BHS Leucocytosis and Leucopenia Dr Caers
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Leukemoid Reaction in a Patient with Acute Lymphoblastic Leukemia Following the Second Chemotherapy
262JCEI / Yokuş et al. Leukemoid reaction in ALL 2013; 4 (2): 262-263 Journal of Clinical and Experimental Investigations doi: 10.5799/ahinjs.01.2013.02.0280 LETTER TO EDITOR Leukemoid reaction in a patient with acute lymphoblastic leukemia following the second chemotherapy Akut lenfoblastik lösemili hastada ikinci kemoterapi sonrası gelişen lökomoid reaksiyon Osman Yokuş1, Murat Albayrak2, Aynur Albayrak3, Habip Gedik4 To the Editor, to 50.000 cells/µL. The examined peripheral blood smear appeared as similar to the chronic phase of The occurrence of persistent neutrophilic leukocy- CML (fig.2). A cytogenetic examination of Philadel- tosis above 50,000 cells/µL for reasons other than phia chromosome [t(9:22] was found to be nega- leukemia is defined as leukemoid reaction. Chronic tive, therefore, CML was excluded in the patient. myelogenous leukemia (CML) and chronic neutro- Hydroxurea was initiated once a day. Leukocytosis philic leukemia (CNL) should be excluded, and un- recovered to normal range after one week (fig.3) derlying diseases or causes should be examined, and bone marrow examination revealed remission. in differential diagnosis. The most commonly ob- Cytogenetic analysis was normal and this leukocy- served causes of leukemoid reactions are severe tosis was determined as reactive leukemoid reac- infections, intoxications, malignancies, severe hem- tion. We aimed to report this case owing to the fact orrhage, or acute hemolysis [1]. J Clin Exp Invest that leukocytosis associated with G-CSF, which is 2013; 4 (2): 262-263 used to increase the leukocyte count during neutro- Rarely, leukemoid reaction can be seen in pa- penia, has been reported previously but it occurred tients with acute leukemia subsequent to chemo- after second chemotherapy without G-CSF [4]. -

Wikipedia: the Term Leukemoid Reaction Describes an Elevated White Blood
Correspondence: I. Potasman, MD Leukemoid Reaction: Spectrum and Prognosis of 173 Adult Patients Infectious Diseases, ABSTRACT No. Bnai Zion Med. Ctr. 47 Golomb St., Haifa 31048. 39147 Israel Potasman, MD and Moti Grupper, MD Tel. 972-48359055 Fax. 972-48359755 Bnai Zion Med. Ctr., Haifa, Israel Email: [email protected] LR- CLINICAL and LABORATORY FEATURES CHRONIC DISEASES & CONDITIONS CAUSING LR METHODS WikipediA: The term leukemoid reaction describes an elevated white blood cell count, or leukocytosis, that is a physiological response to stress or infection (as Table 1: Leukemoid Reaction: Demographics, Major Clinical, and Laboratory features, and Table 2: Chronic & possible Instigating diseases Causing Leukemoid Reaction (n=173) The BZMC is a 411 bed university hospital located in Haifa, Israel. Mortality (n=173) Disease/Drug Occurrences (%) opposed to a primary blood malignancy, such as leukemia). Contains all basic departments except for neurosurgery, cardiovascular surgery and solid-tumor oncology. The respi- Parameter N (%) Alive Dead n Age (years, mean ±S.D.) 69.4 ±19.6 63.3±21.2 79.4±11.2 Background ratory intensive care unit inhabits six patients; additional respirators are in use in the 3 departments of medicine. History of Cardiovascular 86 (49.7%) Minimal-Maximal 21-97 21-97 28-97 ABSTRACT During an average year there are 29,508 hospitalizations of adults (>18 years) with ~150,000 hospitalization-days, Median 75 69 81 disease Diabetes Mellitus 46 (26.6%) and an average occupancy of 92%. Patients were eligible throughout hospital stay, and wherever they were admit- Chronic Lung disease 29 (16.8%) ted. -

Reptile Clinical Pathology Vickie Joseph, DVM, DABVP (Avian)
Reptile Clinical Pathology Vickie Joseph, DVM, DABVP (Avian) Session #121 Affiliation: From the Bird & Pet Clinic of Roseville, 3985 Foothills Blvd. Roseville, CA 95747, USA and IDEXX Laboratories, 2825 KOVR Drive, West Sacramento, CA 95605, USA. Abstract: Hematology and chemistry values of the reptile may be influenced by extrinsic and intrinsic factors. Proper processing of the blood sample is imperative to preserve cell morphology and limit sample artifacts. Identifying the abnormal changes in the hemogram and biochemistries associated with anemia, hemoparasites, septicemias and neoplastic disorders will aid in the prognostic and therapeutic decisions. Introduction Evaluating the reptile hemogram is challenging. Extrinsic factors (season, temperature, habitat, diet, disease, stress, venipuncture site) and intrinsic factors (species, gender, age, physiologic status) will affect the hemogram numbers, distribution of the leukocytes and the reptile’s response to disease. Certain procedures should be ad- hered to when drawing and processing the blood sample to preserve cell morphology and limit sample artifact. The goal of this paper is to briefly review reptile red blood cell and white blood cell identification, normal cell morphology and terminology. A detailed explanation of abnormal changes seen in the hemogram and biochem- istries in response to anemia, hemoparasites, septicemias and neoplasia will be addressed. Hematology and Chemistries Blood collection and preparation Although it is not the scope of this paper to address sites of blood collection and sample preparation, a few im- portant points need to be explained. For best results to preserve cell morphology and decrease sample artifacts, hematologic testing should be performed as soon as possible following blood collection. -

Management of Hepatic Burkitt Lymphoma in Children
Gastroenterology & Hepatology International Journal ISSN: 2574-8009 Management of Hepatic Burkitt Lymphoma in Children Elhoudzi J* and Harif M Case Report Pediatric Hematology & Oncology Department, University Hospital Center, Morocco Volume 3 Issue 1 Medical school of Marrakesh, Cady Ayad University, Morocco Received Date: June 02, 2018 Published Date: June 15, 2018 *Corresponding author: Jamila Elhoudzi, Pediatric Hematology & Oncology Department, University Hospital Center, Morocco, Ibn Sina street, Ammerchich, 40000, Morocco, Tel: 00212661544256; Email: [email protected] . Abstract Hepatic Burkitt lymphoma is extremely rare in childhood and can be overlooked in differential diagnosis of liver masses. Patient: A8-year-old girl presented with a 1 month history of abdominal pain and weight loss and jaundice. Results: Physical examination revealed hepatomegaly and no palpable lymph node. Laboratory finding showed mild anemia (hemoglobin, 10,8 g/dL), elevated transaminase (ALT, 305 IU/L; ASAT,755 IU/L), elevated bilitubin (Bilirubin total, 179mg/L, Bilirubin direct, 143mg/l). Abdominal ultrasound shouwed a multiple hepatic lesions. Liver biopsy examination confirmed Burkitt's lymphoma. No metastasis was detected in the thoracic cavity, bone marrow, and spinal fluid. The patient was treated with the combination regimen of cyclophosphamide, doxorubicin, vincristine, prednisone and high dose methotrexate. Cytosine arabinoside and methotrexate were added for CNS prophylaxis by intrathecal installation. Serial follow-up ultrasound showed a marked decrease in the size of hepatic lesions but residual hilar lymph nodes at 2cm and the control showed stable size of lymph node after 28 months of chemotherapy. Conclusion: The clinical feature of primary hepaticlymphoma varies from no symptom to fulminant hepatic failure. There are no specific imaging criteria for diagnosing primary hepatic Burkitt’s lymphoma. -

Reactive Splenomegaly and Variation of Lymphoid-Plasma Cell Population Associated with a Mouse Pituitary Thyrotropic Tumor*
Reactive Splenomegaly and Variation of Lymphoid-Plasma Cell Population Associated with a Mouse Pituitary Thyrotropic Tumor* EDITH E. SPROULANDRAUL GRINBERG (Rosiceli Park Memorial Institute and New York Slate Department of Health, Buffalo, New York) SUMMARY A transplantable thyrotropic pituitary tumor, subline L24a, which grew after 13 months of dormancy in an intact mouse was associated in its early passage with a variety of lymphoid tumors. On subsequent passage, slow growth over a 6- to 12- month period was regularly accompanied by striking splenomegaly without lymphoid or thymic neoplasia. The enlargement was due to a great increase in cells of the lymphoid series in the red pulp without loss of splenic architecture. In thyroidec- tomized mice plasma cells with many Russell bodies were especially numerous, and these cells were found hi hypertrophied lymphoid follicles within other organs. It is suggested that the splenomegaly and, hi earlier passage the lymphoid tumors, may represent an exaggerated antibody response to a tumor's having unusual or abnormal hormonal activity. The transplanted pituitary tumors, in turn, showed severe hemor- rhagic degeneration with peripheral small lymphocyte stasis in the lymphatics. Initial observations concerning pleomorphic reticulum through the courtesy of Dr. Jacob Furth, was studied cell- and lymphosarcomas or lymphoid hyperplasias through repeated passage for purposes of comparison. regularly accompanying a thyrotropic mouse pituitary This tumor has maintained uniform behavior with rapid neoplasm, subline L24a, have been reported (22). The autonomous growth, active secretion of TSH, and a sex original L24 pituitary tumor was developed by Dr. Jacob dependence which was lacking in the L24 line. A mam- Furth by I131thyroid ablation. -

Persistent Eosinophilia Is a Challenging Problem
DOI: 10.26717/BJSTR.2017.01.000244 Nahla A M Hamed. Biomed J Sci & Tech Res ISSN: 2574-1241 Editorial Open Access Persistent Eosinophilia is a Challenging Problem Nahla AM Hamed* Professor of Hematology, Faculty of Medicine, Alexandria University, Egypt Received: July 25, 2017; Published: August 01, 2017 *Corresponding author: Nahla AM Hamed, Professor of Hematology, Faculty of Medicine, Alexandria University, Egypt Abstract 9 HE is defined as >1.5 x 10 /L eosinophils in the blood on 2 examinations (interval >1 mo) and/or tissue HE defined by: eosinophils percentage in BM section exceeding 20% of all nucleated cells; and/or extensive eosinophilic tissue infiltration by pathologist opinion; and/or presenceAbbreviations: of marked deposition of eosinophil granule proteins (in the absence or presence of major tissue eosinophils infiltration). AEC: absolute eosinophil count; HE: Hypereosinophilia; ABPA: Allergic Bronchopulmonary Aspergillosis; B-ALL: Acute B-cell lymphoblastic leukemia; GVHD: Graft-Versus-Host Disease; BM: Bone Marrow; PB: Peripheral Blood; IL5: Interleukin 5; AML: Acute Myeloid Leukemia; LV: Lymphocytic Variant; Th2:T-cells have a helper type 2; EPPER: Eosinophilic, polymorphic, and pruritic Eruption Associated with Radiotherapy; MPN: Myeloproliferative Neoplasm; HES: Hypereosinophilic Syndrome; PDGFRA: Platelet-Derived Growth Factor Receptor Alpha; PDGFRB: Platelet-Derived Growth Factor Receptor Beta; FGFR1: Fibroblast Growth Factor Receptor 1; CEL-NOS: Chronic Eosinophilic Leukemia-Not Otherwise Specified; MDS: Myelodysplastic Syndrome; IgH: Ig Heavy Chain; EBV: Epstein-Barr virus Introduction cystic structures (e.g. hydatid cyst, neurocysticercosis) are unlikely Eosinophilia3 is defined as an AEC >500/μL [1].3 The severity ), and severe to cause eosinophilia [7]. Disseminated coccidioidomycosis and of eosinophilia has3 been arbitrarily divided into mild9 (AEC: 500- aspergillosis (when presenting as ABPA) are well-known fungal 1,500/mm ), moderate (AEC: 1,500-5,000/mm causes of eosinophilia. -

Leukemias Leukemia - Tumor Disease of the Blood System Is Characterized by Three Main Features: 1
Leukemias Leukemia - tumor disease of the blood system is characterized by three main features: 1. Hyperplasia - proliferation of tumor, or a germ hematopoiesis in places where it should be in a normal state (in the bone marrow); 2. Anaplasia - is when the processes of proliferation (cell proliferation) prevails over the differentiation process; 3. Metaplasia - tumor proliferation, of any germ hematopoiesis in places where it should not be (inside the body, the brain, etc.), with an expanding germ hematopoiesis displaces local tissue elements, replacing them with a. Currently, this process is called metastasis. Unlike leucocytosis, leukemoid reactions and other reactive hematopoietic tissue growths at the base of leukemia is uncontrolled (unlimited) cell proliferation in violation of their ability to differentiation and maturation. Loss of ability to mature leukemia cells can take place much more than normal blood cells, the number of cycles of division, and that creates a huge cell production that characterizes leukemia. The etiology of leukemia to date is not certain. On the tumor nature of leukemia indicated by the presence of the general laws that unite leukemias and tumors: a violation of the cell's ability to differentiate; morphological and metabolic anaplasia cells; common etiological factors contributing to the development of leukemia and tumors, and others. The possible etiologic factors causing the development of leukemia, include ionizing radiation, a number of chemicals, viruses. Some importance in the development of leukemia is attached to genetic factors, hereditary and acquired immune deficiency action blastomogenic metabolite of tryptophan and tyrosine. Theories of the origin of leukemia. Radiation theory. The role of ionizing radiation in causing leukemia was proved experimentally. -
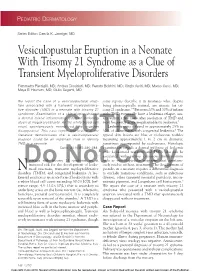
Vesiculopustular Eruption in a Neonate with Trisomy 21 Syndrome As a Clue of Transient Myeloproliferative Disorders
PEDIATRIC DERMATOLOGY Series Editor: Camila K. Janniger, MD Vesiculopustular Eruption in a Neonate With Trisomy 21 Syndrome as a Clue of Transient Myeloproliferative Disorders Fiammetta Piersigilli, MD; Andrea Diociaiuti, MD; Renata Boldrini, MD; Cinzia Auriti, MD; Marco Curci, MD; Maya El Hachem, MD; Giulio Seganti, MD We report the case of a vesiculopustular erup- some reports describe it in neonates who, despite tion associated with a transient myeloprolifera- being phenotypically normal, are mosaic for tri- tive disorder (TMD) in a neonate with trisomy 21 somy 21 syndrome.2-4 Between 20% and 30% of infants syndrome. Examination of a skin biopsy showed with TMD eventually have a leukemia relapse, usu- a dermal mixed inflammatory infiltrate including ally within a few years after resolution of TMD and atypical megakaryoblasts. As the white blood cell most frequently acute megakaryoblastic leukemia.5 count spontaneously normalized, the eruption Leukemia cutis is found in approximately 25% to disappeared. This case report and review of the 30% of all neonates with congenital leukemia.6 The literature demonstrates thatCUTIS a vesiculopustular typical skin lesions are blue or violaceous nodules eruption could be an important clue to identify measuring approximately 1 to 2 cm in diameter, TMD in a neonate. sometimes accompanied by ecchymoses. Histologic Cutis. 2010;85:286-288. examination reveals a dermal infiltrate of leukemic cells. Leukemoid reactions and TMDs also can be associated with various cutaneous manifestations eonates with trisomy 21 syndrome are at such as vesiculopustular eruptions7 that spontane- Doincreased risk for the developmentNot of leuke- ously resolveCopy without treatment. The development of N moid reactions, transient myeloproliferative pustules in a neonate requires a differential diagnosis disorders (TMDs), and congenital leukemia. -

Chronic Myelogenous Leukemia Presenting with Oculomotor Nerve Palsy: a Case Report and Review of Literatures
American Journal of Cancer Case Reports Adhikari BK A et al. American Journal of Cancer Case Reports 2016, 4:51-58 http://ivyunion.org/index.php/ajccr/ Page 1 of 8 6 Case Report Chronic Myelogenous Leukemia Presenting with Oculomotor Nerve Palsy: A Case Report and Review of Literatures Amrit Adhikari BK1*, Dinesh Sangroula2, Saad Rahmat3, and Marie Chevenon3 1 Richmond University Medical Center, Staten Island, NY,USA 2 Northwell Health-The Zucker Hillside Hospital, New York, NY,USA 3 St. George's University School of Medicine, Grenada, West Indies,USA Abstract Introduction: Chronic myelogenous leukemia (CML), the most common sub-type of leukemia, usually presents with anorexia, fatigue, weight loss, splenomegaly, infection, and bleeding diasthesis. Cranial nerve palsy is a rare occurrence with myelo-proliferative disorder. Though prior literatures reported cranial neuropathies with different myelo-proliferative disorders, commonly acute leukemias and lymphomas, this is the first case of CML presenting with oculomotor nerve palsy. Presentation of case: We report a 55-year old African American male presented in emergency department with features of third cranial nerve palsy, including unilateral ptosis, diplopia, and downward-outward deviation of eyeball without involvement of pupil. Clinical suspicion of CML, based on preliminary routine laboratory investigation, was confirmed by bone marrow biopsy and genetic testing of marrow aspirate. Patient was treated with Imatinib and regularly followed up with complete blood count. Conclusion: CML may present with lone cranial nerve palsy as the first clinical finding. Hence, we emphasize to consider leukemia as one of the possible differential diagnoses in suspected patients presenting with isolated oculomotor palsy, if no other cause is evident. -

Leukemoid Reaction in a Preterm Infant: Diagnostic Challenge in Resource Poor Setting: a Case Report
International Journal of Medical and Pharmaceutical Case Reports 13(2): 14-17, 2020; Article no.IJMPCR.61804 ISSN: 2394-109X, NLM ID: 101648033 Leukemoid Reaction in a Preterm Infant: Diagnostic Challenge in Resource Poor Setting: A Case Report Okoli Chukwudi1*, Nwaogu Nwaoma2 and Nwafia Ifeyinwa3 1Department of Haematology/Oncology, Lifeline Children’s Hospital Lekki, Lagos, Nigeria. 2George's Memorial Medical Center Lekki, Lagos, Nigeria. 3College of Medicine, University of Nigeria Ituku, Ozalla Campus, Enugu, Nigeria. Authors’ contributions This work was carried out in collaboration among all authors. Author OC designed the study, performed the statistical analysis, wrote the protocol and wrote the first draft of the manuscript. Authors NN and NI managed the analyses of the study. Author OC managed the literature searches. All authors read and approved the final manuscript. Article Information DOI: 10.9734/IJMPCR/2020/v13i230117 Editor(s): (1) Dr. Jurij Janež, University Medical Centre Ljubljana, Slovenia. Reviewers: (1) Mariana Almada Bassani, University of Campinas, Brasil. (2) Andrezza de Lemos Bezerra, UNINASSAU, Brazil. Complete Peer review History: http://www.sdiarticle4.com/review-history/61804 Received 25 July 2020 Case Study Accepted 30 September 2020 Published 19 October 2020 ABSTRACT A preterm neonate delivered at 28 weeks gestation, mother had antenatal steroid. Blood counts showed leukemoid reaction, blood culture, procalcitonin and peripheral blood film was normal. Baby was stabilized in the NICU, recovered and the WBC count done serially showed a downward trend. The leukemoid reaction was presumed to come from antenatal steroid use. The diagnostic and management challenges encountered in managing the infant in resource constrained environment like ours is presented alongside. -

ICON: Eosinophil Disorders
ICON: Eosinophil Disorders The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Valent, P., A. D. Klion, L. J. Rosenwasser, M. Arock, B. S. Bochner, J. H. Butterfield, J. Gotlib, et al. 2012. “ICON: Eosinophil Disorders.” The World Allergy Organization Journal 5 (12): 174-181. doi:10.1097/WOX.0b013e31827f4192. http://dx.doi.org/10.1097/ WOX.0b013e31827f4192. Published Version doi:10.1097/WOX.0b013e31827f4192 Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:11717517 Terms of Use This article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http:// nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of- use#LAA CONSENSUS DOCUMENT ICON: Eosinophil Disorders Peter Valent, MD,1 Amy D. Klion, MD,2 Lanny J. Rosenwasser, MD,3 Michel Arock, PharmD, PhD,4 Bruce S. Bochner, MD,5 Joseph H. Butterfield, MD,6 Jason Gotlib, MD,7 Torsten Haferlach, MD,8 Andrzej Hellmann, MD,9 Hans-Peter Horny, MD,10 Kristin M. Leiferman, MD,11 Georgia Metzgeroth, MD,12 Kenji Matsumoto, MD, PhD,13 Andreas Reiter, MD,12 Florence Roufosse, MD, PhD,14 Marc E. Rothenberg, MD, PhD,15 Hans-Uwe Simon, MD, PhD,16 Karl Sotlar, MD,9 Peter Vandenberghe, MD, PhD,17 Peter F. Weller, MD,18 and Gerald J. Gleich, MD11,19 Key Words: eosinophil disorders, hypereosinophilic syndrome Several different neoplastic, paraneoplastic, infectious, and aller- (HES), global consensus, classification gic disorders may underlie HE. -

The Idiopathic Hypereosinophilic Syndrome and Eosinophilic Leukemias
Editorials, Comments & Views Editorials, Comments & Views tion event permitted the diagnosis to be made. The idiopathic hypereosinophilic syndrome and For several decades the true nature of many exam- eosinophilic leukemias ples of idiopathic HES remained obscure although the striking male dominance suggested that one or more he idiopathic hypereosinophilic syndrome (idio- entities were there to be discovered. Recent research pathic HES) was first defined by Chusid et al. in has revealed at least two explanations of such cases T1975 as a condition in which there was unex- of chronic eosinophilia: (i) reactive eosinophilia as a plained eosinophilia (eosinophil count greater than response to cytokines secreted by aberrant T cells; (ii) 1.5×109/L) persisting for at least 6 months and lead- chronic eosinophilic leukemia with clonal molecular ing to tissue damage.1 The requirement for the genetic abnormalities but generally without cytoge- eosinophilia to persist and remain unexplained for six netic abnormalities. With the application of appropri- months served to exclude examples of reactive ate diagnostic techniques, the number of patients in eosinophilia in which an explanation emerged during whom the eosinophilia remains idiopathic has been this time. The requirement for tissue damage, such as reduced considerably. cardiac damage, would appear to be less important since there is likely to be a phase of this disease that Eosinophilia as a response to cytokines precedes tissue damage. Such patients can be regard- secreted by aberrant T cells ed as having chronic idiopathic eosinophilia (CIE), with Lymphoma, either Hodgkin’s disease or non- the recognition that they may well have the same Hodgkin’s lymphoma, is one of the well recognized spectrum of underlying disorders as those with idio- causes of reactive cytokine-driven eosinophilia.