AR Splicing Variants and Resistance to AR Targeting Agents
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Detection of Interacting Transcription Factors in Human Tissues Using
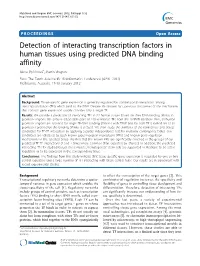
Myšičková and Vingron BMC Genomics 2012, 13(Suppl 1):S2 http://www.biomedcentral.com/1471-2164/13/S1/S2 PROCEEDINGS Open Access Detection of interacting transcription factors in human tissues using predicted DNA binding affinity Alena Myšičková*, Martin Vingron From The Tenth Asia Pacific Bioinformatics Conference (APBC 2012) Melbourne, Australia. 17-19 January 2012 Abstract Background: Tissue-specific gene expression is generally regulated by combinatorial interactions among transcription factors (TFs) which bind to the DNA. Despite this known fact, previous discoveries of the mechanism that controls gene expression usually consider only a single TF. Results: We provide a prediction of interacting TFs in 22 human tissues based on their DNA-binding affinity in promoter regions. We analyze all possible pairs of 130 vertebrate TFs from the JASPAR database. First, all human promoter regions are scanned for single TF-DNA binding affinities with TRAP and for each TF a ranked list of all promoters ordered by the binding affinity is created. We then study the similarity of the ranked lists and detect candidates for TF-TF interaction by applying a partial independence test for multiway contingency tables. Our candidates are validated by both known protein-protein interactions (PPIs) and known gene regulation mechanisms in the selected tissue. We find that the known PPIs are significantly enriched in the groups of our predicted TF-TF interactions (2 and 7 times more common than expected by chance). In addition, the predicted interacting TFs for studied tissues (liver, muscle, hematopoietic stem cell) are supported in literature to be active regulators or to be expressed in the corresponding tissue. -

Tolerance to Sustained Activation of the Camp/Creb Pathway Activity in Osteoblastic Cells Is Enabled by Loss of P53 Mannu K
Walia et al. Cell Death and Disease (2018) 9:844 DOI 10.1038/s41419-018-0944-8 Cell Death & Disease ARTICLE Open Access Tolerance to sustained activation of the cAMP/Creb pathway activity in osteoblastic cells is enabled by loss of p53 Mannu K. Walia1, Scott Taylor1,PatriciaW.M.Ho1,T.JohnMartin1,2 and Carl R. Walkley 1,2,3 Abstract The loss of p53 function is a central event in the genesis of osteosarcoma (OS). How mutation of p53 enables OS development from osteoblastic lineage cells is poorly understood. We and others have reported a key role for elevated and persistent activation of the cAMP/PKA/Creb1 pathway in maintenance of OS. In view of the osteoblast lineage being the cell of origin of OS, we sought to determine how these pathways interact within the context of the normal osteoblast. Normal osteoblasts (p53 WT) rapidly underwent apoptosis in response to acute elevation of cAMP levels or activity, whereas p53-deficient osteoblasts tolerated this aberrant cAMP/Creb level and activity. Using the p53 activating small-molecule Nutlin-3a and cAMP/Creb1 activator forskolin, we addressed the question of how p53 responds to the activation of cAMP. We observed that p53 acts dominantly to protect cells from excessive cAMP accumulation. We identify a Creb1-Cbp complex that functions together with and interacts with p53. Finally, translating these results we find that a selective small-molecule inhibitor of the Creb1-Cbp interaction demonstrates selective toxicity to OS cells where this pathway is constitutively active. This highlights the cAMP/Creb axis as a potentially actionable therapeutic vulnerability in p53-deficient tumors such as OS. -

Genetics of Gene Expression in Primary Immune Cells Identifies Cell
ARTICLES Genetics of gene expression in primary immune cells identifies cell type–specific master regulators and roles of HLA alleles Benjamin P Fairfax1, Seiko Makino1, Jayachandran Radhakrishnan1, Katharine Plant1, Stephen Leslie2, Alexander Dilthey3, Peter Ellis4, Cordelia Langford4, Fredrik O Vannberg1,5 & Julian C Knight1 Trans-acting genetic variants have a substantial, albeit poorly characterized, role in the heritable determination of gene expression. Using paired purified primary monocytes and B cells, we identify new predominantly cell type–specific cis and trans expression quantitative trait loci (eQTLs), including multi-locus trans associations to LYZ and KLF4 in monocytes and B cells, respectively. Additionally, we observe a B cell–specific trans association of rs11171739 at 12q13.2, a known autoimmune disease locus, with IP6K2 (P = 5.8 × 10−15), PRIC285 (P = 3.0 × 10−10) and an upstream region of CDKN1A (P = 2 × 10−52), suggesting roles for cell cycle regulation and peroxisome proliferator-activated receptor γ (PPARγ) signaling in autoimmune pathogenesis. We also find that specific human leukocyte antigen (HLA) alleles form trans associations with the expression of AOAH and ARHGAP24 in monocytes but not in B cells. In summary, we show that mapping gene expression in defined primary cell populations identifies new cell type–specific trans-regulated networks and provides insights into the genetic basis of disease susceptibility. Defining the genetic determinants of gene expression is crucial to especially pertinent in the elucidation of trans-acting eQTLs, where understanding the biological and medical significance of genetic var- context specificity may be of greater relevance12. iation. This is particularly relevant in the drive to identify functional Here we sought to determine cell type–specific eQTLs relevant to variants underlying observed disease associations from genome- immunity and inflammation in paired samples of primary monocytes wide association studies (GWAS)1. -

Molecular Pathogenesis and Regulation of the Mir-29-3P-Family: Involvement of ITGA6 and ITGB1 in Intra-Hepatic Cholangiocarcinoma
cancers Article Molecular Pathogenesis and Regulation of the miR-29-3p-Family: Involvement of ITGA6 and ITGB1 in Intra-Hepatic Cholangiocarcinoma Yuto Hozaka 1 , Naohiko Seki 2,* , Takako Tanaka 1, Shunichi Asai 2, Shogo Moriya 3, Tetsuya Idichi 1, Masumi Wada 1, Kiyonori Tanoue 1, Yota Kawasaki 1, Yuko Mataki 1 , Hiroshi Kurahara 1 and Takao Ohtsuka 1 1 Department of Digestive Surgery, Breast and Thyroid Surgery, Graduate School of Medical and Dental Sciences, Kagoshima University, Kagoshima 890-8520, Japan; [email protected] (Y.H.); [email protected] (T.T.); [email protected] (T.I.); [email protected] (M.W.); [email protected] (K.T.); [email protected] (Y.K.); [email protected] (Y.M.); [email protected] (H.K.); [email protected] (T.O.) 2 Department of Functional Genomics, Graduate School of Medicine, Chiba University, Chiba 260-8670, Japan; [email protected] 3 Department of Biochemistry and Genetics, Graduate School of Medicine, Chiba University, Chiba 260-8670, Japan; [email protected] * Correspondence: [email protected]; Tel.: +81-43-226-2971 Simple Summary: Even today, there are no effective targeted therapies for intrahepatic cholan- giocarcinoma (ICC) patients. Clarifying the molecular pathogenesis of ICC will contribute to the Citation: Hozaka, Y.; Seki, N.; development of treatment strategies for this disease. In this study, we searched for the role of the Tanaka, T.; Asai, S.; Moriya, S.; Idichi, miR-29-3p-family and its association with oncogenic pathway. Interestingly, aberrant expression of T.; Wada, M.; Tanoue, K.; Kawasaki, ITGA6 and ITGB1 was directly regulated by the miR-29-3p-family which are involved in multiple Y.; Mataki, Y.; et al. -
Genequery™ Human Stem Cell Transcription Factors Qpcr Array
GeneQuery™ Human Stem Cell Transcription Factors qPCR Array Kit (GQH-SCT) Catalog #GK125 Product Description ScienCell's GeneQuery™ Human Stem Cell Transcription Factors qPCR Array Kit (GQH-SCT) surveys a panel of 88 transcription factors related to stem cell maintenance and differentiation. Transcription factors are proteins that can regulate target gene transcription level by binding to specific regions of the genome known as enhancers or silencers. Brief examples of how genes may be grouped according to their functions are shown below: • Pluripotency transcription factors: NANOG, POU5F1, SOX2 • Embryonic development: EOMES, FOXC2/D3/O1, HOXA9/A10, KLF2/5, LIN28B, MAX, PITX2, SMAD1, TBX5, ZIC1 • Germ layer formation and differentiation: FOXA2, GATA6, HAND1, ISL1, KLF4, SMAD2, SOX9 • Organ morphogenesis: EZH2, HOXA11/B3/B5/C9, MSX2, MYC, PAX5/8, VDR • Angiogenesis: CDX2, JUN, NR2F2, RUNX1, WT1 • Hematopoiesis and osteogenesis: EGR3, ESR1, GATA1/2/3, GLI2, NFATC1, PAX9, RB1, SOX6, SP1, STAT1 • Neural stem cell maintenance and differentiation: ATF2, CREB1, FOSB, FOXO3, HES1, HOXD10, MCM2/7, MEF2C, NEUROD1/G1, OLIG1/2, PAX3/6, POU4F1, PPARG, SMAD3/4, SNAI1, STAT3 Note : all gene names follow their official symbols by the Human Genome Organization Gene Nomenclature Committee (HGNC). GeneQuery™ qPCR array kits are qPCR ready in a 96-well plate format, with each well containing one primer set that can specifically recognize and efficiently amplify a target gene's cDNA. The carefully designed primers ensure that: (i) the optimal annealing temperature in qPCR analysis is 65°C (with 2 mM Mg 2+ , and no DMSO); (ii) the primer set recognizes all known transcript variants of target gene, unless otherwise indicated; and (iii) only one gene is amplified. -

NF-Y Controls Fidelity of Transcription Initiation at Gene Promoters
ARTICLE https://doi.org/10.1038/s41467-019-10905-7 OPEN NF-Y controls fidelity of transcription initiation at gene promoters through maintenance of the nucleosome-depleted region Andrew J. Oldfield 1,6, Telmo Henriques1,2,8, Dhirendra Kumar1,8, Adam B. Burkholder3,8, Senthilkumar Cinghu1, Damien Paulet4,5, Brian D. Bennett3, Pengyi Yang 1,7, Benjamin S. Scruggs1, Christopher A. Lavender3, Eric Rivals 4,5, Karen Adelman1,2 & Raja Jothi1 1234567890():,; Faithful transcription initiation is critical for accurate gene expression, yet the mechanisms underlying specific transcription start site (TSS) selection in mammals remain unclear. Here, we show that the histone-fold domain protein NF-Y, a ubiquitously expressed transcription factor, controls the fidelity of transcription initiation at gene promoters in mouse embryonic stem cells. We report that NF-Y maintains the region upstream of TSSs in a nucleosome- depleted state while simultaneously protecting this accessible region against aberrant and/or ectopic transcription initiation. We find that loss of NF-Y binding in mammalian cells disrupts the promoter chromatin landscape, leading to nucleosomal encroachment over the canonical TSS. Importantly, this chromatin rearrangement is accompanied by upstream relocation of the transcription pre-initiation complex and ectopic transcription initiation. Further, this phenomenon generates aberrant extended transcripts that undergo translation, disrupting gene expression profiles. These results suggest NF-Y is a central player in TSS selection in metazoans and highlight the deleterious consequences of inaccurate transcription initiation. 1 Epigenetics and Stem Cell Biology Laboratory, National Institute of Environmental Health Sciences, National Institutes of Health, Research Triangle Park, Durham, NC 27709, USA. 2 Department of Biological Chemistry and Molecular Pharmacology, Harvard Medical School, Boston, MA 02115, USA. -

Onl Er Msb 145504 GA 1..19
UC Irvine UC Irvine Previously Published Works Title Proteomic analyses reveal distinct chromatin-associated and soluble transcription factor complexes. Permalink https://escholarship.org/uc/item/1fz5r77k Journal Molecular systems biology, 11(1) ISSN 1744-4292 Authors Li, Xu Wang, Wenqi Wang, Jiadong et al. Publication Date 2015-01-21 DOI 10.15252/msb.20145504 License https://creativecommons.org/licenses/by/4.0/ 4.0 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Article Proteomic analyses reveal distinct chromatin- associated and soluble transcription factor complexes Xu Li1,†, Wenqi Wang1,†, Jiadong Wang1, Anna Malovannaya2, Yuanxin Xi2,3, Wei Li2,3, Rudy Guerra4, David H Hawke5, Jun Qin2 & Junjie Chen1,* Abstract living organisms. Sophisticated signal transduction pathways are required for the development and survival of any organism, a minor The current knowledge on how transcription factors (TFs), the ulti- disruption of which may cause developmental defects and diseases mate targets and executors of cellular signalling pathways, are such as cancer (Fig 1A). The examples of these highly conserved regulated by protein–protein interactions remains limited. Here, signalling pathways include the Wnt (MacDonald et al,2009),TGF-b we performed proteomics analyses of soluble and chromatin- (Massague, 1998) and NF-jB (Hayden & Ghosh, 2004) pathways. associated complexes of 56 TFs, including the targets of many Many of these pathways function by ultimately regulating the signalling pathways involved in development and cancer, and 37 activity of certain transcription factors (TFs), often by changing their members of the Forkhead box (FOX) TF family. Using tandem affin- localizations. Reports on individual proteins suggested that the ity purification followed by mass spectrometry (TAP/MS), we chromatin association of TFs is tightly controlled by upstream signals. -

Mecp2 Enforces Foxp3 Expression to Promote Regulatory T
MeCP2 enforces Foxp3 expression to promote PNAS PLUS regulatory T cells’ resilience to inflammation Chaoran Lia,1, Shan Jianga,1,2, Si-Qi Liua, Erik Lykkena, Lin-tao Zhaob, Jose Sevillaa, Bo Zhub, and Qi-Jing Lia,3 aDepartment of Immunology, Duke University Medical Center, Durham, NC 27710; and bInstitute of Cancer, Xinqiao Hospital, The Third Military Medical University, Chongqing 400037, China Edited by Harvey Cantor, Dana-Farber Cancer Institute, Boston, MA, and approved June 3, 2014 (received for review January 24, 2014) Forkhead box P3+ (Foxp3+) regulatory T cells (Tregs) are crucial for the intestinal barrier; most intriguingly, the transplantation of peripheral tolerance. During inflammation, steady Foxp3 expres- wild-type (WT) bone marrow successfully arrested RTT disease sion in Tregs is essential for maintaining their lineage identity and in MeCP2-null mice (16). Nevertheless, apart from these cor- suppressive function. However, the molecular machinery govern- relative studies, MeCP2’s causative role in immune regulation ing Tregs’ resilience to inflammation-induced Foxp3 destabili- remains largely unexplored. + + zation remains elusive. Here, we demonstrate that methyl-CpG As potent suppressors of inflammation, CD4 CD25 regu- binding protein 2 (MeCP2), an eminent epigenetic regulator known latory T cells (Tregs) are an indispensable T-cell subset re- primarily as the etiological factor of Rett syndrome, is critical to sus- sponsible for peripheral tolerance and immune homeostasis (17). tain Foxp3 expression in Tregs during inflammation. In response to Foxp3 is the master regulator of the Treg gene expression pro- inflammatory stimuli, MeCP2 is specifically recruited to the Conserved gram, and consequently Foxp3 mutation in both humans and foxp3 Non-Coding sequence 2 region of the locus, where it collabo- mice is sufficient to trigger the development of severe lympho- rates with cAMP responsive element binding protein 1 to promote proliferative autoimmune disorders (18–24). -

Inhibition of IRF4 in Dendritic Cells by PRR-Independent
RESEARCH ARTICLE Inhibition of IRF4 in dendritic cells by PRR-independent and -dependent signals inhibit Th2 and promote Th17 responses Jihyung Lee1, Junyan Zhang1,2,3, Young-Jun Chung1,4, Jun Hwan Kim1, Chae Min Kook1, Jose´ M Gonza´ lez-Navajas3,5,6, David S Herdman1, Bernd Nu¨ rnberg7, Paul A Insel1,8, Maripat Corr1, Ji-Hun Mo4, Ailin Tao2,3, Kei Yasuda9, Ian R Rifkin9,10, David H Broide1, Roger Sciammas11, Nicholas JG Webster1,12*, Eyal Raz1,3* 1Department of Medicine, University of California San Diego, San Diego, United States; 2The Second Affiliated Hospital of Guangzhou Medical University (GMU), The State Key Laboratory of Respiratory Disease, Guangdong Provincial Key Laboratory of Allergy & Clinical Immunology, Guangzhou, China; 3Center for Immunology, Inflammation and Immune-mediated disease, GMU, Guangzhou, China; 4Department of Otorhinolaryngology-Head and Neck Surgery, Dankook University College of Medicine, Chungnam, Republic of Korea; 5Alicante Institute for Health and Biomedical Research (ISABIAL - FISABIO), Alicante, Spain; 6Networked Biomedical Research Center for Hepatic and Digestive Diseases (CIBERehd), Institute of Health Carlos III, Madrid, Spain; 7Department of Pharmacology and Experimental Therapy, University of Tu¨ bingen, Tu¨ bingen, Germany; 8Department of Pharmacology, University of California San Diego, San Diego, United States; 9Boston University School of Medicine, Boston, United States; 10VA Boston Healthcare System, Boston, United States; 11Center for Comparative Medicine, University of California, Davis, Davis, United States; 12VA San Diego Healthcare System, San Diego, United States *For correspondence: [email protected] (NJGW); [email protected] (ER) Abstract Cyclic AMP (cAMP) is involved in many biological processes but little is known Competing interests: The regarding its role in shaping immunity. -

Microrna-205 Affects Mouse Granulosa Cell Apoptosis and Estradiol
bioRxiv preprint doi: https://doi.org/10.1101/301523; this version posted April 14, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. MicroRNA-205 affects mouse granulosa cell apoptosis and estradiol synthesis by targeting CREB1 Pengju Zhang1, Jun Wang2, Hongyan Lang1, Weixia Wang1, Xiaohui Liu1, Haiyan Liu1, Chengcheng Tan1, Xintao Li1*, Yumin Zhao1*, Xinghong Wu1* 1Institute of Animal Sciences, Jilin Academy of Agricultural Sciences, #1363 Shengtai Street, Changchun 130124, Jilin Province, PR China 2College of Animal Science and Technology, Jilin Agricultural University, 2888 Xincheng Street, Changchun 130118, Jilin Province, PR China *Authors for correspondence (Xintao Li, email:[email protected]; Yumin Zhao, email:[email protected]; Xinghong Wu, email:[email protected]) ABSTRACT MicroRNAs-205 (miR-205), were reportedly to be involved in various physiological and pathological processes, but its biological function in follicular atresia remain unknown. In this study, we investigated the expression of miR-205 in mouse granulosa cells (mGCs), and explored its functions in primary mGCs using a serial of in vitro experiments. The result of qRT-PCR demonstrated that miR-205 expression was significantly increased in early atretic follicles (EAF), and progressively atretic follicles (PAF) compared to healthy follicles (HF). Our results also revealed that overexpression of miR-205 in mGCs significantly promoted apoptosis, caspas-3/9 activities, and inhibited estrogen E2 release, and cytochrome P450 family 19 subfamily A polypeptide 1 (CYP19A1, a key gene in E2 production) expression. -
CREB-Dependent Transcription in Astrocytes: Signalling Pathways, Gene Profiles and Neuroprotective Role in Brain Injury
CREB-dependent transcription in astrocytes: signalling pathways, gene profiles and neuroprotective role in brain injury. Tesis doctoral Luis Pardo Fernández Bellaterra, Septiembre 2015 Instituto de Neurociencias Departamento de Bioquímica i Biologia Molecular Unidad de Bioquímica y Biologia Molecular Facultad de Medicina CREB-dependent transcription in astrocytes: signalling pathways, gene profiles and neuroprotective role in brain injury. Memoria del trabajo experimental para optar al grado de doctor, correspondiente al Programa de Doctorado en Neurociencias del Instituto de Neurociencias de la Universidad Autónoma de Barcelona, llevado a cabo por Luis Pardo Fernández bajo la dirección de la Dra. Elena Galea Rodríguez de Velasco y la Dra. Roser Masgrau Juanola, en el Instituto de Neurociencias de la Universidad Autónoma de Barcelona. Doctorando Directoras de tesis Luis Pardo Fernández Dra. Elena Galea Dra. Roser Masgrau In memoriam María Dolores Álvarez Durán Abuela, eres la culpable de que haya decidido recorrer el camino de la ciencia. Que estas líneas ayuden a conservar tu recuerdo. A mis padres y hermanos, A Meri INDEX I Summary 1 II Introduction 3 1 Astrocytes: physiology and pathology 5 1.1 Anatomical organization 6 1.2 Origins and heterogeneity 6 1.3 Astrocyte functions 8 1.3.1 Developmental functions 8 1.3.2 Neurovascular functions 9 1.3.3 Metabolic support 11 1.3.4 Homeostatic functions 13 1.3.5 Antioxidant functions 15 1.3.6 Signalling functions 15 1.4 Astrocytes in brain pathology 20 1.5 Reactive astrogliosis 22 2 The transcription -

Combinatorial Targeting of the Androgen Receptor for Prostate
Combinatorial Targeting of the Androgen Receptor for Prostate Cancer Therapy A thesis submitted to the University of Adelaide in the fulfilment of the requirements for the degree of Doctor of Philosophy By Sarah Louise Carter B.BiomolChem.(Hons) Dame Roma Mitchell Cancer Research Laboratories School of Medicine The University of Adelaide and The Hanson Institute March 2015 Contents Chapter 1: General Introduction ........................................................................................1 1.1 Background ..................................................................................................................2 1.2 Androgens and the Prostate ..........................................................................................3 1.3 Androgen Signalling through the Androgen Receptor .................................................4 1.3.1 The androgen receptor (AR) ..................................................................................4 1.3.2 Androgen signalling in the prostate .......................................................................6 1.4 Current Treatment Strategies for Prostate Cancer ........................................................8 1.4.1 Diagnosis ...............................................................................................................8 1.4.2 Localised disease .................................................................................................10 1.4.3 Relapse and metastatic disease ............................................................................13