The Relationship Between Sleep Duration and Working Memory in Children
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Compare and Contrast Two Models Or Theories of One Cognitive Process with Reference to Research Studies
! The following sample is for the learning objective: Compare and contrast two models or theories of one cognitive process with reference to research studies. What is the question asking for? * A clear outline of two models of one cognitive process. The cognitive process may be memory, perception, decision-making, language or thinking. * Research is used to support the models as described. The research does not need to be outlined in a lot of detail, but underatanding of the role of research in supporting the models should be apparent.. * Both similarities and differences of the two models should be clearly outlined. Sample response The theory of memory is studied scientifically and several models have been developed to help The cognitive process describe and potentially explain how memory works. Two models that attempt to describe how (memory) and two models are memory works are the Multi-Store Model of Memory, developed by Atkinson & Shiffrin (1968), clearly identified. and the Working Memory Model of Memory, developed by Baddeley & Hitch (1974). The Multi-store model model explains that all memory is taken in through our senses; this is called sensory input. This information is enters our sensory memory, where if it is attended to, it will pass to short-term memory. If not attention is paid to it, it is displaced. Short-term memory Research. is limited in duration and capacity. According to Miller, STM can hold only 7 plus or minus 2 pieces of information. Short-term memory memory lasts for six to twelve seconds. When information in the short-term memory is rehearsed, it enters the long-term memory store in a process called “encoding.” When we recall information, it is retrieved from LTM and moved A satisfactory description of back into STM. -

Dissociation Between Declarative and Procedural Mechanisms in Long-Term Memory
! DISSOCIATION BETWEEN DECLARATIVE AND PROCEDURAL MECHANISMS IN LONG-TERM MEMORY A dissertation submitted to the Kent State University College of Education, Health, and Human Services in partial fulfillment of the requirements for the degree of Doctor of Philosophy By Dale A. Hirsch August, 2017 ! A dissertation written by Dale A. Hirsch B.A., Cleveland State University, 2010 M.A., Cleveland State University, 2013 Ph.D., Kent State University, 2017 Approved by _________________________, Director, Doctoral Dissertation Committee Bradley Morris _________________________, Member, Doctoral Dissertation Committee Christopher Was _________________________, Member, Doctoral Dissertation Committee Karrie Godwin Accepted by _________________________, Director, School of Lifespan Development and Mary Dellmann-Jenkins Educational Sciences _________________________, Dean, College of Education, Health and Human James C. Hannon Services ! ""! ! HIRSCH, DALE A., Ph.D., August 2017 Educational Psychology DISSOCIATION BETWEEN DECLARATIVE AND PROCEDURAL MECHANISMS IN LONG-TERM MEMORY (66 pp.) Director of Dissertation: Bradley Morris The purpose of this study was to investigate the potential dissociation between declarative and procedural elements in long-term memory for a facilitation of procedural memory (FPM) paradigm. FPM coupled with a directed forgetting (DF) manipulation was utilized to highlight the dissociation. Three experiments were conducted to that end. All three experiments resulted in facilitation for categorization operations. Experiments one and two additionally found relatively poor recognition for items that participants were told to forget despite the fact that relevant categorization operations were facilitated. Experiment three resulted in similarly poor recognition for category names that participants were told to forget. Taken together, the three experiments in this investigation demonstrate a clear dissociation between the procedural and declarative elements of the FPM task. -

Working Memory and Cued Recall Max V
Georgia Southern University Digital Commons@Georgia Southern University Honors Program Theses 2016 Working memory and cued recall Max V. Fey 8602950 Karen Naufel Georgia Southern University Lawrence Locker Georgia Southern University Follow this and additional works at: https://digitalcommons.georgiasouthern.edu/honors-theses Part of the Cognitive Psychology Commons Recommended Citation Fey, Max V. 8602950; Naufel, Karen; and Locker, Lawrence, "Working memory and cued recall" (2016). University Honors Program Theses. 220. https://digitalcommons.georgiasouthern.edu/honors-theses/220 This thesis (open access) is brought to you for free and open access by Digital Commons@Georgia Southern. It has been accepted for inclusion in University Honors Program Theses by an authorized administrator of Digital Commons@Georgia Southern. For more information, please contact [email protected]. 1 Working Memory and Cued Recall Working Memory and Cued Recall An Honors Thesis submitted in partial fulfillment of the requirements for Honors in the Department of Psychology. By Maximilian Fey Under the mentorship of Dr. Karen Naufel ABSTRACT Previous research has found that individuals with high working memory have greater recall capabilities than those with low working memory (Unsworth, Spiller, & Brewers, 2012). Research did not test the extent to which cues affect one’s recall ability in relation to working memory. The present study will examine this issue. Participants completed a working memory measure. Then, they were provided with cued recall tasks whereby they recalled Facebook friends. The cues varied to be no cues, ambiguous cues high in imageability, and cues directly related to Facebook. The results showed that there was no difference between individual’s ability to recall their Facebook friends and their working memory scores. -
Working Memory and the Organization of Brain Systems
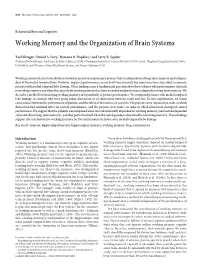
4818 • The Journal of Neuroscience, April 30, 2008 • 28(18):4818–4822 Behavioral/Systems/Cognitive Working Memory and the Organization of Brain Systems Yael Shrager,1 Daniel A. Levy,2 Ramona O. Hopkins,3 and Larry R. Squire4 1University of California, San Diego, La Jolla, California 92093, 2Weizmann Institute of Science, Rechovot 76100, Israel, 3Brigham Young University, Provo, Utah 84602, and 4Veterans Affairs Healthcare System, San Diego, California 92161 Working memory has historically been viewed as an active maintenance process that is independent of long-term memory and indepen- dent of the medial temporal lobe. However, impaired performance across brief time intervals has sometimes been described in amnesic patients with medial temporal lobe damage. These findings raise a fundamental question about how to know when performance depends on working memory and when the capacity for working memory has been exceeded and performance depends on long-term memory. We describe a method for identifying working memory independently of patient performance. We compared patients with medial temporal lobe damage to controls who were given either distraction or no distraction between study and test. In four experiments, we found concordance between the performance of patients and the effect of distraction on controls. The patients were impaired on tasks in which distraction had minimal effect on control performance, and the patients were intact on tasks in which distraction disrupted control performance. We suggest that the patients were impaired when the task minimally depended on working memory (and instead depended substantially on long-term memory), and they performed well when the task depended substantially on working memory. -

What Is Working Memory and How Does It Affect Learning?
3/16/2016 What is working Do you observe these behaviours? memory and how does Is easily distracted when doing something not highly it affect learning? interesting Has trouble waiting his/her turn Struggles with getting started and completing a task. Watches and depends on friends to remind them of the current task Difficulty organising something with multiple steps… frequently stops, frequently loses their place Often seems restless and on the go Fails to progress despite working hard Quick mental arithmetic What is working memory? Who does it affect? 7 + 9 x 3 –4 = 35 x 9 = 35 x 76 = 1 3/16/2016 How does it differ from short term What is working memory? memory? Repeating multi-part instructions A system for temporary Carrying out instructions storage and manipulation of information, necessary for wide range of cognitive tasks Remembering a street address Following driving directions The ability to keep information Following driving directions as a new driver active in your mind for a short period of time (seconds) keeping it available for further processing Working memory is an essential function Alan Baddeley’s Working Memory Metaphor in every day life Central Executive Processes all stimuli we encounter Delegates it to the different parts of our brain that can take action Allows us to block out unnecessary information Visuo-Spatial Phonological Loop Episodic Buffer It keeps us updated on what’s Sketch Pad happening – and keeps us focused on what matters 2 3/16/2016 Working Memory (WM) Capacity: Storage AND Attention Dependent on Many Variables • WM capacity – affected by deficit: disease, genetics, age….but also fatigue, medication, mood. -
Working Memory
Working Memory Chapter 4 1 Working Memory Some memories are very fragile and go into oblivion very quickly. Working memory is one such memory. 1. Try this. Do this mentally. Write your answers on paper. a. 7 X 9 = 63 b. 74 X 9 = 666 c. 74 X 96 = 7104 2 Working Memory (WM) 1. We know attention is limited. So information that gets to memory is also limited. Thus capacity of working memory is limited. 2. Working memory is brief, immediate memory we use for current information. A portion of working memory coordinates ongoing mental activities. 3. Working memory has been known as short-term memory, and is contrasted from long-term. Some investigators believe the two are the same (Nairne, 2002). 3 1 Classic Research on Working Memory (Short-term Memory) 4 Short-term Memory In the 19th century, Sir George Hamilton discovered that he could accurately store about 7 items (marbles) in memory if he glanced at the items quickly. If the items were more than 7 his accuracy decreased. Sir George Hamilton 5 Short-term Memory 1. Miller (1956) wrote, “The magical number seven plus or minus two: some limits on our capacity for processing information”. 2. Miller suggested that the capacity of our short-term memory was small. We could store about 5-9 items in it. 3. He also showed that items could be “chunked”, which would increase our memory capacity. George Miller 6 2 Try This ! C T A I I L T C S F R O R E C A L L ! F R A C T O L I S T I C R E C A L L ! 7 Another Example 870-230-5339 (10 items) 870 + 230 + 5 3 3 9 (1) (1) (4) 2 chunks + 4 items (6 items) Capacity of short-term memory may be increased by a process called “chunking”. -

Sleep Problems Across Development: a Pathway to Adolescent Risk Taking Through Working Memory
J Youth Adolescence DOI 10.1007/s10964-014-0179-7 EMPIRICAL RESEARCH Sleep Problems Across Development: A Pathway to Adolescent Risk Taking Through Working Memory April Gile Thomas • Kathryn C. Monahan • Angela F. Lukowski • Elizabeth Cauffman Received: 22 April 2014 / Accepted: 23 August 2014 Ó Springer Science+Business Media New York 2014 Abstract Problematic sleep can be detrimental to the middle childhood to adolescence. Although sleep problems development of important cognitive functions, such as in infancy, early childhood, and middle childhood were not working memory, and may have the potential for negative directly related to adolescent working memory, sleep behavioral consequences, such as risk-taking. In this way, problems during adolescence were associated with poorer sleep problems may be particularly harmful for youth— adolescent working memory. In turn, these deficits in whose cognitive abilities are still developing and who are working memory were related to greater risk taking in late more susceptible to risky behavior. Using data from a large, adolescence. In summary, the present results suggest that national, longitudinal study, continuity and change in sleep sleep problems in earlier periods are indicative of risk for problems were examined from 2 to 15 years of age and sleep problems later in development, but that sleep problems associated with deficits in working memory at age 15 and in adolescence contribute uniquely to deficits in working risk taking behaviors at age 18. Participants (N = 1,364 memory that, in turn, lead to risky behavior during late children; 48.3 % female) were assessed for sleep problems adolescence. (parent-report), working memory (behavioral task), and risk taking behavior (youth self-report). -

The Declarative/Procedural Model Michael T
Cognition 92 (2004) 231–270 www.elsevier.com/locate/COGNIT Contributions of memory circuits to language: the declarative/procedural model Michael T. Ullman* Brain and Language Laboratory, Departments of Neuroscience, Linguistics, Psychology and Neurology, Georgetown University, Washington, DC, USA Received 12 December 2001; revised 13 December 2002; accepted 29 October 2003 Abstract The structure of the brain and the nature of evolution suggest that, despite its uniqueness, language likely depends on brain systems that also subserve other functions. The declarative/procedural (DP) model claims that the mental lexicon of memorized word-specific knowledge depends on the largely temporal-lobe substrates of declarative memory, which underlies the storage and use of knowledge of facts and events. The mental grammar, which subserves the rule-governed combination of lexical items into complex representations, depends on a distinct neural system. This system, which is composed of a network of specific frontal, basal-ganglia, parietal and cerebellar structures, underlies procedural memory, which supports the learning and execution of motor and cognitive skills, especially those involving sequences. The functions of the two brain systems, together with their anatomical, physiological and biochemical substrates, lead to specific claims and predictions regarding their roles in language. These predictions are compared with those of other neurocognitive models of language. Empirical evidence is presented from neuroimaging studies of normal language processing, and from developmental and adult-onset disorders. It is argued that this evidence supports the DP model. It is additionally proposed that “language” disorders, such as specific language impairment and non-fluent and fluent aphasia, may be profitably viewed as impairments primarily affecting one or the other brain system. -
Procedural and Declarative Memory in Children with Developmental Disorders of Language and Literacy
Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 917 Procedural and Declarative Memory in Children with Developmental Disorders of Language and Literacy MARTINA HEDENIUS ACTA UNIVERSITATIS UPSALIENSIS ISSN 1651-6206 ISBN 978-91-554-8707-2 UPPSALA urn:nbn:se:uu:diva-204245 2013 Dissertation presented at Uppsala University to be publicly examined in Gustavianum, Uppsala, Friday, September 13, 2013 at 13:15 for the degree of Doctor of Philosophy (Faculty of Medicine). The examination will be conducted in English. Abstract Hedenius, M. 2013. Procedural and Declarative Memory in Children with Developmental Disorders of Language and Literacy. Acta Universitatis Upsaliensis. Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 917. 96 pp. Uppsala. ISBN 978-91-554-8707-2. The procedural deficit hypothesis (PDH) posits that a range of language, cognitive and motor impairments associated with specific language impairment (SLI) and developmental dyslexia (DD) may be explained by an underlying domain-general dysfunction of the procedural memory system. In contrast, declarative memory is hypothesized to remain intact and to play a compensatory role in the two disorders. The studies in the present thesis were designed to test this hypothesis. Study I examined non-language procedural memory, specifically implicit sequence learning, in children with SLI. It was shown that children with poor performance on tests of grammar were impaired at consolidation of procedural memory compared to children with normal grammar. These findings support the PDH and are line with previous studies suggesting a link between grammar processing and procedural memory. In Study II, the same implicit sequence learning paradigm was used to test procedural memory in children with DD. -

First Direct Evidence of Two Stages in Free Recall and Three Corresponding Estimates of Working Memory Capacity
1 Running head: First direct evidence of two stages in free recall First direct evidence of two stages in free recall and three corresponding estimates of working memory capacity Eugen Tarnow, Ph.D.1 18-11 Radburn Road, Fair Lawn, NJ 07410, USA [email protected] Abstract I find that exactly two stages can be seen directly in sequential free recall distributions. These distributions show that the first three recalls come from the emptying of working memory, recalls 6 and above come from a second stage and the 4th and 5th recalls are mixtures of the two. A discontinuity, a rounded step function, is shown to exist in the fitted linear slope of the recall distributions as the recall shifts from the emptying of working memory (positive slope) to the second stage (negative slope). The discontinuity leads to a first estimate of the capacity of working memory at 4-4.5 items. Working memory accounts for the recency effect. The primacy effect comes from the second stage with a contribution also from working memory for short lists (the first item). The different slopes of the working memory and secondary stages, and that the two have different functional forms, accounts for the u-shaped serial position curve. The total recall is shown to be a linear combination of the content of working memory and items recalled in the second stage with 3.0-3.9 items coming from working memory, a second estimate of the capacity of working memory. A third, separate upper limit on the capacity of working memory is found (3.06 items), corresponding to the requirement that the content of working memory cannot exceed the total recall, item by item. -

Okami Study Guide: Chapter 8 1
Okami Study Guide: Chapter 8 1 Chapter in Review 1. Memory may be defined as a group of mechanisms and systems that encode, store, and retrieve information. The modal model of memory describes three stages and stores in the memory process: sensory memory, short-term memory (STM), and long- term memory (LTM). 2. Sensory memory very briefly stores fleeing sensory impressions for further processing in STM and LTM. Sensory memory is divided into two categories: iconic store, which stores fleeting visual impressions; and echoic store, which stores fleeting auditory impressions. In addition to storing sensory impressions for further processing, sensory memory allows us to perceive the world as a continuous stream of events instead of a series of “snapshots.” 3. When you consciously or unconsciously decide to pay attention to specific pieces of information in sensory memory, the information is transferred into short-term memory. The duration and capacity of STM are limited. In general, information can remain in STM for no longer than 20 seconds unless maintenance rehearsal takes place, and no more than 4 single items or chunks of information can be held in STM at any one time. A chunk is any grouping of items that are strongly associated with one another. 4. Long-term memory (LTM) is theoretically limitless and relatively permanent. Information moves from STM to LTM when it is encoded in one of three ways: through sound (acoustic encoding), imagery (visual encoding), or meaning (semantic encoding). Encoding in STM tends to be primarily acoustic, secondarily visual, and much less often semantic. However, encoding in LTM is most effective if it is semantic. -

The Relationship Between Sleep, Working Memory, and Decision Making in Young and Old Adult Populations
University of Central Florida STARS Honors Undergraduate Theses UCF Theses and Dissertations 2017 The Relationship Between Sleep, Working Memory, and Decision Making in Young and Old Adult Populations Melissa G. Merz University of Central Florida Part of the Behavioral Neurobiology Commons, Cognition and Perception Commons, Cognitive Neuroscience Commons, Cognitive Psychology Commons, and the Industrial and Organizational Psychology Commons Find similar works at: https://stars.library.ucf.edu/honorstheses University of Central Florida Libraries http://library.ucf.edu This Open Access is brought to you for free and open access by the UCF Theses and Dissertations at STARS. It has been accepted for inclusion in Honors Undergraduate Theses by an authorized administrator of STARS. For more information, please contact [email protected]. Recommended Citation Merz, Melissa G., "The Relationship Between Sleep, Working Memory, and Decision Making in Young and Old Adult Populations" (2017). Honors Undergraduate Theses. 210. https://stars.library.ucf.edu/honorstheses/210 THE RELATIONSHIP BETWEEN SLEEP, WORKING MEMORY, AND DECISION MAKING IN YOUNG AND OLD ADULT POPULATIONS by MELISSA G. MERZ A thesis submitted in partial fulfillment of the requirements for the Honors in the Major Program in Psychology in the College of Sciences and in the Burnett Honors College at the University of Central Florida Orlando, Florida Spring Term 2017 Thesis Chair: Dr. Nichole Lighthall ©2017 Melissa G. Merz ii Abstract Sleep is known to influence basic tasks concerning working memory, reaction time and executive functioning (Silva, Wang, Ronda, Wyatt, & Duffy, 2010; Nebes, Buysse, Halligan, Houck, & Monk, 2009). However, the amount that sleep influences these functions varies from study to study possibly due to differences in age and task design.