,A.Bihar University , Muzaffarpur. Bihar. 2 Research Scholar, B.R.A.Bihar University, Muzaffarpur. Bihar. www.arseam.com Abstract The term Scheduled Caste, an expression standardized in the Constitution of India, was coined by Simon Commission in course of its study of the cases of those castes or groups , and was embodied in Section 309 of the Government of India Act, 1935. The Constitution of India adopted the term Scheduled Castes as coined by Simon Commission to designate them as dalits or depressed classes. This paper studies the Scheduled Castes, relating them to their Livelihood patterns, which may give valuable suggestions for their development. The present study may provide good suggestions for the well-being of this neglected class of the society and bringing them at par with the other castes. Key words: Scheduled Caste, Livelihood, SARAN District, Constitution of India Introduction: - The classification of Indian society based on Castes is unique. In India caste determines the interaction between the different social classes. A Hindu belongs to the caste of his or her parents where they remain and it becomes very difficult -
Town Wise Revised Action Plan for Polluted River Stretches in the State of Bihar Original Application No: 200/2014 (Matter : M.C
INDEX Town wise Revised Action Plan for polluted River Stretches in the State of Bihar Original application No: 200/2014 (Matter : M.C. Mehta Vs Union of India & Orgs) S.No. Particulars Page No 1 Synopsis 1-7 Maps showing ongoing /Proposed Sewerage Scheme in 2 8 Towns under Polluted Stretch & Tributaries Map showing Patna town division into zones for Sewerage 3 9 Schemes Compliance report in terms of progress in Quarter related to 4 10-15 STPs in the state of Bihar Report related to Polluted Stretches and Lying of sewage 5 network, collection and disposal of sewage, interception and 16-33 diversion of drains carrying sewage to STP. 6 Ganga River Tributary Towns 34-35 7 SWM Status & Action Plan for Ganga & its Tributaries 36-38 8 ODF Status & Action Plan of Ganga & its tributaries 39 9 Status of Plastic Waste Management 40 10 Annexures Status of Ongoing / Tendered / Tender to be floated of Schemes under Namami Gange Program i. and 41-48 Status of Screening with Sewerage Schemes : Annexure- i Solid Waste Management Status Report in Ganga Towns and ii. Status of different Components of SWM and allied Works at 49-52 Ghats: Annexure- ii Report of Plastic Carry Bags Since coming into effect of iii. Plastic Waste Management Byelaws till date: 53-56 Annexure- iii Toilet Status of Ganga Town ULBs and Status of ODF ULBs iv. Certified by QCI: 57-59 Annexure- iv 60-68 and 69 11 Status on Utilization of treated sewage (Column- 1) 12 Flood Plain regulation 69 (Column-2) 13 E Flow in river Ganga & tributaries 70 (Column-4) 14 Assessment of E Flow 70 (Column-5) 70 (Column- 3) 15 Adopting good irrigation practices to Conserve water and 71-76 16 Details of Inundated area along Ganga river with Maps 77-90 17 Rain water harvesting system in river Ganga & tributaries 91-96 18 Letter related to regulation of Ground water 97 Compliance report to the prohibit dumping of bio-medical 19 98-99 waste Securing compliance to ensuring that water quality at every 20 100 (Column- 5) point meets the standards. -

Master Plan for Patna - 2031
IMPROVING DRAFT MASTER PLAN FOR PATNA - 2031 FINAL REPORT Prepared for, Department of Urban Development & Housing, Govt. of Bihar Prepared by, CEPT, Ahmadabad FINAL REPORT IMPROVING DRAFT MASTER PLAN FOR PATNA-2031 FINAL REPORT IMPROVING DRAFT MASTER PLAN FOR PATNA - 2031 Client: Urban Development & Housing Department Patna, Bihar i Prepared by: Center for Environmental Planning and Technology (CEPT) University Kasturbhai Lalbhai Campus, University Road, Navrangpura, Ahmedabad – 380 009 Gujarat State Tel: +91 79 2630 2470 / 2740 l Fax: +91 79 2630 2075 www.cept.ac.in I www.spcept.ac.in CEPT UNIVERSITY I AHMEDABAD i FINAL REPORT IMPROVING DRAFT MASTER PLAN FOR PATNA-2031 TABLE OF CONTENTS TABLE OF CONTENTS i LIST OF TABLES v LIST OF FIGURES vii LIST OF MAPS viii LIST of ANNEXURE ix 1 INTRODUCTION 10 1.1 Introduction 11 1.2 Planning Significance of Patna as a City 12 1.3 Economic Profile 14 1.4 Existing Land Use – Patna Municipal Corporation Area 14 1.5 Previous Planning Initiatives 16 1.5.1 Master Plan (1961-81) 16 1.5.2 Plan Update (1981-2001) 17 1.5.3 Master Plan 2001-21 18 1.6 Need for the Revision of the Master Plan 19 1.7 Methodology 20 1.7.1 Stage 1: Project initiation 20 1.7.2 Stage 02 and 03: Analysis of existing situation & Future projections and Concept Plan 21 1.7.3 Stage 04: Updated Base Map and Existing Land Use Map 21 1.7.4 Stage 5: Pre-final Master Plan and DCR 24 2 DELINEATION OF PATNA PLANNING AREA 25 i 2.1 Extent of Patna Planning Area (Project Area) 26 2.2 Delineation of Patna Planning Area (Project Area) 27 2.3 Delineated -

Livelihood Pattern of Scheduled Castes of Saran District
International Journal of Human Resource & Industrial Research, Vol.3, Issue 7, Dec, 2016, pp 01-11, ISSN: 2349 –3593 (Online), ISSN: 2349 –4816 (Print) LIVELIHOOD PATTERN OF SCHEDULED CASTES OF SARAN DISTRICT Dr. Rupa Kumari1 & Ms. Sweta Jyoti2 1 Associate Professor, HOD, Department of Geography, M.D.D.M College, B.R,A.Bihar University , Muzaffarpur. Bihar. 2 Research Scholar, B.R.A.Bihar University, Muzaffarpur. Bihar. www.arseam.com Abstract The term Scheduled Caste, an expression standardized in the Constitution of India, was coined by Simon Commission in course of its study of the cases of those castes or groups , and was embodied in Section 309 of the Government of India Act, 1935. The Constitution of India adopted the term Scheduled Castes as coined by Simon Commission to designate them as dalits or depressed classes. This paper studies the Scheduled Castes, relating them to their Livelihood patterns, which may give valuable suggestions for their development. The present study may provide good suggestions for the well-being of this neglected class of the society and bringing them at par with the other castes. Key words: Scheduled Caste, Livelihood, SARAN District, Constitution of India Introduction: - The classification of Indian society based on Castes is unique. In India caste determines the interaction between the different social classes. A Hindu belongs to the caste of his or her parents where they remain and it becomes very difficult for anyone to change their caste status. Andre Beteille defines caste as “a small and named -

1 113 - Ekma BAYA BHAG ANIL KUMAR SINGH ASST TEACHER B.R.C EKMA BEO EKMA EKMA 9631494871
BLO Sl Ac No and Booth Name Name of office in Controling Block Mobile No Name Name Designation which post Office Name No. UTKRAMIT MADHYA VIDYALAY DOHAR 1 113 - Ekma BAYA BHAG ANIL KUMAR SINGH ASST TEACHER B.R.C EKMA BEO EKMA EKMA 9631494871 UTKRAMIT MADHYA VIDYALAY DOHAR 2 113 - Ekma DAYA BHAG SATY PRAKSH SINGH ASS TEACHER B.R.C EKMA BEO EKMA EKMA 9546916970 DR SHASHI BHUSHAN 3 113 - Ekma UTKRAMIT MADHYA VIDYALAY TESUAR SHAHI TEACHER B.R.C EKMA BEO EKMA EKMA 9431088243 4113 - Ekma PRATHMIK VIDYALAY KHAJUAN RAGHO PRASAD TEACHER B.R.C EKMA BEO EKMA EKMA 9546013960 UTKRAMIT UCHCH VIDYALAY DEVPURA 5 113 - Ekma DAYA BHAG RAJEEV SHAHI TEACHER B.R.C EKMA BEO EKMA EKMA 9006662771 UTKRAMIT UCHCH VIDYALAY DEVPURA JAYNANDAN PRASAD 6 113 - Ekma BAYA BHAG SHAHI TEACHER B.R.C EKMA BEO EKMA EKMA 9973885943 7113 - Ekma PRATHMIK VIDYALAY ITAHRI PANKAJ KUMAR TEACHER B.R.C EKMA BEO EKMA EKMA 9771131649 UTKRAMIT MADHYA VIDYALAY 8 113 - Ekma JAMANPURA DAYA BHAG ANIL PRASAD TEACHER B.R.C EKMA BEO EKMA EKMA 8292667913 UTKRAMIT MADHYA VIDYALAY 9 113 - Ekma JAMANPURA BAYA BHAG KRISHNA BAITA TEACHER B.R.C EKMA BEO EKMA EKMA 9546744690 MD KALAMUDDIN 10 113 - Ekma PRATHAMIK VIDYALAY HANUMANGANJ HUSSAIN TEACHER B.R.C EKMA BEO EKMA EKMA 9006315414 KANYA MADHYA VIDYALAY BATHANI SHAMBHUNATH 11 113 - Ekma TOLA BENAUT CHODHRI TEACHER B.R.C EKMA BEO EKMA EKMA 9931923400 BRAJESH KUMAR 12 113 - Ekma MADHYA VIDYALAY BALIYA BAYA BHAG SINGH TEACHER B.R.C EKMA BEO EKMA EKMA 7759985752 13113 - Ekma MADHY VIDHYALAY, BALIYA DAYA BHAG ANIL KUMAR PRASAD TEACHER B.R.C EKMA BEO EKMA EKMA 9955571980 BLO Sl Ac No and Booth Name Name of office in Controling Block Mobile No Name Name Designation which post Office Name No. -
Population of Class Wise Towns in Bihar
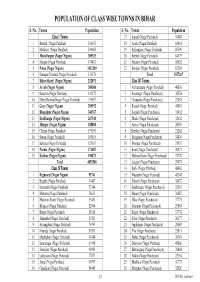
POPULATION OF CLASS WISE TOWNS IN BIHAR S. No. Towns Population S. No. Towns Population Class I Towns 17 Supaul (Nagar Parishad) 54085 1 Bettiah (Nagar Parishad) 116670 18 Araria (Nagar Parishad) 60861 2 Motihari (Nagar Parishad) 100683 19 Kishanganj (Nagar Parishad) 85590 3 Muzaffarpur (Nagar Nigam) 305525 20 Beehat (Nagar Parishad) 64579 4 Hajipur (Nagar Parishad) 119412 21 Barauni (Nagar Parishad) 58628 5 Patna (Nagar Nigam) 1432209 22 Benipur (Nagar Parishad) 62203 6 Danapur Nizamat (Nagar Parishad) 131176 Total 1557267 7 Bihar Sharif (Nagar Nigam) 232071 Class III Towns 8 Arrah (Nagar Nigam) 203380 1 Narkatiaganj (Nagar Parishad) 40830 9 Sasaram (Nagar Parishad) 131172 2 Ramnagar (Nagar Panchayat) 38554 10 Dehri DalmiyaNagar (Nagar Parishad) 119057 3 Chanpatia (Nagar Panchayat) 22038 11 Gaya (Nagar Nigam) 389192 4 Raxaul (Nagar Parishad) 41610 12 Bhagalpur (Nagar Nigam) 340767 5 Sugauli (Nagar Panchayat) 31432 13 Darbhanga (Nagar Nigam) 267348 6 Dhaka (Nagar Panchayat) 32632 14 Munger (Nagar Nigam) 188050 7 Areraj (Nagar Panchayat) 20356 15 Chapra (Nagar Parishad) 179190 8 Sheohar (Nagar Panchayat) 21262 16 Siwan (Nagar Parishad) 109919 9 Bairgania (Nagar Panchayat) 34836 17 Saharsa (Nagar Parishad) 125167 10 Motipur (Nagar Panchayat) 21957 18 Purnia (Nagar Nigam) 171687 11 Kanti (Nagar Panchayat) 20871 19 Katihar (Nagar Nigam) 190873 12 Mahnar Bazar (Nagar Panchayat) 37370 Total 4853548 13 Lalganj (Nagar Panchayat) 29873 Class II Towns 14 Barh (Nagar Parishad) 48442 1 Begusarai (Nagar Nigam) 93741 15 Masaurhi (Nagar Parishad) 45248