Ddt in Indoor Residual Spraying: Human Health Aspects
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
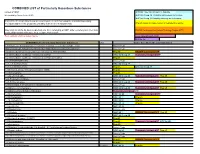
COMBINED LIST of Particularly Hazardous Substances
COMBINED LIST of Particularly Hazardous Substances revised 2/4/2021 IARC list 1 are Carcinogenic to humans list compiled by Hector Acuna, UCSB IARC list Group 2A Probably carcinogenic to humans IARC list Group 2B Possibly carcinogenic to humans If any of the chemicals listed below are used in your research then complete a Standard Operating Procedure (SOP) for the product as described in the Chemical Hygiene Plan. Prop 65 known to cause cancer or reproductive toxicity Material(s) not on the list does not preclude one from completing an SOP. Other extremely toxic chemicals KNOWN Carcinogens from National Toxicology Program (NTP) or other high hazards will require the development of an SOP. Red= added in 2020 or status change Reasonably Anticipated NTP EPA Haz list COMBINED LIST of Particularly Hazardous Substances CAS Source from where the material is listed. 6,9-Methano-2,4,3-benzodioxathiepin, 6,7,8,9,10,10- hexachloro-1,5,5a,6,9,9a-hexahydro-, 3-oxide Acutely Toxic Methanimidamide, N,N-dimethyl-N'-[2-methyl-4-[[(methylamino)carbonyl]oxy]phenyl]- Acutely Toxic 1-(2-Chloroethyl)-3-(4-methylcyclohexyl)-1-nitrosourea (Methyl-CCNU) Prop 65 KNOWN Carcinogens NTP 1-(2-Chloroethyl)-3-cyclohexyl-1-nitrosourea (CCNU) IARC list Group 2A Reasonably Anticipated NTP 1-(2-Chloroethyl)-3-cyclohexyl-1-nitrosourea (CCNU) (Lomustine) Prop 65 1-(o-Chlorophenyl)thiourea Acutely Toxic 1,1,1,2-Tetrachloroethane IARC list Group 2B 1,1,2,2-Tetrachloroethane Prop 65 IARC list Group 2B 1,1-Dichloro-2,2-bis(p -chloropheny)ethylene (DDE) Prop 65 1,1-Dichloroethane -

Replacement Therapy, Not Recreational Tonic Testosterone, Widely Used As a Lifestyle Drug, Is a Medicine and Should Be Kept As Such
correspondence Replacement therapy, not recreational tonic Testosterone, widely used as a lifestyle drug, is a medicine and should be kept as such. Sir — We read with great interest the News male tonics and remedies — most harmless, your Feature that there is a need for large- Feature “A dangerous elixir?” (Nature 431, but some as drastic as grafting goat testicles scale, long-term clinical trials to address 500–501; 2004) reporting the zeal with onto humans. Unfortunately, a certain several issues associated with testosterone which testosterone is being requested by amount of quackery is now perceived to be use. For example, testosterone therapy may men who apparently view the hormone as associated with testosterone therapy, and the be beneficial against osteoporosis, heart a ‘natural’ alternative to the drug Viagra. increased prescription of the hormone in disease and Alzheimer’s disease, but the Like Viagra, testosterone replacement recent years does little to dispel this notion. dangers remain obscure. therapy — with emphasis on the word Nonetheless, as your Feature highlights, Until we know more, both prescribing ‘replacement’ — is a solution to a very real hypogonadism is a very real clinical clinicians and the male population need to clinical problem. There is a distinction condition. It is characterized by abnormally be aware that testosterone, like any other between patients whose testosterone has low serum levels of testosterone, in medication, should only be administered declined to abnormally low levels, and conjunction with symptoms such as to patients for whom such therapy is individuals seeking testosterone as a pick- mood disturbance, depression, sexual clinically indicated. me-up. -

DDT and Its Derivatives Have Remained in the Environment
International Journal of Molecular Sciences Review A Novel Action of Endocrine-Disrupting Chemicals on Wildlife; DDT and Its Derivatives Have Remained in the Environment Ayami Matsushima Laboratory of Structure-Function Biochemistry, Department of Chemistry, Faculty of Science, Kyushu University, Fukuoka 819-0395, Japan; [email protected]; Tel.: +81-92-802-4159 Received: 20 March 2018; Accepted: 2 May 2018; Published: 5 May 2018 Abstract: Huge numbers of chemicals are released uncontrolled into the environment and some of these chemicals induce unwanted biological effects, both on wildlife and humans. One class of these chemicals are endocrine-disrupting chemicals (EDCs), which are released even though EDCs can affect not only the functions of steroid hormones but also of various signaling molecules, including any ligand-mediated signal transduction pathways. Dichlorodiphenyltrichloroethane (DDT), a pesticide that is already banned, is one of the best-publicized EDCs and its metabolites have been considered to cause adverse effects on wildlife, even though the exact molecular mechanisms of the abnormalities it causes still remain obscure. Recently, an industrial raw material, bisphenol A (BPA), has attracted worldwide attention as an EDC because it induces developmental abnormalities even at low-dose exposures. DDT and BPA derivatives have structural similarities in their chemical features. In this short review, unclear points on the molecular mechanisms of adverse effects of DDT found on alligators are summarized from data in the literature, and recent experimental and molecular research on BPA derivatives is investigated to introduce novel perspectives on BPA derivatives. Especially, a recently developed BPA derivative, bisphenol C (BPC), is structurally similar to a DDT derivative called dichlorodiphenyldichloroethylene (DDE). -

Pesticides Reduce Symbiotic Efficiency of Nitrogen-Fixing Rhizobia and Host Plants
Pesticides reduce symbiotic efficiency of nitrogen-fixing rhizobia and host plants Jennifer E. Fox*†, Jay Gulledge‡, Erika Engelhaupt§, Matthew E. Burow†¶, and John A. McLachlan†ʈ *Center for Ecology and Evolutionary Biology, University of Oregon, 335 Pacific Hall, Eugene, OR 97403; †Center for Bioenvironmental Research, Environmental Endocrinology Laboratory, Tulane University, 1430 Tulane Avenue, New Orleans, LA 70112-2699; ‡Department of Biology, University of Louisville, Louisville, KY 40292 ; §University of Colorado, Boulder, CO 80309; and ¶Department of Medicine and Surgery, Hematology and Medical Oncology Section, Tulane University Medical School, 1430 Tulane Avenue, New Orleans, LA 70112-2699 Edited by Christopher B. Field, Carnegie Institution of Washington, Stanford, CA, and approved May 8, 2007 (received for review January 8, 2007) Unprecedented agricultural intensification and increased crop by plants, in rotation with non-N-fixing crops (8, 15). The yield will be necessary to feed the burgeoning world population, effectiveness of this strategy relies on maximizing symbiotic N whose global food demand is projected to double in the next 50 fixation (SNF) and plant yield to resupply organic and inorganic years. Although grain production has doubled in the past four N and nutrients to the soil. The vast majority of biologically fixed decades, largely because of the widespread use of synthetic N is attributable to symbioses between leguminous plants (soy- nitrogenous fertilizers, pesticides, and irrigation promoted by the bean, alfalfa, etc.) and species of Rhizobium bacteria; replacing ‘‘Green Revolution,’’ this rate of increased agricultural output is this natural fertilizer source with synthetic N fertilizer would cost unsustainable because of declining crop yields and environmental Ϸ$10 billion annually (16, 17). -

Past Use of Chlordane, Dieldrin, And
The Hazard Evaluation and Emergency Response Office (HEER Office) is part of the Hawai‘i Department of Health (HDOH) Environmental Health Administration, whose mission is to protect human health and the environment. The HEER Office provides leadership, support, and partnership in preventing, planning for, responding to, and enforcing environmental laws relating to releases or threats of releases of hazardous substances. Past Use of Chlordane, Dieldrin, and other Organochlorine Pesticides for Termite Control in Hawai‘i: Safe Management Practices around Treated Foundations or during Building Demolition This fact sheet provides building owners, demolition and construction contractors, developers, realtors, and others with an overview of the potential environmental concerns associated with the past use of organochlorine termiticides (pesticides used to control termites) in Hawai‘i. In addition, this fact sheet discusses methods for reducing exposure to organochlorine termiticides during building demolition or around the foundations of treated buildings and identifies resources for further information. What are organochlorine termiticides? Organochlorine termiticides are a group of pesticides that were used for termite control in and around wooden buildings and homes from the mid-1940s to the late 1980s. These organochlorine pesticides included chlordane, aldrin, dieldrin, heptachlor, and dichlorodiphenyltrichloroethane (DDT). They were used primarily by pest control operators in Hawaii’s urban areas, but also by homeowners, the military, the state, and counties to protect buildings against termite damage. In the 1970s and 1980s, the U.S. Environmental Protection Agency (EPA) banned all uses of these organochlorine pesticides except for heptachlor, which can be used today only for control of fire ants in underground power transformers. -

Detection of Estrogen Receptor Endocrine Disruptor Potency of Commonly Used Organochlorine Pesticides Using the LUMI-CELL ER Bioassay
DEVELOPMENTAL AND REPRODUCTIVE TOXICITY Detection of Estrogen Receptor Endocrine Disruptor Potency of Commonly Used Organochlorine Pesticides Using The LUMI-CELL ER Bioassay John D. Gordon1, Andrew C: Chu1, Michael D. Chu2, Michael S. Denison3, George C. Clark1 1Xenobiotic Detection Systems, Inc., 1601 E. Geer St., Suite S, Durham, NC 27704, USA 2Alta Analytical Perspectives, 2714 Exchange Drive, Wilmington, NC 28405, USA 3Dept. of Environmental Toxicology, Meyer Hall, Univ. of California, Davis; Davis, CA 95616 USA Introduction Organochlorine pesticides are found in many ecosystems worldwide as result of agricultural and industrial activities and exist as complex mixtures. The use of these organochlorine pesticides has resulted in the contamination of lakes and streams, and eventually the animal and human food chain. Many of these pesticides, such as pp ’-DDT, pp ’-DDE, Kepone, Vinclozolin, and Methoxychlor (a substitute for the banned DDT), have been described as putative estrogenic endocrine disruptors, and act by mimicking endogenous estrogen 1-3 . Estrogenic compounds can have a significant detrimental effect on the endocrine and reproductive systems of both human and other animal populations 4 . Previous studies have shown a strong association between several EDCs (17p-Estradiol, DES, Zeralanol, Zeralenone, Coumestrol, Genistein, Biochanin A, Diadzein, Naringenin, Tamoxifin) and estrogenic activity via uterotropic assay, cell height, gland number, increased lactoferrin, and a transcriptional activity assay using BG1Luc4E2 cells4 . Some other examples of the effects of these EDCs are: decreased reproductive success and feminization of males in several wildlife species; increased hypospadias along with reductions in sperm counts in men; increase in the incidence of human breast and prostate cancers; and endometriosis 3-5 . -

A General-Purpose Garden Pesticide C
West Virginia Agricultural and Forestry Experiment Davis College of Agriculture, Natural Resources Station Bulletins And Design 1-1-1954 A general-purpose garden pesticide C. K. Dorsey M. E. Gallegly Follow this and additional works at: https://researchrepository.wvu.edu/ wv_agricultural_and_forestry_experiment_station_bulletins Digital Commons Citation Dorsey, C. K. and Gallegly, M. E., "A general-purpose garden pesticide" (1954). West Virginia Agricultural and Forestry Experiment Station Bulletins. 365T. https://researchrepository.wvu.edu/wv_agricultural_and_forestry_experiment_station_bulletins/630 This Bulletin is brought to you for free and open access by the Davis College of Agriculture, Natural Resources And Design at The Research Repository @ WVU. It has been accepted for inclusion in West Virginia Agricultural and Forestry Experiment Station Bulletins by an authorized administrator of The Research Repository @ WVU. For more information, please contact [email protected]. BULLETIN 365T June 1954 WEST VIRGINIA UNIVERSITY AGRICULTURAL EXPERIMENT STATION AUTHORS Authors of A General-Purpose Garden Pesti- cide are C. K. DORSEY, Entomologist and Professor of Entomology, and M. E. GAL- LEGLY, Assistant Plant Pathologist and As- sistant Professor of Plant Pathology. ACKNOWLEDGEMENT The authors are indebted to Kemper L. Callahan for assistance in portions of the studies. West Virginia University Agricultural Experiment Station College of Agriculture, Forestry, and Home Economics H. R. Varney, Director MORGANTOWN A General-Purpose Garden Pesticide C. K. DORSEY and M. E. GALLEGLY IN recent years numerous new insecticides and fungicides have been developed and many have been recommended for use in the home garden. These vary considerably in their effectiveness in the control of different pests. For example, rotenone is effective in controlling the Mexican bean beetle and the potato flea beetle, but is ineffective against the potato leafhopper. -

WO 2012/148799 Al 1 November 2012 (01.11.2012) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2012/148799 Al 1 November 2012 (01.11.2012) P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 9/107 (2006.01) A61K 9/00 (2006.01) kind of national protection available): AE, AG, AL, AM, A 61 47/10 (2006.0V) AO, AT, AU, AZ, BA, BB, BG, BH, BR, BW, BY, BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, DO, (21) International Application Number: DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, HN, PCT/US2012/034361 HR, HU, ID, IL, IN, IS, JP, KE, KG, KM, KN, KP, KR, (22) International Filing Date: KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, 20 April 2012 (20.04.2012) MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, OM, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SC, SD, (25) Filing Language: English SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, (26) Publication Language: English TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. (30) Priority Data: (84) Designated States (unless otherwise indicated, for every 61/480,259 28 April 201 1 (28.04.201 1) US kind of regional protection available): ARIPO (BW, GH, GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, SZ, TZ, (71) Applicant (for all designated States except US): BOARD UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, MD, RU, OF REGENTS, THE UNIVERSITY OF TEXAS SYS¬ TJ, TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, TEM [US/US]; 201 West 7th St., Austin, TX 78701 (US). -

Prenatal Testosterone Supplementation Alters Puberty Onset, Aggressive Behavior, and Partner Preference in Adult Male Rats
J Physiol Sci (2012) 62:123–131 DOI 10.1007/s12576-011-0190-7 ORIGINAL PAPER Prenatal testosterone supplementation alters puberty onset, aggressive behavior, and partner preference in adult male rats Cynthia Dela Cruz • Oduvaldo C. M. Pereira Received: 26 October 2011 / Accepted: 19 December 2011 / Published online: 11 January 2012 Ó The Physiological Society of Japan and Springer 2012 Abstract The objective of this study was to investigate because pregnant women exposed to hyperandrogenemia whether prenatal exposure to testosterone (T) could change and then potentially exposing their unborn children to ele- the body weight (BW), anogenital distance (AGD), ano- vated androgen levels in the uterus can undergo alteration of genital distance index (AGDI), puberty onset, social normal levels of T during the sexual differentiation period, behavior, fertility, sexual behavior, sexual preference, and T and, as a consequence, affect the reproductive and behavior level of male rats in adulthood. To test this hypothesis, patterns of their children in adulthood. pregnant rats received either 1 mg/animal of T propionate diluted in 0.1 ml peanut oil or 0.1 ml peanut oil, as control, Keywords Aggressive behavior Á Male rats Á on the 17th, 18th and 19th gestational days. No alterations in Prenatal testosterone Á Puberty onset Á Sexual behavior Á BW, AGD, AGDI, fertility, and sexual behavior were Sexual differentiation observed (p [ 0.05). Delayed onset of puberty (p \ 0.0001), increased aggressive behavior (p [ 0.05), altered pattern of sexual preference (p \ 0.05), and reduced T plasma level Introduction (p \ 0.05) were observed for adult male rats exposed pre- natally to T. -

California Proposition 65 (Prop65)
20 NOVEMBER 2018 To Whom It May Concern: Certificate of Compliance California Proposition 65 California’s Proposition 65 entitles California consumers to special warnings for products that contain chemicals known to the state of California to cause cancer and birth defects or other reproductive harm if those products expose consumers to such chemicals above certain threshold levels. This is to certify that Alliance Memory comply with Safe Drinking Water and Toxic Enforcement Act of 1986, commonly known as California Proposition 65, that are ‘known to the state to cause cancer or reproductive toxicity’ as of December 29, 2017, by following the labelling guidelines set out therein. Alliance Memory labelling system clearly states a ‘Prop65 warning’ as and when necessary, on product packaging that is destined for the state of California, USA. This document certifies that to the best of our current knowledge and belief and under normal usage, Alliance Memory’s IC products are in compliance with California Proposition 65 – The Safe Drinking Water and Toxic Enforcement Act, 1986) and do not contain chemical elements of those listed within the California Proposition 65 chemical listing as shown below. Signature : Date: 20 November 2018 Name : Kim Bagby Title : Director QRA Department/Alliance Memory California Proposition 65 list of chemicals. The following is a list of chemicals published as a requirement of Safe Drinking Water and Toxic Enforcement Act of 1986, commonly known as California Proposition 65, that are ‘known to the state to cause -

Exposure to Endocrine Disrupting Chemicals and Risk of Breast Cancer
International Journal of Molecular Sciences Review Exposure to Endocrine Disrupting Chemicals and Risk of Breast Cancer Louisane Eve 1,2,3,4,Béatrice Fervers 5,6, Muriel Le Romancer 2,3,4,* and Nelly Etienne-Selloum 1,7,8,* 1 Faculté de Pharmacie, Université de Strasbourg, F-67000 Strasbourg, France; [email protected] 2 Université Claude Bernard Lyon 1, F-69000 Lyon, France 3 Inserm U1052, Centre de Recherche en Cancérologie de Lyon, F-69000 Lyon, France 4 CNRS UMR5286, Centre de Recherche en Cancérologie de Lyon, F-69000 Lyon, France 5 Centre de Lutte Contre le Cancer Léon-Bérard, F-69000 Lyon, France; [email protected] 6 Inserm UA08, Radiations, Défense, Santé, Environnement, Center Léon Bérard, F-69000 Lyon, France 7 Service de Pharmacie, Institut de Cancérologie Strasbourg Europe, F-67000 Strasbourg, France 8 CNRS UMR7021/Unistra, Laboratoire de Bioimagerie et Pathologies, Faculté de Pharmacie, Université de Strasbourg, F-67000 Strasbourg, France * Correspondence: [email protected] (M.L.R.); [email protected] (N.E.-S.); Tel.: +33-4-(78)-78-28-22 (M.L.R.); +33-3-(68)-85-43-28 (N.E.-S.) Received: 27 October 2020; Accepted: 25 November 2020; Published: 30 November 2020 Abstract: Breast cancer (BC) is the second most common cancer and the fifth deadliest in the world. Exposure to endocrine disrupting pollutants has been suggested to contribute to the increase in disease incidence. Indeed, a growing number of researchershave investigated the effects of widely used environmental chemicals with endocrine disrupting properties on BC development in experimental (in vitro and animal models) and epidemiological studies. -

Health Effects Support Document for 1,1-Dichloro-2,2- Bis(P-Chlorophenyl)Ethylene (DDE)
Health Effects Support Document for 1,1-Dichloro-2,2- bis(p-chlorophenyl)ethylene (DDE) Health Effects Support Document for 1,1-Dichloro-2,2-bis(p-chlorophenyl)ethylene (DDE) U.S. Environmental Protection Agency Office of Water (4304T) Health and Ecological Criteria Division Washington, DC 20460 www.epa.gov/safewater/ccl/pdf/DDE.pdf EPA Document Number EPA-822-R-08-003 January, 2008 Printed on Recycled Paper DDE — January, 2008 iv FOREWORD The Safe Drinking Water Act (SDWA), as amended in 1996, requires the Administrator of the Environmental Protection Agency (EPA) to establish a list of contaminants to aid the Agency in regulatory priority setting for the drinking water program. In addition, the SDWA requires EPA to make regulatory determinations for no fewer than five contaminants by August 2001 and every five years thereafter. The criteria used to determine whether or not to regulate a chemical on the Contaminant Candidate List (CCL) are the following: • The contaminant may have an adverse effect on the health of persons. • The contaminant is known to occur or there is a substantial likelihood that the contaminant will occur in public water systems with a frequency and at levels of public health concern. • In the sole judgment of the Administrator, regulation of such contaminant presents a meaningful opportunity for health risk reduction for persons served by public water systems. The Agency’s findings for all three criteria are used in making a determination to regulate a contaminant. The Agency may determine that there is no need for regulation when a contaminant fails to meet one of the criteria.