New Anatomical Classification of the Axilla with Implications for Sentinel
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Microlymphatic Surgery for the Treatment of Iatrogenic Lymphedema
Microlymphatic Surgery for the Treatment of Iatrogenic Lymphedema Corinne Becker, MDa, Julie V. Vasile, MDb,*, Joshua L. Levine, MDb, Bernardo N. Batista, MDa, Rebecca M. Studinger, MDb, Constance M. Chen, MDb, Marc Riquet, MDc KEYWORDS Lymphedema Treatment Autologous lymph node transplantation (ALNT) Microsurgical vascularized lymph node transfer Iatrogenic Secondary Brachial plexus neuropathy Infection KEY POINTS Autologous lymph node transplant or microsurgical vascularized lymph node transfer (ALNT) is a surgical treatment option for lymphedema, which brings vascularized, VEGF-C producing tissue into the previously operated field to promote lymphangiogenesis and bridge the distal obstructed lymphatic system with the proximal lymphatic system. Additionally, lymph nodes with important immunologic function are brought into the fibrotic and damaged tissue. ALNT can cure lymphedema, reduce the risk of infection and cellulitis, and improve brachial plexus neuropathies. ALNT can also be combined with breast reconstruction flaps to be an elegant treatment for a breast cancer patient. OVERVIEW: NATURE OF THE PROBLEM Clinically, patients develop firm subcutaneous tissue, progressing to overgrowth and fibrosis. Lymphedema is a result of disruption to the Lymphedema is a common chronic and progres- lymphatic transport system, leading to accumula- sive condition that can occur after cancer treat- tion of protein-rich lymph fluid in the interstitial ment. The reported incidence of lymphedema space. The accumulation of edematous fluid mani- varies because of varying methods of assess- fests as soft and pitting edema seen in early ment,1–3 the long follow-up required for diagnosing lymphedema. Progression to nonpitting and irre- lymphedema, and the lack of patient education versible enlargement of the extremity is thought regarding lymphedema.4 In one 20-year follow-up to be the result of 2 mechanisms: of patients with breast cancer treated with mastec- 1. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Human Anatomy As Related to Tumor Formation Book Four
SEER Program Self Instructional Manual for Cancer Registrars Human Anatomy as Related to Tumor Formation Book Four Second Edition U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutesof Health SEER PROGRAM SELF-INSTRUCTIONAL MANUAL FOR CANCER REGISTRARS Book 4 - Human Anatomy as Related to Tumor Formation Second Edition Prepared by: SEER Program Cancer Statistics Branch National Cancer Institute Editor in Chief: Evelyn M. Shambaugh, M.A., CTR Cancer Statistics Branch National Cancer Institute Assisted by Self-Instructional Manual Committee: Dr. Robert F. Ryan, Emeritus Professor of Surgery Tulane University School of Medicine New Orleans, Louisiana Mildred A. Weiss Los Angeles, California Mary A. Kruse Bethesda, Maryland Jean Cicero, ART, CTR Health Data Systems Professional Services Riverdale, Maryland Pat Kenny Medical Illustrator for Division of Research Services National Institutes of Health CONTENTS BOOK 4: HUMAN ANATOMY AS RELATED TO TUMOR FORMATION Page Section A--Objectives and Content of Book 4 ............................... 1 Section B--Terms Used to Indicate Body Location and Position .................. 5 Section C--The Integumentary System ..................................... 19 Section D--The Lymphatic System ....................................... 51 Section E--The Cardiovascular System ..................................... 97 Section F--The Respiratory System ....................................... 129 Section G--The Digestive System ......................................... 163 Section -

Consensus Guideline on the Management of the Axilla in Patients with Invasive/In-Situ Breast Cancer
- Official Statement - Consensus Guideline on the Management of the Axilla in Patients With Invasive/In-Situ Breast Cancer Purpose To outline the management of the axilla for patients with invasive and in-situ breast cancer. Associated ASBrS Guidelines or Quality Measures 1. Performance and Practice Guidelines for Sentinel Lymph Node Biopsy in Breast Cancer Patients – Revised November 25, 2014 2. Performance and Practice Guidelines for Axillary Lymph Node Dissection in Breast Cancer Patients – Approved November 25, 2014 3. Quality Measure: Sentinel Lymph Node Biopsy for Invasive Breast Cancer – Approved November 4, 2010 4. Prior Position Statement: Management of the Axilla in Patients With Invasive Breast Cancer – Approved August 31, 2011 Methods A literature review inclusive of recent randomized controlled trials evaluating the use of sentinel lymph node surgery and axillary lymph node dissection for invasive and in-situ breast cancer as well as the pathologic review of sentinel lymph nodes and indications for axillary radiation was performed. This is not a complete systematic review but rather, a comprehensive review of recent relevant literature. A focused review of non-randomized controlled trials was then performed to develop consensus guidance on management of the axilla in scenarios where randomized controlled trials data is lacking. The ASBrS Research Committee developed a consensus document, which was reviewed and approved by the ASBrS Board of Directors. Summary of Data Reviewed Recommendations Based on Randomized Controlled -

Anatomy and Physiology in Relation to Compression of the Upper Limb and Thorax
Clinical REVIEW anatomy and physiology in relation to compression of the upper limb and thorax Colin Carati, Bren Gannon, Neil Piller An understanding of arterial, venous and lymphatic flow in the upper body in normal limbs and those at risk of, or with lymphoedema will greatly improve patient outcomes. However, there is much we do not know in this area, including the effects of compression upon lymphatic flow and drainage. Imaging and measuring capabilities are improving in this respect, but are often expensive and time-consuming. This, coupled with the unknown effects of individual, diurnal and seasonal variances on compression efficacy, means that future research should focus upon ways to monitor the pressure delivered by a garment, and its effects upon the fluids we are trying to control. More is known about the possible This paper will describe the vascular Key words effects of compression on the anatomy of the upper limb and axilla, pathophysiology of lymphoedema when and will outline current understanding of Anatomy used on the lower limbs (Partsch and normal and abnormal lymph drainage. It Physiology Junger, 2006). While some of these will also explain the mechanism of action Lymphatics principles can be applied to guide the use of compression garments and will detail Compression of compression on the upper body, it is the effects of compression on fluid important that the practitioner is movement. knowledgeable about the anatomy and physiology of the upper limb, axilla and Vascular drainage of the upper limb thorax, and of the anatomical and vascular It is helpful to have an understanding of Little evidence exists to support the differences that exist between the upper the vascular drainage of the upper limb, use of compression garments in the and lower limb, so that the effects of these since the lymphatic drainage follows a treatment of lymphoedema, particularly differences can be considered when using similar course (Figure 1). -

Pectoral Region and Axilla Doctors Notes Notes/Extra Explanation Editing File Objectives
Color Code Important Pectoral Region and Axilla Doctors Notes Notes/Extra explanation Editing File Objectives By the end of the lecture the students should be able to : Identify and describe the muscles of the pectoral region. I. Pectoralis major. II. Pectoralis minor. III. Subclavius. IV. Serratus anterior. Describe and demonstrate the boundaries and contents of the axilla. Describe the formation of the brachial plexus and its branches. The movements of the upper limb Note: differentiate between the different regions Flexion & extension of Flexion & extension of Flexion & extension of wrist = hand elbow = forearm shoulder = arm = humerus I. Pectoralis Major Origin 2 heads Clavicular head: From Medial ½ of the front of the clavicle. Sternocostal head: From; Sternum. Upper 6 costal cartilages. Aponeurosis of the external oblique muscle. Insertion Lateral lip of bicipital groove (humerus)* Costal cartilage (hyaline Nerve Supply Medial & lateral pectoral nerves. cartilage that connects the ribs to the sternum) Action Adduction and medial rotation of the arm. Recall what we took in foundation: Only the clavicular head helps in flexion of arm Muscles are attached to bones / (shoulder). ligaments / cartilage by 1) tendons * 3 muscles are attached at the bicipital groove: 2) aponeurosis Latissimus dorsi, pectoral major, teres major 3) raphe Extra Extra picture for understanding II. Pectoralis Minor Origin From 3rd ,4th, & 5th ribs close to their costal cartilages. Insertion Coracoid process (scapula)* 3 Nerve Supply Medial pectoral nerve. 4 Action 1. Depression of the shoulder. 5 2. Draw the ribs upward and outwards during deep inspiration. *Don’t confuse the coracoid process on the scapula with the coronoid process on the ulna Extra III. -

Medical Term Lay Term(S)
MEDICAL TERM LAY TERM(S) ABDOMINAL Pertaining to body cavity below diaphragm which contains stomach, intestines, liver, and other organs ABSORB Take up fluids, take in ACIDOSIS Condition when blood contains more acid than normal ACUITY Clearness, keenness, esp. of vision - airways ACUTE New, recent, sudden ADENOPATHY Swollen lymph nodes (glands) ADJUVANT Helpful, assisting, aiding ADJUVANT Added treatment TREATMENT ANTIBIOTIC Drug that kills bacteria and other germs ANTIMICROBIAL Drug that kills bacteria and other germs ANTIRETROVIRAL Drug that inhibits certain viruses ADVERSE EFFECT Negative side effect ALLERGIC REACTION Rash, trouble breathing AMBULATE Walk, able to walk -ATION -ORY ANAPHYLAXIS Serious, potentially life threatening allergic reaction ANEMIA Decreased red blood cells; low red blood cell count ANESTHETIC A drug or agent used to decrease the feeling of pain or eliminate the feeling of pain by general putting you to sleep ANESTHETIC A drug or agent used to decrease the feeling of pain or by numbing an area of your body, local without putting you to sleep ANGINA Pain resulting from insufficient blood to the heart (ANGINA PECTORIS) ANOREXIA Condition in which person will not eat; lack of appetite ANTECUBITAL Area inside the elbow ANTIBODY Protein made in the body in response to foreign substance; attacks foreign substance and protects against infection ANTICONVULSANT Drug used to prevent seizures ANTILIPIDEMIC A drug that decreases the level of fat(s) in the blood ANTITUSSIVE A drug used to relieve coughing ARRHYTHMIA Any change from the normal heartbeat (abnormal heartbeat) ASPIRATION Fluid entering lungs ASSAY Lab test ASSESS To learn about ASTHMA A lung disease associated with tightening of the air passages ASYMPTOMATIC Without symptoms AXILLA Armpit BENIGN Not malignant, usually without serious consequences, but with some exceptions e.g. -

Multilingual Cancer Glossary French | Français A
Multilingual Cancer Glossary French | Français www.petermac.org/multilingualglossary email: [email protected] www.petermac.org/cancersurvivorship The Multilingual Cancer Glossary has been developed Disclaimer to provide language professionals working in the The information contained within this booklet is given cancer field with access to accurate and culturally as a guide to help support patients, carers, families and and linguistically appropriate cancer terminology. The consumers understand their healthand support their glossary addresses the known risk of mistranslation of health decision making process. cancer specific terms in resources in languages other than English. The information given is not fully comprehensive, nor is it intended to be used to diagnose, treat, cure or prevent Acknowledgements any medical conditions. If you require medical assistance This project is a Cancer Australia Supporting people please contact your local doctor or call Peter Mac on with cancer Grant initiative, funded by the Australian 03 8559 5000. Government. To the maximum extent permitted by law, Peter The Australian Cancer Survivorship Centre, A Richard Pratt Mac and its employees, volunteers and agents legacy would like to thank and acknowledge all parties are not liable to any person in contract, tort who contributed to the development of the glossary. (including negligence or breach of statutory duty) or We particularly thank members of the project steering otherwise for any direct or indirect loss, damage, committee and working group, language professionals cost or expense arising out of or in connection with and community organisations for their insights and that person relying on or using any information or assistance. advice provided in this booklet or incorporated into it by reference. -

Intractable Shoulder Dystocia: a Posterior Axilla Maneuver May Save the Day
Intractable shoulder dystocia: A posterior axilla maneuver may save the day My preferred posterior axilla maneuver is the Menticoglou maneuver. Here, a look at your options and steps to delivery. Robert L. Barbieri, MD houlder dystocia is an unpredictable 7. delivering the posterior arm obstetric emergency that challenges 8. considering the Gaskin all-four maneuver. S all obstetricians and midwives. In response to a shoulder dystocia emergency, When initial management most clinicians implement a sequence of steps are not enough IN THIS well-practiced steps that begin with early If this sequence of steps does not result in ARTICLE recognition of the problem, clear communi- successful vaginal delivery, additional op- cation of the emergency with delivery room tions include: clavicle fracture, cephalic re- staff, and a call for help to available clinicians. placement followed by cesarean delivery Menticoglou Management steps may include: (Zavanelli maneuver), symphysiotomy, or maneuver 1. instructing the mother to stop pushing and fundal pressure combined with a rotational page 18 moving the mother’s buttocks to the edge maneuver. Another simple intervention that of the bed is not discussed widely in medical textbooks Importance of 2. ensuring there is not a tight nuchal cord or taught during training is the posterior simulation 3. committing to avoiding the use of excessive axilla maneuver. page 20 force on the fetal head and neck 4. considering performing an episiotomy 5. performing the McRoberts maneuver com- Posterior axilla maneuvers bined with suprapubic pressure Varying posterior axilla maneuvers have 6. using a rotational maneuver, such as the been described by many expert obstetri- Woods maneuver or the Rubin maneuver cians, including Willughby (17th Cen- tury),1 Holman (1963),2 Schramm (1983),3 4 Dr. -
Hand and Arm Guidelines After Your Axillary Lymph Node Dissection
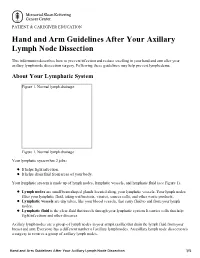
PATIENT & CAREGIVER EDUCATION Hand and Arm Guidelines After Your Axillary Lymph Node Dissection This information describes how to prevent infection and reduce swelling in your hand and arm after your axillary lymph node dissection surgery. Following these guidelines may help prevent lymphedema. About Your Lymphatic System Figure 1. Normal lymph drainage Figure 1. Normal lymph drainage Your lymphatic system has 2 jobs: It helps fight infection. It helps drain fluid from areas of your body. Your lymphatic system is made up of lymph nodes, lymphatic vessels, and lymphatic fluid (see Figure 1). Lymph nodes are small bean-shaped glands located along your lymphatic vessels. Your lymph nodes filter your lymphatic fluid, taking out bacteria, viruses, cancer cells, and other waste products. Lymphatic vessels are tiny tubes, like your blood vessels, that carry fluid to and from your lymph nodes. Lymphatic fluid is the clear fluid that travels through your lymphatic system. It carries cells that help fight infections and other diseases. Axillary lymph nodes are a group of lymph nodes in your armpit (axilla) that drain the lymph fluid from your breast and arm. Everyone has a different number of axillary lymph nodes. An axillary lymph node dissection is a surgery to remove a group of axillary lymph nodes. Hand and Arm Guidelines After Your Axillary Lymph Node Dissection 1/5 About Lymphedema Sometimes, removing lymph nodes can make it hard for your lymphatic system to drain properly. If this happens, lymphatic fluid can build up in the area where the lymph nodes were removed. This extra fluid causes swelling called lymphedema. -

Nasal, Axillary, and Perineal Carriage of Staphylococcus Aureus Among
J Clin Pathol 1991;44:681-684 681 Nasal, axillary, and perineal carriage of aureus among women: Staphylococcus J Clin Pathol: first published as 10.1136/jcp.44.8.681 on 1 August 1991. Downloaded from Identification of strains producing epidermolytic toxin S J Dancer, W C Noble Abstract by which the mother may also become infec- Following two outbreaks of staphylococ- ted, leading to the development of a breast cal scalded skin syndrome in a maternity abscess. '0 unit, 500 pregnant women attending an S aureus of certain phage groups tend to be antenatal clinic were screened for car- associated with particular skin diseases." A riage of epidermolytic toxin producing rare neonatal disease called the staphylococcal Staphylococcus aureus. Nasal, axillary, scalded skin syndrome and the related milder, and perineal swabs were collected from but more common form, pemphigus neo- women whose gestational ages ranged natorum, are generally caused by strains from 12-40 weeks. Isolates of S aureus belonging to phage group H1."2 3 Both these were purified, phage typed, and tested for conditions fall within a continuous spectrum methicillin sensitivity and production of which ranges from localised bullous impetigo epidermolytic toxin. The results showed to a generalised epidermolysis of the skin that 164 (33%) women carried S aureus; resembling widespread first degree burns.'4 of these, 100 (61%) were from the nose The causative strain of S aureus colonising and three (2%) from axillae, but 41 sites such as nose or umbilical stump in neo- (25%) strains were isolated from the nates"5 produces epidermolytic toxins which perineum alone. -

Mondor's Disease: a Review of the Literature
doi: 10.2169/internalmedicine.0495-17 Intern Med 57: 2607-2612, 2018 http://internmed.jp 【 REVIEW ARTICLE 】 Mondor’s Disease: A Review of the Literature Masayuki Amano 1 and Taro Shimizu 2 Abstract: Mondor’s disease (MD) is a rare disease that manifests with a palpable cord-like induration on the body surface. In general, MD is a self-limited, benign thrombophlebitis that resolves in four to eight weeks without any specific treatment. Cases of MD can be roughly categorized into three different groups based on the site of the lesion as follows: original MD of the anterolateral thoracoabdominal wall, penile MD with dorsum and dorsolateral aspects of the penis, and axillary web syndrome with mid-upper arm after axillary surgery. The diagnosis of MD is rather straightforward and based on a physical examinations. However, some case occur “secondary” with another underlying disease, including malignancy, a hypercoagulative state, and vasculitis. Therefore, it is critical to identify MD precisely, evaluate any possible underlying disease, and avoid any un- necessary invasive tests or treatment. In this paper, we comprehensively review the clinical characteristics of MD. Key words: Mondor disease, Mondor’s disease, thrombophlebitis of superficial vein (Intern Med 57: 2607-2612, 2018) (DOI: 10.2169/internalmedicine.0495-17) We herein reviewed the epidemiology, etiology, patho- Introduction physiology, symptomatology, diagnosis, management, and prognosis of MD. Mondor’s disease (MD) occurs with palpable subcutane- ous cord-like indurations beneath the skin. Usually, MD is a Epidemiology and Etiology benign, self-limited disease that resolves spontaneously in four to eight weeks. Cases with cord-like lesions on the Despite many years having lapsed since its first report, chest wall were first reported in the early 1850s, and Henri the details of MD remain unclear due to its rarity.