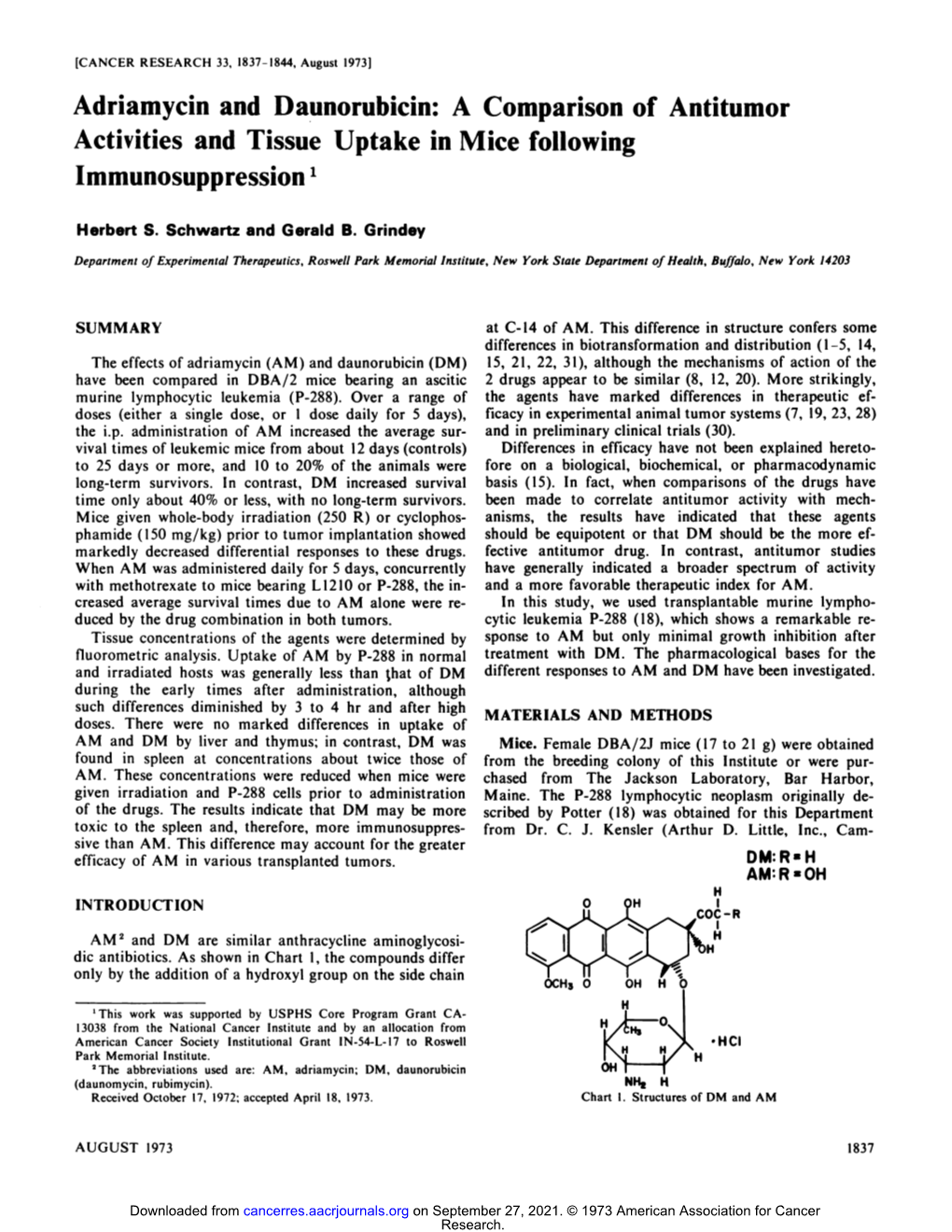
Adriamycin and Daunorubicin: a Comparison of Antitumor Activities and Tissue Uptake in Mice Following 1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Comparison of Early Intensive Methotrexate/Mercaptopurine With
Leukemia (2001) 15, 1038–1045 2001 Nature Publishing Group All rights reserved 0887-6924/01 $15.00 www.nature.com/leu A comparison of early intensive methotrexate/mercaptopurine with early intensive alternating combination chemotherapy for high-risk B-precursor acute lymphoblastic leukemia: a Pediatric Oncology Group phase III randomized trial SJ Lauer1, JJ Shuster2, DH Mahoney Jr3, N Winick4, S Toledano5, L Munoz5, G Kiefer6, JD Pullen7, CP Steuber3 and BM Camitta6 1Emory University School of Medicine, Atlanta, GA; 2Pediatric Oncology Group Statistical Office and Department of Statistics, University of Florida, Gainesville, FL; 3Texas Children’s Cancer Center, Baylor College of Medicine, Houston, TX; 4University of Texas Southwestern Medical Center, Dallas, TX; 5University Miami School of Medicine, Miami, FL; 6Midwest Children’s Cancer Center, Milwaukee, WI; and 7University of Mississippi Medical Center Children’s Hospital, Jackson, MS, USA A prospective, randomized multicenter study was performed to to their risk for relapse and treatment strategies designed to evaluate the relative efficacy of two different concepts for early improve event-free survival (EFS). intensive therapy in a randomized trial of children with B-pre- cursor acute lymphoblastic leukemia (ALL) at high risk (HR) for It is believed that the leading causes of relapse in children relapse. Four hundred and ninety eligible children with HR-ALL with higher risk ALL (HR-ALL) are inadequate cell kill and were randomized on the Pediatric Oncology Group (POG) 9006 emergence of drug-resistant clones. Clinical trials using early phase III trial between 7 January 1991 and 12 January 1994. intensive myelosuppressive combination chemotherapy as After prednisone (PDN), vincristine (VCR), asparaginase (ASP) post-induction consolidation were designed to maximize cell and daunorubicin (DNR) induction, 470 patients received either 2 kill and address drug resistance. -

Incidence of Differentiation Syndrome Associated with Treatment
Journal of Clinical Medicine Review Incidence of Differentiation Syndrome Associated with Treatment Regimens in Acute Myeloid Leukemia: A Systematic Review of the Literature Lucia Gasparovic 1, Stefan Weiler 1,2, Lukas Higi 1 and Andrea M. Burden 1,* 1 Institute of Pharmaceutical Sciences, Department of Chemistry and Applied Biosciences, ETH Zurich, 8093 Zurich, Switzerland; [email protected] (L.G.); [email protected] (S.W.); [email protected] (L.H.) 2 National Poisons Information Centre, Tox Info Suisse, Associated Institute of the University of Zurich, 8032 Zurich, Switzerland * Correspondence: [email protected]; Tel.: +41-76-685-22-56 Received: 30 August 2020; Accepted: 14 October 2020; Published: 18 October 2020 Abstract: Differentiation syndrome (DS) is a potentially fatal adverse drug reaction caused by the so-called differentiating agents such as all-trans retinoic acid (ATRA) and arsenic trioxide (ATO), used for remission induction in the treatment of the M3 subtype of acute myeloid leukemia (AML), acute promyelocytic leukemia (APL). However, recent DS reports in trials of isocitrate dehydrogenase (IDH)-inhibitor drugs in patients with IDH-mutated AML have raised concerns. Given the limited knowledge of the incidence of DS with differentiating agents, we conducted a systematic literature review of clinical trials with reports of DS to provide a comprehensive overview of the medications associated with DS. In particular, we focused on the incidence of DS reported among the IDH-inhibitors, compared to existing ATRA and ATO therapies. We identified 44 published articles, encompassing 39 clinical trials, including 6949 patients. Overall, the cumulative incidence of DS across all treatment regimens was 17.7%. -

Daunorubicin Hydrochloride Injection Hikma Pharmaceuticals USA Inc
DAUNORUBICIN HYDROCHLORIDE- daunorubicin hydrochloride injection Hikma Pharmaceuticals USA Inc. ---------- DAUNORUBICIN HYDROCHLORIDE INJECTION Rx ONLY WARNINGS 1.Daunorubicin Hydrochloride Injection must be given into a rapidly flowing intravenous infusion. It must never be given by the intramuscular or subcutaneous route. Severe local tissue necrosis will occur if there is extravasation during administration. 2.Myocardial toxicity manifested in its most severe form by potentially fatal congestive heart failure may occur either during therapy or months to years after termination of therapy. The incidence of myocardial toxicity increases after a total cumulative dose exceeding 400 to 550 mg/m2 in adults, 300 mg/m2 in children more than 2 years of age, or 10 mg/kg in children less than 2 years of age. 3.Severe myelosuppression occurs when used in therapeutic doses; this may lead to infection or hemorrhage. 4.It is recommended that daunorubicin hydrochloride be administered only by physicians who are experienced in leukemia chemotherapy and in facilities with laboratory and supportive resources adequate to monitor drug tolerance and protect and maintain a patient compromised by drug toxicity. The physician and institution must be capable of responding rapidly and completely to severe hemorrhagic conditions and/or overwhelming infection. 5.Dosage should be reduced in patients with impaired hepatic or renal function. DESCRIPTION Daunorubicin hydrochloride is the hydrochloride salt of an anthracycline cytotoxic antibiotic produced by a strain of Streptomyces coeruleorubidus. It is provided as a deep red sterile liquid in vials for intravenous administration only. Each mL contains 5 mg daunorubicin (equivalent to 5.34 mg of daunorubicin hydrochloride), 9 mg sodium chloride; sodium hydroxide and/or hydrochloric acid (to adjust pH), and water for injection, q.s. -

Benefit of Intermediate-Dose Cytarabine-Containing Induction In
Letters to the Editor ter RFS and EFS rates and showed a marked tendency to Benefit of intermediate-dose cytarabine-containing improve the OS of patients with CEBPAdm in both uni- induction in molecular subgroups of acute myeloid variate and multivariable analyses, as shown in Online leukemia Supplementary Table S2. Five-year RFS, EFS, and OS rates were 85%, 81%, and 88% in the intermediate-dose com- The outcome of acute myeloid leukemia (AML) is pared with 56%, 56%, and 68% in the conventional- affected by disease characteristics as well as treatment dose group, respectively (Figure 1). In total, 13 of 75 1-3 regimens. In the CALGB8525 trial, patients with core (17%) patients with CEBPAdm AML underwent allo- binding factor (CBF)-positive leukemia benefited from geneic transplantation in CR1, including five of 32 (16%) 4 consolidation with a high dose of cytarabine. More in the conventional-dose group and eight of 43 (19%) in 2 recently, high-dose daunorubicin (60-90 mg/m ) has the intermediate-dose group. To analyze results in the 5,6 become widely used. High-dose daunorubicin confers a absence of any possible contributory effect of transplan- favorable prognosis for patients with NPM1 muta- tation, patients were censored at the time of transplanta- 1,7,8 tions. tion in CR1. Patients with CEBPAdm AML exposed to Higher-dose cytarabine was also introduced into AML intermediate-dose cytarabine achieved an increase in 5- 3,9 induction therapy. Recently, we investigated the role of year RFS, censored at the date of transplantation, from intermediate-dose cytarabine in induction therapy of 56% to 83% (hazard ratio [HR], 0.313; 95% confidence AML and found that the introduction of intermediate- interval [95% CI]: 0.119-0.824; Wald P=0.019) (Online dose cytarabine, combined with daunorubicin and omac- Supplementary Figure S3). -
Acute Lymphoblastic Leukemia (ALL) (Part 1 Of
LEUKEMIA TREATMENT REGIMENS: Acute Lymphoblastic Leukemia (ALL) (Part 1 of 12) Note: The National Comprehensive Cancer Network (NCCN) Guidelines® for Acute Lymphoblastic Leukemia (ALL) should be consulted for the management of patients with lymphoblastic lymphoma. Clinical Trials: The NCCN recommends cancer patient participation in clinical trials as the gold standard for treatment. Cancer therapy selection, dosing, administration, and the management of related adverse events can be a complex process that should be handled by an experienced healthcare team. Clinicians must choose and verify treatment options based on the individual patient; drug dose modifications and supportive care interventions should be administered accordingly. The cancer treatment regimens below may include both U.S. Food and Drug Administration-approved and unapproved indications/regimens. These regimens are only provided to supplement the latest treatment strategies. The NCCN Guidelines are a work in progress that may be refined as often as new significant data becomes available. They are a consensus statement of its authors regarding their views of currently accepted approaches to treatment. Any clinician seeking to apply or consult any NCCN Guidelines is expected to use independent medical judgment in the context of individual clinical circumstances to determine any patient’s care or treatment. The NCCN makes no warranties of any kind whatsoever regarding their content, use, or application and disclaims any responsibility for their application or use in any -
Acute Myeloid Leukemia (AML) Treatment Regimens
Acute Myeloid Leukemia (AML) Treatment Regimens Clinical Trials: The National Comprehensive Cancer Network recommends cancer patient participation in clinical trials as the gold standard for treatment. Cancer therapy selection, dosing, administration, and the management of related adverse events can be a complex process that should be handled by an experienced healthcare team. Clinicians must choose and verify treatment options based on the individual patient; drug dose modifications and supportive care interventions should be administered accordingly. The cancer treatment regimens below may include both U.S. Food and Drug Administration-approved and unapproved indications/regimens. These regimens are only provided to supplement the latest treatment strategies. These Guidelines are a work in progress that may be refined as often as new significant data becomes available. The NCCN Guidelines® are a consensus statement of its authors regarding their views of currently accepted approaches to treatment. Any clinician seeking to apply or consult any NCCN Guidelines® is expected to use independent medical judgment in the context of individual clinical circumstances to determine any patient’s care or treatment. The NCCN makes no warranties of any kind whatsoever regarding their content, use, or application and disclaims any responsibility for their application or use in any way. uInduction Therapy1 Note: All recommendations are Category 2A unless otherwise indicated. The NCCN believes the best option for any patient with cancer is in a clinical trial and strongly encourages this option for all patients. PATIENT CRITERIA REGIMEN AND DOSING Age <60 years2-8 Days 1–3: An anthracycline (daunorubicin 60–90mg/m2 IV OR idarubicin 12mg/m2) Days 1–7: Cytarabine 100–200mg/m2 continuous IV (Category 1). -

Induction Chemotherapy with Standard-Dose Cytarabine
ORIGINAL ARTICLE Rev Hematol Mex. 2019 January-March;20(1):18-27. Induction chemotherapy with standard-dose cytarabine, daunorubicin and etoposide (7+3+7) versus high-dose cytarabine and daunorubicin in young patients with newly diagnosed acute myeloid leukemia. Quimioterapia de inducción con dosis estándar de citarabina, daunorrubicina y etopósido (7+3+7) vs dosis alta de citarabina y daunorrubicina en pacientes jóvenes con leucemia mieloide aguda recién diagnosticada. Ubaldo Rafael Valencia-Rocha,1 Roberta Demichelis-Gómez,1 Adriana López-Rosas,1 Erick Crespo-Solís2 Abstract OBJECTIVE: To compared two more intensive induction regimens than 7+3: 7+3+ eto- poside (7+3+7) versus high-dose cytarabine and daunorubicine (HiDAC-D) in patients with acute myeloid leukemia. MATERIAL AND METHOD: A comparative study of 18-55 years old patients treated at National Institute of Medical Sciences and Nutrition Salvador Zubiran, Mexico City, from November 2010 to November 2016. Induction regimens used in this study included 7+3+7 (cytarabine 100 mg/m2/day on days 1-7, daunorubicin 45 mg/m2/day on days 1-3 and etoposide 75 mg/m2/day on days 1-7), and HiDAC-D (cytarabine 3000 mg/m2/ day on days 1-3 and daunorubicin 45 mg/m /day on days 1-2). RESULTS: There were included 40 patients. In the 7+3+7 group, CR (complete remis- sion) was achieved in 76.2% of patients, while in the HiDAC-D treatment group it was 89.4% (17/19; p = 0.44). The group of patients who received the 7+3+7 regimen had 1 Hematology and Oncology De- a median overall survival (OS) of 17.2 months, while the group that received HiDAC-D partment, Instituto Nacional de Ciencias had a median OS of 18.9 months (p = 0.620). -

Daunorubicin Continuous Infusion Induces More Toxicity Than
Leukemia (2001) 15, 898–902 2001 Nature Publishing Group All rights reserved 0887-6924/01 $15.00 www.nature.com/leu Daunorubicin continuous infusion induces more toxicity than bolus infusion in acute lymphoblastic leukemia induction regimen: a randomized study M Hunault-Berger1, N Milpied2, M Bernard3, J-P Jouet4, M Delain5, B Desablens6, A Sadoun7, F Guilhot7, P Casassus8 and N Ifrah1 Division of Hematology of the University Hospital of 1Angers, 2Nantes, 3Rennes, 4Lille, 5Tours, 6Amiens, 7Poitiers and 8Bobigny, France We report the first randomized study assessing the efficacy Patients and methods and safety of daunorubicin (DNR) continuous infusion (CI) com- pared to the more conventional 30-min infusion (i.v.) in newly diagnosed adult acute lymphoblastic leukemia (ALL). Seventy- Treatment seven patients were initially randomized to receive either a 24- h CI DNR (60 mg/m2 days 2–4) (40 patients) or bolus DNR at Seventy-seven consecutive previously untreated patients with the same dosage (37 patients) with vincristine (2 mg i.v. days a non-Burkitt ALL, between the ages of 15 and 65 years, from 1, 8, 15) and oral prednisone (60 mg/m2 days 1–15), without nine hospitals, entered this study from May 1986 to May hematopoietic growth factor support, as an induction regimen. 1990. Patients with either a clinical history or electrical signs The distribution of adverse prognostic factors was comparable of coronary insufficiency or heart failure were not included. in the two-induction arm. Acute toxicity was more important 2 in the CI arm. Gram negative infection (9 vs 1 gram negative During the induction treatment, DNR (60 mg/m /day on days septicemia, P = 0.01) and infection-related deaths (6 vs 1 2 to 4) was delivered according to the initial randomization, deaths, P = NS) occurred more frequently in the CI arm during either by CI or by rapid 30-minute infusion (i.v.). -

Chronic Myelogenous Leukemia (CML) Agents – Unified Formulary
bmchp.org | 888-566-0008 wellsense.org | 877-957-1300 Pharmacy Policy Chronic Myelogenous Leukemia (CML) Agents – Unified Formulary Policy Number: 9.709 Version Number: 2.0 Version Effective Date: 9/1/2021 Product Applicability All Plan+ Products Well Sense Health Plan Boston Medical Center HealthNet Plan New Hampshire Medicaid MassHealth- MCO MassHealth- ACO Qualified Health Plans/ConnectorCare/Employer Choice Direct Senior Care Options Note: Disclaimer and audit information is located at the end of this document. Prior Authorization Policy Reference Table: Drugs that require PA No PA Bosulif® (bosutinib) PD Gleevec® # (imatinib) Iclusig® (ponatinib) Sprycel® (dasatinib) Synribo® (omacetaxine mepesuccinate) Tasigna® (nilotinib) # This is a brand-name drug with FDA “A”-rated generic equivalents. Prior authorization is required for the brand, unless a particular form of that drug (for example, tablet, capsule, or liquid) does not have an FDA “A”-rated generic equivalent. PD Preferred Drug. In general, MassHealth requires a trial of the preferred drug or clinical rationale for prescribing a non-preferred drug within a therapeutic class. Please note, for CML agents, a trial with a preferred agent is not required prior to approval of a non-preferred agent. + Plan refers to Boston Medical Center Health Plan, Inc. and its affiliates and subsidiaries offering health coverage plans to enrolled members. The Plan operates in Massachusetts under the trade name Boston Medical Center HealthNet Plan and in other states under the trade name Well Sense Health Plan. Chronic Myelogenous Leukemia (CML) Agents 1 of 6 Procedure: Approval Chronic Myelogenous Leukemia (Bosulif®, Iclusig® Synribo® (omacetaxine Diagnosis: mepesuccinate)) Acute Lymphoblastic Leukemia (Iclusig®) Approval Criteria: Prescriber provides documentation of ALL of the following: 1. -

Cancer Drug Costs for a Month of Treatment at Initial Food
Cancer drug costs for a month of treatment at initial Food and Drug Administration approval Year of FDA Monthly Cost Monthly cost (2013 Generic name Brand name(s) approval (actual $'s) $'s) Vinblastine Velban 1965 $78 $575 Thioguanine, 6-TG Thioguanine Tabloid 1966 $17 $122 Hydroxyurea Hydrea 1967 $14 $97 Cytarabine Cytosar-U, Tarabine PFS 1969 $13 $82 Procarbazine Matulane 1969 $2 $13 Testolactone Teslac 1969 $179 $1,136 Mitotane Lysodren 1970 $134 $801 Plicamycin Mithracin 1970 $50 $299 Mitomycin C Mutamycin 1974 $5 $22 Dacarbazine DTIC-Dome 1975 $29 $125 Lomustine CeeNU 1976 $10 $41 Carmustine BiCNU, BCNU 1977 $33 $127 Tamoxifen citrate Nolvadex 1977 $44 $167 Cisplatin Platinol 1978 $125 $445 Estramustine Emcyt 1981 $420 $1,074 Streptozocin Zanosar 1982 $61 $147 Etoposide, VP-16 Vepesid 1983 $181 $422 Interferon alfa 2a Roferon A 1986 $742 $1,573 Daunorubicin, Daunomycin Cerubidine 1987 $533 $1,090 Doxorubicin Adriamycin 1987 $521 $1,066 Mitoxantrone Novantrone 1987 $477 $976 Ifosfamide IFEX 1988 $1,667 $3,274 Flutamide Eulexin 1989 $213 $399 Altretamine Hexalen 1990 $341 $606 Idarubicin Idamycin 1990 $227 $404 Levamisole Ergamisol 1990 $105 $187 Carboplatin Paraplatin 1991 $860 $1,467 Fludarabine phosphate Fludara 1991 $662 $1,129 Pamidronate Aredia 1991 $507 $865 Pentostatin Nipent 1991 $1,767 $3,015 Aldesleukin Proleukin 1992 $13,503 $22,364 Melphalan Alkeran 1992 $35 $58 Cladribine Leustatin, 2-CdA 1993 $764 $1,229 Asparaginase Elspar 1994 $694 $1,088 Paclitaxel Taxol 1994 $2,614 $4,099 Pegaspargase Oncaspar 1994 $3,006 $4,713 -

Novel Drugs for Older Patients with Acute Myeloid Leukemia
Leukemia (2015) 29, 760–769 © 2015 Macmillan Publishers Limited All rights reserved 0887-6924/15 www.nature.com/leu REVIEW Novel drugs for older patients with acute myeloid leukemia G Montalban-Bravo1,2,3 and G Garcia-Manero1,3 Acute myeloid leukemia (AML) is the second most common form of leukemia and the most frequent cause of leukemia-related deaths in the United States. The incidence of AML increases with advancing age and the prognosis for patients with AML worsens substantially with increasing age. Many older patients are ineligible for intensive treatment and require other therapeutic approaches to optimize clinical outcome. To address this treatment gap, novel agents with varying mechanisms of action targeting different cellular processes are currently in development. Hypomethylating agents (azacitidine, decitabine, SGI-110), histone deacetylase inhibitors (vorinostat, pracinostat, panobinostat), FMS-like tyrosine kinase receptor-3 inhibitors (quizartinib, sorafenib, midostaurin, crenolanib), cytotoxic agents (clofarabine, sapacitabine, vosaroxin), cell cycle inhibitors (barasertib, volasertib, rigosertib) and monoclonal antibodies (gentuzumab ozogamicin, lintuzumab-Ac225) represent some of these promising new treatments. This review provides an overview of novel agents that have either completed or are currently in ongoing phase III trials in patients with previously untreated AML for whom intensive treatment is not an option. Other potential drugs in earlier stages of development will also be addressed in this review. Leukemia (2015) 29, 760–769; doi:10.1038/leu.2014.244 INTRODUCTION still lacking. In the current review we will focus on the novel Acute myeloid leukemia (AML) is a heterogeneous disease agents under development for older patients not eligible for characterized by uncontrolled clonal expansion of hematopoietic intensive treatment. -

Hyperleukocytosis and Leukostasis in Acute Myeloid Leukemia: Can a Better Understanding of the Underlying Molecular Pathophysiology Lead to Novel Treatments?
cells Review Hyperleukocytosis and Leukostasis in Acute Myeloid Leukemia: Can a Better Understanding of the Underlying Molecular Pathophysiology Lead to Novel Treatments? Jan Philipp Bewersdorf and Amer M. Zeidan * Department of Internal Medicine, Section of Hematology, Yale University School of Medicine, PO Box 208028, New Haven, CT 06520-8028, USA; [email protected] * Correspondence: [email protected]; Tel.: +1-203-737-7103; Fax: +1-203-785-7232 Received: 19 September 2020; Accepted: 15 October 2020; Published: 17 October 2020 Abstract: Up to 18% of patients with acute myeloid leukemia (AML) present with a white blood cell (WBC) count of greater than 100,000/µL, a condition that is frequently referred to as hyperleukocytosis. Hyperleukocytosis has been associated with an adverse prognosis and a higher incidence of life-threatening complications such as leukostasis, disseminated intravascular coagulation (DIC), and tumor lysis syndrome (TLS). The molecular processes underlying hyperleukocytosis have not been fully elucidated yet. However, the interactions between leukemic blasts and endothelial cells leading to leukostasis and DIC as well as the processes in the bone marrow microenvironment leading to the massive entry of leukemic blasts into the peripheral blood are becoming increasingly understood. Leukemic blasts interact with endothelial cells via cell adhesion molecules such as various members of the selectin family which are upregulated via inflammatory cytokines released by leukemic blasts. Besides their role in the development of leukostasis, cell adhesion molecules have also been implicated in leukemic stem cell survival and chemotherapy resistance and can be therapeutically targeted with specific inhibitors such as plerixafor or GMI-1271 (uproleselan).