Purva Rupeeyam of Bhela Indriya Sthana - an Explorative Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Oral Diagnosis: the Clinician's Guide
Wright An imprint of Elsevier Science Limited Robert Stevenson House, 1-3 Baxter's Place, Leith Walk, Edinburgh EH I 3AF First published :WOO Reprinted 2002. 238 7X69. fax: (+ 1) 215 238 2239, e-mail: [email protected]. You may also complete your request on-line via the Elsevier Science homepage (http://www.elsevier.com). by selecting'Customer Support' and then 'Obtaining Permissions·. British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Library of Congress Cataloging in Publication Data A catalog record for this book is available from the Library of Congress ISBN 0 7236 1040 I _ your source for books. journals and multimedia in the health sciences www.elsevierhealth.com Composition by Scribe Design, Gillingham, Kent Printed and bound in China Contents Preface vii Acknowledgements ix 1 The challenge of diagnosis 1 2 The history 4 3 Examination 11 4 Diagnostic tests 33 5 Pain of dental origin 71 6 Pain of non-dental origin 99 7 Trauma 124 8 Infection 140 9 Cysts 160 10 Ulcers 185 11 White patches 210 12 Bumps, lumps and swellings 226 13 Oral changes in systemic disease 263 14 Oral consequences of medication 290 Index 299 Preface The foundation of any form of successful treatment is accurate diagnosis. Though scientifically based, dentistry is also an art. This is evident in the provision of operative dental care and also in the diagnosis of oral and dental diseases. While diagnostic skills will be developed and enhanced by experience, it is essential that every prospective dentist is taught how to develop a structured and comprehensive approach to oral diagnosis. -

Guideline # 18 ORAL HEALTH
Guideline # 18 ORAL HEALTH RATIONALE Dental caries, commonly referred to as “tooth decay” or “cavities,” is the most prevalent chronic health problem of children in California, and the largest single unmet health need afflicting children in the United States. A 2006 statewide oral health needs assessment of California kindergarten and third grade children conducted by the Dental Health Foundation (now called the Center for Oral Health) found that 54 percent of kindergartners and 71 percent of third graders had experienced dental caries, and that 28 percent and 29 percent, respectively, had untreated caries. Dental caries can affect children’s growth, lead to malocclusion, exacerbate certain systemic diseases, and result in significant pain and potentially life-threatening infections. Caries can impact a child’s speech development, learning ability (attention deficit due to pain), school attendance, social development, and self-esteem as well.1 Multiple studies have consistently shown that children with low socioeconomic status (SES) are at increased risk for dental caries.2,3,4 Child Health Disability and Prevention (CHDP) Program children are classified as low socioeconomic status and are likely at high risk for caries. With regular professional dental care and daily homecare, most oral disease is preventable. Almost one-half of the low-income population does not obtain regular dental care at least annually.5 California children covered by Medicaid (Medi-Cal), ages 1-20, rank 41 out of all 50 states and the District of Columbia in receiving any preventive dental service in FY2011.6 Dental examinations, oral prophylaxis, professional topical fluoride applications, and restorative treatment can help maintain oral health. -

Oral Lesions in Sjögren's Syndrome
Med Oral Patol Oral Cir Bucal. 2018 Jul 1;23 (4):e391-400. Oral lesions in Sjögren’s syndrome patients Journal section: Oral Medicine and Pathology doi:10.4317/medoral.22286 Publication Types: Review http://dx.doi.org/doi:10.4317/medoral.22286 Oral lesions in Sjögren’s syndrome: A systematic review Julia Serrano 1, Rosa-María López-Pintor 1, José González-Serrano 1, Mónica Fernández-Castro 2, Elisabeth Casañas 1, Gonzalo Hernández 1 1 Department of Oral Medicine and Surgery, School of Dentistry, Complutense University, Madrid, Spain 2 Rheumatology Service, Hospital Infanta Sofía, Madrid, Spain Correspondence: Departamento de Especialidades Clínicas Odontológicas Facultad de Odontología Universidad Complutense de Madrid Plaza Ramón y Cajal s/n, 28040 Madrid. Spain [email protected] Serrano J, López-Pintor RM, González-Serrano J, Fernández-Castro M, Casañas E, Hernández G. Oral lesions in Sjögren’s syndrome: A system- atic review. Med Oral Patol Oral Cir Bucal. 2018 Jul 1;23 (4):e391-400. Received: 18/11/2017 http://www.medicinaoral.com/medoralfree01/v23i4/medoralv23i4p391.pdf Accepted: 09/05/2018 Article Number: 22291 http://www.medicinaoral.com/ © Medicina Oral S. L. C.I.F. B 96689336 - pISSN 1698-4447 - eISSN: 1698-6946 eMail: [email protected] Indexed in: Science Citation Index Expanded Journal Citation Reports Index Medicus, MEDLINE, PubMed Scopus, Embase and Emcare Indice Médico Español Abstract Background: Sjögren’s syndrome (SS) is an autoimmune disease related to two common symptoms: dry mouth and eyes. Although, xerostomia and hyposialia have been frequently reported in these patients, not many studies have evaluated other oral manifestations. -
Addisonian Pigmentation of the Oral Mucosa
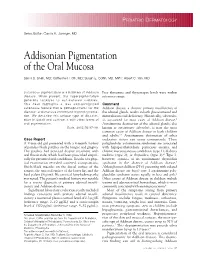
PEDIATRIC DERMATOLOGY Series Editor: Camila K. Janniger, MD Addisonian Pigmentation of the Oral Mucosa Samir S. Shah, MD; Catherine H. Oh, MD; Susan E. Coffin, MD, MPH; Albert C. Yan, MD Cutaneous pigmentation is a hallmark of Addison Free thyroxine and thyrotropin levels were within disease. When present, the hyperpigmentation reference range. generally localizes to sun-exposed surfaces. This case highlights a less well-recognized Comment cutaneous feature that is pathognomonic for the Addison disease, a chronic primary insufficiency of disease: oral mucous membrane hyperpigmenta- the adrenal glands, results in both glucocorticoid and tion. We describe this unique type of discolor- mineralocorticoid deficiency. Historically, tuberculo- ation in detail and contrast it with other forms of sis accounted for most cases of Addison disease.1 oral pigmentation. Autoimmune destruction of the adrenal glands, also Cutis. 2005;76:97-99. known as autoimmune adrenalitis, is now the most common cause of Addison disease in both children and adults.2,3 Autoimmune destruction of other Case Report endocrine tissues can occur concurrently. These A 9-year-old girl presented with a 4-month history polyglandular autoimmune syndromes are associated of painless black patches on the tongue and gingiva. with hypoparathyroidism, pernicious anemia, and The patches had persisted despite treatment with chronic mucocutaneous candidiasis (type 1); diabetes oral fluconazole, which had been prescribed empiri- mellitus (type 2); or thyroiditis (type 3).4 Type 3, cally for presumed oral candidiasis. Results of a phys- however, consists of an autoimmune thyroiditis ical examination revealed scattered, asymptomatic, syndrome in the absence of Addison disease.5 bluish-black macules on the dorsal surface of the Although most children (75%) presenting with isolated tongue, the mucosal surface of the lower lip, and the Addison disease are boys,6 type 1 autoimmune poly- hard palate (Figure). -

The OHNEP Interprofessional Oral Health Faculty Toolkit
The OHNEP Interprofessional Oral Health Faculty Toolkit Adult-Gerontology Nurse Practitioner Program CURRICULUM INTEGRATION OF INTERPROFESSIONAL ORAL HEALTH CORE COMPETENCIES: • Adult-Gerontology Health Assessment • Adult-Gerontology Health Promotion • Adult-GerontologyPrimary Care • Resources © Oral Health Nursing Education and Practice (OHNEP) INTRODUCTION The Oral Health Nursing Education and Practice (OHNEP) program has developed an Interprofessional Oral Health Faculty Tool Kit to S! provide you with user friendly curriculum templates and teaching-learning resources to use when integrating oral health and its links to ! overall health in your Adult-Gerontology Nurse Practitioner program. ! Oral health and its relation to overall health has been identified as an important population health issue. Healthy People 2020 (2011), the IOM Reports, Advancing Oral Health in America (2011) and Building Workforce Capacity in Oral Health (2011), as well as the IPEC Competencies ! (2011), challenged HRSA to develop interprofessional oral health core competencies for primary care providers. Publication of the report, ! Integrating Oral Health in Primary Care Practice (2014), reflects those interprofessional oral health competencies that can be used by Adult- Gerontology Nurse Practitioners for faculty development, curriculum integration and establishment of “best practices” in clinical settings. ! The HRSA interprofessional oral health core competencies, the IPEC competencies and the NONPF core competencies provide the framework for the curriculum templates and resources. Exciting teaching-learning strategies that take students from Exposure to Immersion to Competence can begin in the classroom, link to simulated or live clinical experiences and involve community-based service learning, advocacy and policy initiatives as venues you can readily use to integrate oral health into your existing primary care curriculum. -

Adverse Effects of Medications on Oral Health
Adverse Effects of Medications on Oral Health Dr. James Krebs, BS Pharm, MS, PharmD Director of Experiential Education College of Pharmacy, University of New England Presented by: Rachel Foster PharmD Candidate, Class of 2014 University of New England October 2013 Objectives • Describe the pathophysiology of various medication-related oral reactions • Recognize the signs and symptoms associated with medication-related oral reactions • Identify the populations associated with various offending agents • Compare the treatment options for medication-related oral reactions Medication-related Oral Reactions • Stomatitis • Oral Candidiasis • Burning mouth • Gingival hyperplasia syndrome • Alterations in • Glossitis salivation • Erythema • Alterations in taste Multiforme • Halitosis • Oral pigmentation • Angioedema • Tooth discoloration • Black hairy tongue Medication-related Stomatitis • Clinical presentation – Aphthous-like ulcers, mucositis, fixed-drug eruption, lichen planus1,2 – Open sores in the mouth • Tongue, gum line, buccal membrane – Patient complaint of soreness or burning http://www.virtualmedicalcentre.com/diseases/oral-mucositis-om/92 0 http://www.virtualmedicalcentre.com/diseases/oral-mucositis-om/920 Medication-related Stomatitis • Offending agents1,2 Medication Indication Patient Population Aspirin •Heart health • >18 years old •Pain reliever • Cardiac patients NSAIDs (i.e. Ibuprofen, •Headache General population naproxen) •Pain reliever •Fever reducer Chemotherapy (i.e. •Breast cancer •Oncology patients methotrexate, 5FU, •Colon -
A Concise Guide to Treating Painful Oral Lesions
Drugs Used to Treat Osteoporosis and Bone Cancer Perio & Implant Centers The Team for of the Monterey Bay (831) 648-8800 Jochen P. Pechak, DDS, MSD in Silicon Valley (408) 738-3423 Which May Cause Osteonecrosis of the Jaws mobile: www.DrPechakapp.com he many bisphosphonates and monoclonal antibodies which are used to treat osteoporosis and bone cancer often web: GumsRus.com causeDrugsDrugs osteonecrosis Used Used of the to jaws.to Treat AsTreat dental clinicians,Osteoporosis Osteoporosis it is important that and andwe are Bone awareBone of this Cancers Cancers side effect before Ttreating our patients who are taking these drugs. The tables below summarize these drugs, the route these drugs are administered, andWhich Whichtheir likelihood May May of causing Cause Cause osteonecrosis Osteonecrosis Osteonecrosis of the jaws as reported byof of Dr. the theRobert Jaws JawsMarx at the University of Miami Division of Oral and Maxillofacial Surgery. PDL tm Osteoporosis Drugs Drugs Osteoporosis Used to Treat Drugs Osteoporosis PerioDontaLetter Jochen P. Pechak, DDS, MSD, Periodontics and Implant Dentistry Spring DrugDrug ClassificationClassification ActionAction DoseDose RouteRoute %% of of ReportedReported CasesCases of of OsteonecrosisOsteonecrosis AlendronateAlendronate BisphosphonateBisphosphonate OsteoclastOsteoclast 7070 mg/wk mg/wk OralOral 8282%% From Our Office A Concise Guide to Treating (Fosamax(Fosamax ToxicityToxicity to Yours... Generic)Generic) Painful Oral Lesions ResidronateResidronate BisphosphonateBisphosphonate OsteoclastOsteoclast 3535 mg/wk mg/wk OralOral 1%1% As dentists specializing in treat- (Actonel Toxicity (Actonel Toxicity ment of diseases of the oral cavity atients present frequently with Treating Cold Sores Atelvia)Atelvia) and associated structures, we are painful oral lesions. They are often also called upon to treat pain- IbandronateIbandronate BisphosphonateBisphosphonate OsteoclastOsteoclast 150150 mg/mos mg/mos OralOral 1%1% usually not serious, but patients And Canker Sores (Boniva) Toxicity IV ful oral lesions in the mouth. -

Hairy Tongue, Geographic Tongue, Scrotal Tongue and Systemic Connections: Clinical Images and an Overview
CASE REPORT Hairy tongue, geographic tongue, scrotal tongue and systemic connections: clinical images and an overview Cinzia Casu, DDS1, Maria Giulia Nosotti, RDH2, Antonia Sinesi, RDH2, Giovanna Mosaico, RDH2 Casu C, Nosotti MG, Sinesi A, et al. Hairy tongue, geographic tongue, condition, predominantly asymptomatic. Clinically, it is characterized by scrotal tongue and systemic connections: clinical images and an overview. fissures with a depth of up to 6 mm that extend along the dorsal and/or Dentist Case Rep. 2019;3(1):01-03. lateral sides of the tongue. These benign entities are connected with systemic disease (psoriasis, diabetes, hypertension and GT; tumors, radiant therapies ABSTRACT and BHT; fungal infections and Merkesson-Rosenthal syndrome and ST). Black Hairy Tongue (BHT) is a benign condition, caused by a defect of keratin Although an association between elevated IgE and migrant glossitis has desquamation over lingual papillae and its discoloration is caused by the been documented, associations between the three lingual conditions and the presence of porphyrin-producing chromogenic bacteria or yeast. Geographic presence of allergy are unclear. We would like to present a case in which the Tongue (GT) is characterized by a central erythematous zone consisting of 3 conditions were present in the same tongue of a female patient with allergic atrophy of the filiform papillae, whereas the white zone shows regenerating rhinitis and calcium deficiency. filiform papillae along with keratin. Scrotal Tongue (ST) is a common Key Words: Geographic tongue; scrotal tongue; black hairy tongue he tongue is considered the most complex organ of the body and a very Scrotal Tongue (ST) is a frequent condition in the population, Timportant structure in the oral cavity. -

Common Superficial Tongue Lesions
ENT Common Superficial Tongue Lesions ANURADHA SUNIL*, JACOB KURIEN**, ARCHANA MUKUNDA†, ASHIK BIN BASHEER‡, DEEPTHI# ABSTRACT The tongue is an important structure in the oral cavity and the strongest muscular organ in the body involved in critical functions of taste, speaking, chewing and swallowing. The basic anatomy of tongue is such that unless scrupulous dental hygiene is followed it may lead to pathological lesions. Since the earliest days of medicine, the tongue has been considered a good reflection of systemic diseases. Assessment of the tongue has historically been an important part of a clinical medical examination as many pathological lesions are seen exclusively on the tongue. Lesions occurring on the tongue are vast and range from developmental disorders to infections to idiopathic lesions to malignancies; some lesions may be clues to the underlying systemic illness. General practitioners/physicians and dentists regularly come across such lesions on tongue in their day-to-day practice. A basic and through knowledge of the commonly occurring lesions on the tongue may enlighten the general practitioner in regards to the diagnosis and thereby help in the most effective management of the patients. Uniform diagnostic criteria may heighten the level of clinical diagnosis. Most lesions occurring on tongue heal fast owing to the rich blood supply and if a lesion fails to heal within 10-14 days it must be biopsied and/or further evaluation is necessary for an appropriate diagnosis. Keywords: General practitioner, superficial tongue lesions, squamous cell carcinoma of tongue, pyogenic granuloma of tongue, tuberculous ulcers on tongue, aphthous ulcers, pemphigus vulgaris lesions on tongue, lichenoid lesions on tongue ral health highlights the relationship between Knowledge of clinical characteristics such as size, oral and overall health, emphasizing that oral location, surface morphology, color, pain and duration Ohealth involves more than dentition. -

Common Icd-10 Dental Codes
COMMON ICD-10 DENTAL CODES SERVICE PROVIDERS SHOULD BE AWARE THAT AN ICD-10 CODE IS A DIAGNOSTIC CODE. i.e. A CODE GIVING THE REASON FOR A PROCEDURE; SO THERE MIGHT BE MORE THAN ONE ICD-10 CODE FOR A PARTICULAR PROCEDURE CODE AND THE SERVICE PROVIDER NEEDS TO SELECT WHICHEVER IS THE MOST APPROPRIATE. ICD10 Code ICD-10 DESCRIPTOR FROM WHO (complete) OWN REFERENCE / INTERPRETATION/ CIRCUM- STANCES IN WHICH THESE ICD-10 CODES MAY BE USED TIP:If you are viewing this electronically, in order to locate any word in the document, click CONTROL-F and type in word you are looking for. K00 Disorders of tooth development and eruption Not a valid code. Heading only. K00.0 Anodontia Congenitally missing teeth - complete or partial K00.1 Supernumerary teeth Mesiodens K00.2 Abnormalities of tooth size and form Macr/micro-dontia, dens in dente, cocrescence,fusion, gemination, peg K00.3 Mottled teeth Fluorosis K00.4 Disturbances in tooth formation Enamel hypoplasia, dilaceration, Turner K00.5 Hereditary disturbances in tooth structure, not elsewhere classified Amylo/dentino-genisis imperfecta K00.6 Disturbances in tooth eruption Natal/neonatal teeth, retained deciduous tooth, premature, late K00.7 Teething syndrome Teething K00.8 Other disorders of tooth development Colour changes due to blood incompatability, biliary, porphyria, tetyracycline K00.9 Disorders of tooth development, unspecified K01 Embedded and impacted teeth Not a valid code. Heading only. K01.0 Embedded teeth Distinguish from impacted tooth K01.1 Impacted teeth Impacted tooth (in contact with another tooth) K02 Dental caries Not a valid code. Heading only. -

A Patient Having Recurrent Aphtous Stomatitis After Three Years Of
ion Res ict ea d rc d h A & f o T Journal of l h a e n r r a u p Unal et al., J Addict Res Ther 2014, 5:4 o y J 10.4172/2155-6105.1000202 ISSN: 2155-6105 Addiction Research & Therapy DOI: Case Report Open Access A Patient Having Recurrent Aphtous Stomatitis After Three Years of Smoking Cessation; A Case Report and Review of Literature Mustafa Unal1, Bektas Murat Yalcin2* and Onur Ozturk3 1 Department of Family Practice, Asistant Professor, Dr.Ondokuz Mayis University Medical Faculty, Turkey 2 Department of Family Practice, Associate Professor, Dr. Ondokuz Mayis University Medical Faculty, Turkey 3Family Physician, Samsun Education and Specialization State Hospital, Turkey *Corresponding author: Bektas Murat YALCIN, Associate Professor, Ondokuz Mayıs University medical Faculty Department of Family Medicine Kurupelit/Samsun, Turkey, Tel: 0362 3121919-346 ; E-mail: [email protected] Received date: December 18, 2014, Accepted date: December 29, 2014, Publication date: December 31, 2014 Copyright: © 2014 Unal M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Cigarette smoking is the foremost health risk issue affecting individuals of all age groups globally. It is the most important causes of the preventable deaths and diseases. Aware of these facts many smokers wish to quit. However smoking cessation is though for smokers who experiences many unpleasant and troublesome physiological or psychological problems. After cessation oral ulcers and other oral aphtous lesions which are considered as mild and expected to disappear in time, can be seen. -

The Pseudolesions of the Oral Mucosa: Differential Diagnosis and Related Systemic Conditions
applied sciences Review The Pseudolesions of the Oral Mucosa: Differential Diagnosis and Related Systemic Conditions Fedora della Vella 1,* , Dorina Lauritano 2 , Carlo Lajolo 3 , Alberta Lucchese 4, Dario Di Stasio 4 , Maria Contaldo 4 , Rosario Serpico 4 and Massimo Petruzzi 1,* 1 Interdisciplinary Department of Medicine, University of Bari “Aldo Moro”, 70124 Bari, Italy 2 School of Medicine and Surgery, University of Milano-Bicocca, 20900 Monza, Italy; [email protected] 3 Department of Head and Neck, Oral Surgery and Implantology Unit, University Cattolica del Sacro Cuore, 00168 Rome, Italy; [email protected] 4 Multidisciplinary Department of Medical-Surgical and Dental Specialties, University of Campania “Luigi Vanvitelli”, 80138 Naples, Italy; [email protected] (A.L.); [email protected] (D.D.S.); [email protected] (M.C.); [email protected] (R.S.) * Correspondence: [email protected] (F.d.V.); [email protected] (M.P.); Tel.: +39-0805478388 (F.d.V.) Received: 7 May 2019; Accepted: 10 June 2019; Published: 13 June 2019 Abstract: Pseudolesions are defined as physiological or paraphysiological changes of the oral normal anatomy that can easily be misdiagnosed for pathological conditions such as potentially malignant lesions, infective and immune diseases, or neoplasms. Pseudolesions do not require treatment and a surgical or pharmacological approach can constitute an overtreatment indeed. This review aims to describe the most common pseudolesions of oral soft tissues, their possible differential diagnosis and eventual related systemic diseases or syndromes. The pseudolesions frequently observed in clinical practice and reported in literature include Fordyce granules, leukoedema, geographic tongue, fissured tongue, sublingual varices, lingual fimbriae, vallate papillae, white and black hairy tongue, Steno’s duct hypertrophy, lingual tonsil, white sponge nevus, racial gingival pigmentation, lingual thyroid, and eruptive cyst.