Leukemia by Dr.Ahmed Gamal
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Leukemoid Reaction in a Patient with Acute Lymphoblastic Leukemia Following the Second Chemotherapy
262JCEI / Yokuş et al. Leukemoid reaction in ALL 2013; 4 (2): 262-263 Journal of Clinical and Experimental Investigations doi: 10.5799/ahinjs.01.2013.02.0280 LETTER TO EDITOR Leukemoid reaction in a patient with acute lymphoblastic leukemia following the second chemotherapy Akut lenfoblastik lösemili hastada ikinci kemoterapi sonrası gelişen lökomoid reaksiyon Osman Yokuş1, Murat Albayrak2, Aynur Albayrak3, Habip Gedik4 To the Editor, to 50.000 cells/µL. The examined peripheral blood smear appeared as similar to the chronic phase of The occurrence of persistent neutrophilic leukocy- CML (fig.2). A cytogenetic examination of Philadel- tosis above 50,000 cells/µL for reasons other than phia chromosome [t(9:22] was found to be nega- leukemia is defined as leukemoid reaction. Chronic tive, therefore, CML was excluded in the patient. myelogenous leukemia (CML) and chronic neutro- Hydroxurea was initiated once a day. Leukocytosis philic leukemia (CNL) should be excluded, and un- recovered to normal range after one week (fig.3) derlying diseases or causes should be examined, and bone marrow examination revealed remission. in differential diagnosis. The most commonly ob- Cytogenetic analysis was normal and this leukocy- served causes of leukemoid reactions are severe tosis was determined as reactive leukemoid reac- infections, intoxications, malignancies, severe hem- tion. We aimed to report this case owing to the fact orrhage, or acute hemolysis [1]. J Clin Exp Invest that leukocytosis associated with G-CSF, which is 2013; 4 (2): 262-263 used to increase the leukocyte count during neutro- Rarely, leukemoid reaction can be seen in pa- penia, has been reported previously but it occurred tients with acute leukemia subsequent to chemo- after second chemotherapy without G-CSF [4]. -

Wikipedia: the Term Leukemoid Reaction Describes an Elevated White Blood
Correspondence: I. Potasman, MD Leukemoid Reaction: Spectrum and Prognosis of 173 Adult Patients Infectious Diseases, ABSTRACT No. Bnai Zion Med. Ctr. 47 Golomb St., Haifa 31048. 39147 Israel Potasman, MD and Moti Grupper, MD Tel. 972-48359055 Fax. 972-48359755 Bnai Zion Med. Ctr., Haifa, Israel Email: [email protected] LR- CLINICAL and LABORATORY FEATURES CHRONIC DISEASES & CONDITIONS CAUSING LR METHODS WikipediA: The term leukemoid reaction describes an elevated white blood cell count, or leukocytosis, that is a physiological response to stress or infection (as Table 1: Leukemoid Reaction: Demographics, Major Clinical, and Laboratory features, and Table 2: Chronic & possible Instigating diseases Causing Leukemoid Reaction (n=173) The BZMC is a 411 bed university hospital located in Haifa, Israel. Mortality (n=173) Disease/Drug Occurrences (%) opposed to a primary blood malignancy, such as leukemia). Contains all basic departments except for neurosurgery, cardiovascular surgery and solid-tumor oncology. The respi- Parameter N (%) Alive Dead n Age (years, mean ±S.D.) 69.4 ±19.6 63.3±21.2 79.4±11.2 Background ratory intensive care unit inhabits six patients; additional respirators are in use in the 3 departments of medicine. History of Cardiovascular 86 (49.7%) Minimal-Maximal 21-97 21-97 28-97 ABSTRACT During an average year there are 29,508 hospitalizations of adults (>18 years) with ~150,000 hospitalization-days, Median 75 69 81 disease Diabetes Mellitus 46 (26.6%) and an average occupancy of 92%. Patients were eligible throughout hospital stay, and wherever they were admit- Chronic Lung disease 29 (16.8%) ted. -

Management of Hepatic Burkitt Lymphoma in Children
Gastroenterology & Hepatology International Journal ISSN: 2574-8009 Management of Hepatic Burkitt Lymphoma in Children Elhoudzi J* and Harif M Case Report Pediatric Hematology & Oncology Department, University Hospital Center, Morocco Volume 3 Issue 1 Medical school of Marrakesh, Cady Ayad University, Morocco Received Date: June 02, 2018 Published Date: June 15, 2018 *Corresponding author: Jamila Elhoudzi, Pediatric Hematology & Oncology Department, University Hospital Center, Morocco, Ibn Sina street, Ammerchich, 40000, Morocco, Tel: 00212661544256; Email: [email protected] . Abstract Hepatic Burkitt lymphoma is extremely rare in childhood and can be overlooked in differential diagnosis of liver masses. Patient: A8-year-old girl presented with a 1 month history of abdominal pain and weight loss and jaundice. Results: Physical examination revealed hepatomegaly and no palpable lymph node. Laboratory finding showed mild anemia (hemoglobin, 10,8 g/dL), elevated transaminase (ALT, 305 IU/L; ASAT,755 IU/L), elevated bilitubin (Bilirubin total, 179mg/L, Bilirubin direct, 143mg/l). Abdominal ultrasound shouwed a multiple hepatic lesions. Liver biopsy examination confirmed Burkitt's lymphoma. No metastasis was detected in the thoracic cavity, bone marrow, and spinal fluid. The patient was treated with the combination regimen of cyclophosphamide, doxorubicin, vincristine, prednisone and high dose methotrexate. Cytosine arabinoside and methotrexate were added for CNS prophylaxis by intrathecal installation. Serial follow-up ultrasound showed a marked decrease in the size of hepatic lesions but residual hilar lymph nodes at 2cm and the control showed stable size of lymph node after 28 months of chemotherapy. Conclusion: The clinical feature of primary hepaticlymphoma varies from no symptom to fulminant hepatic failure. There are no specific imaging criteria for diagnosing primary hepatic Burkitt’s lymphoma. -

BHS Leucocytosis and Leucopenia Dr Caers
Leucocytoses & leucopenia Jo Caers Dept of Clinical Hematology [email protected] Bone marrow Blood Granulopoiesis Proliferation & 5 days maturation Storage 1 day Marginisation& Circulation 1 day Tissues 1-2 days Granulopoiesis Proliferation & 5 days maturation Storage 1 day Marginisation& Circulation 1 day Tissues 1-2 days Granulopoiesis Proliferation & 5 days maturation Storage 1 day Marginisation& Circulation 1 day Tissues 1-2 days Lymphocytes Monocytes NORMAL BLOOD CELL COUNT Hemoglobin 12.0 – 15.0 g/dl (F) 13.0 – 17.0 g/dl (M) Red Blood Cells 3.9 – 5.6 x 10 6/µl (F) 4.5 – 6.5 x 10 6/µl (M) Hematocrit 36 – 48% (F) 40 – 52% (M) Mean Corpuscular Volume 80 – 95µ³ Mean Hb Concentration 27 – 34 pg Conc corp mean Hb 30 – 35 g/dl Reticulocytes 0.5 – 20 % Leucocytes 4.0 – 10.0 x 10 3/µl ¨ Neutophils 1.8 – 7.5 Lymphocytes 1.5 – 3.5 Monocytes 0.2 – 0.8 Eosinophils 0.04 – 0.45 Basophils 0.01 – 0.1 Platelets 100 – 400 x 10 3/dl Hyperleucocytosis > 10.000 WBC/mm³ Normal Cells Abnormal cells or blastic cells Infections ? Neutrophilia (> 7.500/mm³) Acute Leukemias Lymphocytosis (> 4.500/mm³) Chronic Myelomonocytic Leukemias Chronic Lymhocytic leukemia Chronic Myeloid Leukemia Non Hodgkin Lymphoma Chronic Monocytosis (> 800/mm³) … Inflammations? Eosinophilia (> 400/mm³) Basophilia (> 100/mm³) Leukoerythroblastic reaction Cytopenia with immature RBCs (normoblasts) immature WBCs (agranular neutrophils, myelocytes, metamyelocytes ) Causes BM infiltration • Solid tumor or hematological malignancy • Myelofibrosis Strong BM stimulation • Infection, -

Reactive Splenomegaly and Variation of Lymphoid-Plasma Cell Population Associated with a Mouse Pituitary Thyrotropic Tumor*
Reactive Splenomegaly and Variation of Lymphoid-Plasma Cell Population Associated with a Mouse Pituitary Thyrotropic Tumor* EDITH E. SPROULANDRAUL GRINBERG (Rosiceli Park Memorial Institute and New York Slate Department of Health, Buffalo, New York) SUMMARY A transplantable thyrotropic pituitary tumor, subline L24a, which grew after 13 months of dormancy in an intact mouse was associated in its early passage with a variety of lymphoid tumors. On subsequent passage, slow growth over a 6- to 12- month period was regularly accompanied by striking splenomegaly without lymphoid or thymic neoplasia. The enlargement was due to a great increase in cells of the lymphoid series in the red pulp without loss of splenic architecture. In thyroidec- tomized mice plasma cells with many Russell bodies were especially numerous, and these cells were found hi hypertrophied lymphoid follicles within other organs. It is suggested that the splenomegaly and, hi earlier passage the lymphoid tumors, may represent an exaggerated antibody response to a tumor's having unusual or abnormal hormonal activity. The transplanted pituitary tumors, in turn, showed severe hemor- rhagic degeneration with peripheral small lymphocyte stasis in the lymphatics. Initial observations concerning pleomorphic reticulum through the courtesy of Dr. Jacob Furth, was studied cell- and lymphosarcomas or lymphoid hyperplasias through repeated passage for purposes of comparison. regularly accompanying a thyrotropic mouse pituitary This tumor has maintained uniform behavior with rapid neoplasm, subline L24a, have been reported (22). The autonomous growth, active secretion of TSH, and a sex original L24 pituitary tumor was developed by Dr. Jacob dependence which was lacking in the L24 line. A mam- Furth by I131thyroid ablation. -

Leukemias Leukemia - Tumor Disease of the Blood System Is Characterized by Three Main Features: 1
Leukemias Leukemia - tumor disease of the blood system is characterized by three main features: 1. Hyperplasia - proliferation of tumor, or a germ hematopoiesis in places where it should be in a normal state (in the bone marrow); 2. Anaplasia - is when the processes of proliferation (cell proliferation) prevails over the differentiation process; 3. Metaplasia - tumor proliferation, of any germ hematopoiesis in places where it should not be (inside the body, the brain, etc.), with an expanding germ hematopoiesis displaces local tissue elements, replacing them with a. Currently, this process is called metastasis. Unlike leucocytosis, leukemoid reactions and other reactive hematopoietic tissue growths at the base of leukemia is uncontrolled (unlimited) cell proliferation in violation of their ability to differentiation and maturation. Loss of ability to mature leukemia cells can take place much more than normal blood cells, the number of cycles of division, and that creates a huge cell production that characterizes leukemia. The etiology of leukemia to date is not certain. On the tumor nature of leukemia indicated by the presence of the general laws that unite leukemias and tumors: a violation of the cell's ability to differentiate; morphological and metabolic anaplasia cells; common etiological factors contributing to the development of leukemia and tumors, and others. The possible etiologic factors causing the development of leukemia, include ionizing radiation, a number of chemicals, viruses. Some importance in the development of leukemia is attached to genetic factors, hereditary and acquired immune deficiency action blastomogenic metabolite of tryptophan and tyrosine. Theories of the origin of leukemia. Radiation theory. The role of ionizing radiation in causing leukemia was proved experimentally. -
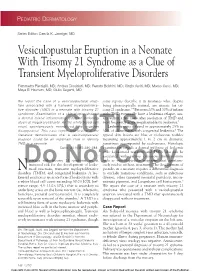
Vesiculopustular Eruption in a Neonate with Trisomy 21 Syndrome As a Clue of Transient Myeloproliferative Disorders
PEDIATRIC DERMATOLOGY Series Editor: Camila K. Janniger, MD Vesiculopustular Eruption in a Neonate With Trisomy 21 Syndrome as a Clue of Transient Myeloproliferative Disorders Fiammetta Piersigilli, MD; Andrea Diociaiuti, MD; Renata Boldrini, MD; Cinzia Auriti, MD; Marco Curci, MD; Maya El Hachem, MD; Giulio Seganti, MD We report the case of a vesiculopustular erup- some reports describe it in neonates who, despite tion associated with a transient myeloprolifera- being phenotypically normal, are mosaic for tri- tive disorder (TMD) in a neonate with trisomy 21 somy 21 syndrome.2-4 Between 20% and 30% of infants syndrome. Examination of a skin biopsy showed with TMD eventually have a leukemia relapse, usu- a dermal mixed inflammatory infiltrate including ally within a few years after resolution of TMD and atypical megakaryoblasts. As the white blood cell most frequently acute megakaryoblastic leukemia.5 count spontaneously normalized, the eruption Leukemia cutis is found in approximately 25% to disappeared. This case report and review of the 30% of all neonates with congenital leukemia.6 The literature demonstrates thatCUTIS a vesiculopustular typical skin lesions are blue or violaceous nodules eruption could be an important clue to identify measuring approximately 1 to 2 cm in diameter, TMD in a neonate. sometimes accompanied by ecchymoses. Histologic Cutis. 2010;85:286-288. examination reveals a dermal infiltrate of leukemic cells. Leukemoid reactions and TMDs also can be associated with various cutaneous manifestations eonates with trisomy 21 syndrome are at such as vesiculopustular eruptions7 that spontane- Doincreased risk for the developmentNot of leuke- ously resolveCopy without treatment. The development of N moid reactions, transient myeloproliferative pustules in a neonate requires a differential diagnosis disorders (TMDs), and congenital leukemia. -

Chronic Myelogenous Leukemia Presenting with Oculomotor Nerve Palsy: a Case Report and Review of Literatures
American Journal of Cancer Case Reports Adhikari BK A et al. American Journal of Cancer Case Reports 2016, 4:51-58 http://ivyunion.org/index.php/ajccr/ Page 1 of 8 6 Case Report Chronic Myelogenous Leukemia Presenting with Oculomotor Nerve Palsy: A Case Report and Review of Literatures Amrit Adhikari BK1*, Dinesh Sangroula2, Saad Rahmat3, and Marie Chevenon3 1 Richmond University Medical Center, Staten Island, NY,USA 2 Northwell Health-The Zucker Hillside Hospital, New York, NY,USA 3 St. George's University School of Medicine, Grenada, West Indies,USA Abstract Introduction: Chronic myelogenous leukemia (CML), the most common sub-type of leukemia, usually presents with anorexia, fatigue, weight loss, splenomegaly, infection, and bleeding diasthesis. Cranial nerve palsy is a rare occurrence with myelo-proliferative disorder. Though prior literatures reported cranial neuropathies with different myelo-proliferative disorders, commonly acute leukemias and lymphomas, this is the first case of CML presenting with oculomotor nerve palsy. Presentation of case: We report a 55-year old African American male presented in emergency department with features of third cranial nerve palsy, including unilateral ptosis, diplopia, and downward-outward deviation of eyeball without involvement of pupil. Clinical suspicion of CML, based on preliminary routine laboratory investigation, was confirmed by bone marrow biopsy and genetic testing of marrow aspirate. Patient was treated with Imatinib and regularly followed up with complete blood count. Conclusion: CML may present with lone cranial nerve palsy as the first clinical finding. Hence, we emphasize to consider leukemia as one of the possible differential diagnoses in suspected patients presenting with isolated oculomotor palsy, if no other cause is evident. -

Leukemoid Reaction in a Preterm Infant: Diagnostic Challenge in Resource Poor Setting: a Case Report
International Journal of Medical and Pharmaceutical Case Reports 13(2): 14-17, 2020; Article no.IJMPCR.61804 ISSN: 2394-109X, NLM ID: 101648033 Leukemoid Reaction in a Preterm Infant: Diagnostic Challenge in Resource Poor Setting: A Case Report Okoli Chukwudi1*, Nwaogu Nwaoma2 and Nwafia Ifeyinwa3 1Department of Haematology/Oncology, Lifeline Children’s Hospital Lekki, Lagos, Nigeria. 2George's Memorial Medical Center Lekki, Lagos, Nigeria. 3College of Medicine, University of Nigeria Ituku, Ozalla Campus, Enugu, Nigeria. Authors’ contributions This work was carried out in collaboration among all authors. Author OC designed the study, performed the statistical analysis, wrote the protocol and wrote the first draft of the manuscript. Authors NN and NI managed the analyses of the study. Author OC managed the literature searches. All authors read and approved the final manuscript. Article Information DOI: 10.9734/IJMPCR/2020/v13i230117 Editor(s): (1) Dr. Jurij Janež, University Medical Centre Ljubljana, Slovenia. Reviewers: (1) Mariana Almada Bassani, University of Campinas, Brasil. (2) Andrezza de Lemos Bezerra, UNINASSAU, Brazil. Complete Peer review History: http://www.sdiarticle4.com/review-history/61804 Received 25 July 2020 Case Study Accepted 30 September 2020 Published 19 October 2020 ABSTRACT A preterm neonate delivered at 28 weeks gestation, mother had antenatal steroid. Blood counts showed leukemoid reaction, blood culture, procalcitonin and peripheral blood film was normal. Baby was stabilized in the NICU, recovered and the WBC count done serially showed a downward trend. The leukemoid reaction was presumed to come from antenatal steroid use. The diagnostic and management challenges encountered in managing the infant in resource constrained environment like ours is presented alongside. -
CML Handbook of Chronic Myeloid Leukemia
Hughes · Ross Melo Timothy P Hughes · David M Ross · Junia V Melo Handbook of Chronic Myeloid Leukemia Myeloid Handbook of Chronic Handbook of Chronic Myeloid Leukemia Timothy P Hughes · David M Ross · Junia V Melo Handbook of Chronic Myeloid Leukemia This independent educational resource is supported by a grant from Novartis Oncology. Timothy P Hughes · David M Ross · Junia V Melo Handbook of Chronic Myeloid Leukemia Timothy P Hughes MD, FRACP, FRCPA, MBBS David M Ross MBBS, PhD, FRACP, FRCPA SA Pathology & SAHMRI University of Adelaide and Flinders University University of Adelaide SA Pathology Department of Hematology Department of Hematology Adelaide Adelaide Australia Australia Junia V Melo MD, PhD, FRCPath University of Adelaide Department of Hematology Adelaide Australia ISBN 978-3-319-08349-0 ISBN 978-3-319-08350-6 (eBook) DOI 10.1007/978-3-319-08350-6 © Springer International Publishing Switzerland 2016 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. The publisher, the authors and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. -

LEUKEMIAS • ALL – “Acute Lymphoblastic Leukemia” A) Occur
LEUKEMIAS • ALL – “Acute Lymphoblastic Leukemia” a) occur at any age i) peak incidence < 5 yrs; incicence again rises in elderly b) ~ 20 % of all leukemias c) most common of leukemias in children d) characterized: i) bone marrow infiltration of immature lymphoid cells (i.e., “BLASTS”) - precussor B and T lymphocytes - spill over into circulation - therefore, blood contains ↑ malignant lymphoid cells e) rapid course i) recurrent infections ii) weakness iii) bleeding into skin and organs iv) enlarged lymph nodes v) mild splenomegaly • AML – “Acute Myelogenous Leukemia” a) ↑ myeloblast in marrow and spill over into blood b) diagnosis of AML i) must have at least 20 % myeloblast in bone marrow c) characteristics: i) most common type of acute leukemia in adults (~ 70 %) ii) “Auer rods” – specific for myeloid d) ALL and AML cannot be differentiated without further biochemical techniques !! • CLL – “Chronic Lymphocytic Leukemia” a) older patients (> 50 yrs) b) CLL cells not distinguishable from mature normal lymphocytes i) “acute CLL” – immature lymphocytes c) CLL is suspected when lymphocytres > 5,000/μL d) progress slowly – not responsiveness to Tx e) B-cell = 95% of all cases (T-cell 5 %) i) B-cell markers = CD19, CD20 ii) T-cell marker = CD5 f) “smudge” cells or “parachute” cells • CML – “ Chronic Myelogenous Leukemia” a) leukocytosis b) disease of adulthood (~ 30 yrs; 85 %) c) three phases: i) chronic - ↑ WBC, Basophils, Eosinophils - < 10 % blasts ii) accelerated - > 10 % blasts, > 20 % Basophils, usually develops into “blasts” crisis - > 20% blasts, develops into acute leukemia profile d) Philadelphia chromosome in ~ 90-95% of CML patients i) BCR/ABL gene rearrangement e) ↓ leukocyte alkaline phosphatase f) Most significant splenomegaly A 38-year-old man complains of increasing weakness and fatigue. -

Download PDF Differential Diagnosis Issues in a Case of Gastric
Romanian Journal of Morphology and Embryology 2009, 50(4):701–705 CASE REPORT Differential diagnosis issues in a case of gastric carcinoma associated with leukemoid reaction C. BOŞOTEANU1), MĂDĂLINA BOŞOTEANU1,2), MARIANA AŞCHIE1,2) 1)Service of Pathology, Emergency County Hospital, Constanta 2)Department of Pathology, Faculty of Medicine, “Ovidius” University, Constanta Abstract Gastric tumors share many characteristics, making a definitive diagnosis challenging. Gastric adenocarcinomas represent 90% of malignant stomach tumors, meanwhile the frequency of gastric lymphoma range between 1–5% of all gastric cancers. Gastric carcinoma bears resemblance with particular forms of non-Hodgkin’s lymphoma of the stomach, not only in morphological presentation, but also in clinical configuration and laboratory tests. We report a case of gastric carcinoma with abnormal hematological picture dominated by leukemoid reaction and peculiar histopathological aspect. Pleomorphism of neoplastic cells and distinct arrangement of these give rise to the need of differentiation between a carcinoma and a non-Hodgkin’s lymphoma of the stomach. On immnohistochemical grounds, we succeeded in our action of segregation between the two lesional entities and we establish as definitive diagnosis that of poorly differentiated gastric adenocarcinoma. Additionally, leukemoid reaction proved to be a manifestation of a bone marrow metastasis from gastric cancer. Keywords: gastric adenocarcinoma, diffuse large B-cell lymphoma, anaplastic large cell lymphoma, immunohistochemistry, leukemoid reaction. Introduction Patient and Methods Gastric tumors share many characteristics, making a We expose the case of a male patient, D.M., definitive diagnosis challenging. Gastric adenocarci- 74-year-old, diagnosed and surgically treated for a nomas represent 90% of malignant stomach tumors and gastric malignant tumor.