Effecrs of NITROGEN NARCOSIS and HYPERCAPNIA on MEMORY
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dysbarism - Barotrauma
DYSBARISM - BAROTRAUMA Introduction Dysbarism is the term given to medical complications of exposure to gases at higher than normal atmospheric pressure. It includes barotrauma, decompression illness and nitrogen narcosis. Barotrauma occurs as a consequence of excessive expansion or contraction of gas within enclosed body cavities. Barotrauma principally affects the: 1. Lungs (most importantly): Lung barotrauma may result in: ● Gas embolism ● Pneumomediastinum ● Pneumothorax. 2. Eyes 3. Middle / Inner ear 4. Sinuses 5. Teeth / mandible 6. GIT (rarely) Any illness that develops during or post div.ing must be considered to be diving- related until proven otherwise. Any patient with neurological symptoms in particular needs urgent referral to a specialist in hyperbaric medicine. See also separate document on Dysbarism - Decompression Illness (in Environmental folder). Terminology The term dysbarism encompasses: ● Decompression illness And ● Barotrauma And ● Nitrogen narcosis Decompression illness (DCI) includes: 1. Decompression sickness (DCS) (or in lay terms, the “bends”): ● Type I DCS: ♥ Involves the joints or skin only ● Type II DCS: ♥ Involves all other pain, neurological injury, vestibular and pulmonary symptoms. 2. Arterial gas embolism (AGE): ● Due to pulmonary barotrauma releasing air into the circulation. Epidemiology Diving is generally a safe undertaking. Serious decompression incidents occur approximately only in 1 in 10,000 dives. However, because of high participation rates, there are about 200 - 300 cases of significant decompression illness requiring treatment in Australia each year. It is estimated that 10 times this number of divers experience less severe illness after diving. Physics Boyle’s Law: The air pressure at sea level is 1 atmosphere absolute (ATA). Alternative units used for 1 ATA include: ● 101.3 kPa (SI units) ● 1.013 Bar ● 10 meters of sea water (MSW) ● 760 mm of mercury (mm Hg) ● 14.7 pounds per square inch (PSI) For every 10 meters a diver descends in seawater, the pressure increases by 1 ATA. -

Nitrogen Narcosis
WHAT IS IT? A reversible alteration in consciousness that occurs while at depth (usually noticeable around 30 meters or 100 ft) Caused by the anesthetic effect of certain gases at high pressure NITROGEN NARCOSIS Depths Beyond 100 Feet! Individual Variability Day-to-Day Variability Signs and Symptoms of N2 Narcosis Impaired performance mental/manual work Dizziness, euphoria, intoxication Overconfidence Uncontrolled laughter Overly talkative Memory loss/post-dive amnesia Perceptual narrowing Impaired sensory function Loss of consciousness > 300 ft Deep Scuba Dives Breathing Air YEAR DIVER DEPTH 1943 Dumas 203 feet 1948 Dumas 307 feet 1967 Watts 390 feet 1968 Watson 437 feet 1989 Gilliam 452 feet Prevention of Nitrogen Narcosis Restrict diving depth to less than 100 fsw If affected, return immediately to surface Plan dive beforehand − Max time to be on bottom − Any decompression required − Minimum air required for ascent − Emergency action in event of accident Breathe helium/oxygen mixture How to Beat Narcosis (Francis 2006) Be sober, no hangover and drug free Be rested and confident Use a high quality regulator Avoid task loading Be over trained Approach limits gradually Use a slate to plan dive Schedule gauge checks and buddy checks Be positive, well motivated and prudent Oxygen Characteristics: − Colorless − Odorless − Tasteless Disadvantage: − Toxic when Oxygen is the only gas excessive amounts metabolized by the human body are breathed under pressure Too much or too little oxygen is dangerous! Oxygen Toxicity -

Outta Gas (From the 2007: Exploring the Inner Space of the Celebes Sea
2007: Exploring the Inner Space of the Celebes Sea Outta Gas FOCUS MAXIMUM NUMBER OF STUDENTS Gas laws 30 GRADE LEVEL KEY WORDS 9-12 (Chemistry/Physics) Celebes Sea SCUBA diving FOCUS QUESTION Gas laws How can Boyle’s Law, Charles’ Law, Gay-Lussac’s Ideal Gas Law Law, Henry’s Law, and Dalton’s Law be used to Boyle’s Law predict the behavior of gases used in SCUBA div- Charles’ Law ing? Gay-Lussac’s Law Henry’s Law LEARNING OBJECTIVES Dalton’s Law Students will define Boyle’s Law, Charles’ Law, Pressure Gay-Lussac’s Law, Henry’s Law, and Dalton’s Law. Worksheet Mathematics Students will use Boyle’s Law, Charles’ Law, Gay- Lussac’s Law, Henry’s Law, and Dalton’s Law to BACKGROUND INFORMATION solve practical problems related to SCUBA diving. Indonesia is well-known as one of Earth’s major centers of biodiversity. Although Indonesia cov- MATERIALS ers only 1.3 percent of Earth’s land surface, it “Blue Water Diving Worksheet,” one copy for includes: each student or student group • 10 percent of the world’s flowering plant species; AUDIO/VISUAL MATERIALS • 12 percent of the world’s mammal species; None • 16 percent of all reptile and amphibian species; and TEACHING TIME • 17 percent of the world’s bird species. One or two 45-minute class periods plus time for students to complete worksheet In addition, together with the Philippines and Great Barrier Reef, this region has more species SEATING ARRANGEMENT of fishes, corals, mollusks, and crustaceans than Classroom style any other location on Earth. -

Masteringphysics: Assignmen
MasteringPhysics: Assignment Print View http://session.masteringphysics.com/myct/assignmentPrint... Manage this Assignment: Chapter 18 Due: 12:00am on Saturday, July 3, 2010 Note: You will receive no credit for late submissions. To learn more, read your instructor's Grading Policy A Law for Scuba Divers Description: Find the increase in the concentration of air in a scuba diver's lungs. Find the number of moles of air exhaled. Also, consider the isothermal expansion of air as a freediver diver surfaces. Identify the proper pV graph. Associated medical conditions discussed. SCUBA is an acronym for self-contained underwater breathing apparatus. Scuba diving has become an increasingly popular sport, but it requires training and certification owing to its many dangers. In this problem you will explore the biophysics that underlies the two main conditions that may result from diving in an incorrect or unsafe manner. While underwater, a scuba diver must breathe compressed air to compensate for the increased underwater pressure. There are a couple of reasons for this: 1. If the air were not at the same pressure as the water, the pipe carrying the air might close off or collapse under the external water pressure. 2. Compressed air is also more concentrated than the air we normally breathe, so the diver can afford to breathe more shallowly and less often. A mechanical device called a regulator dispenses air at the proper (higher than atmospheric) pressure so that the diver can inhale. Part A Suppose Gabor, a scuba diver, is at a depth of . Assume that: 1. The air pressure in his air tract is the same as the net water pressure at this depth. -

Nitrogen Narcosis in Hyperbaric Chamber Nurses
International Journal of Research in Nursing Original Research Paper Nitrogen Narcosis in Hyperbaric Chamber Nurses 1,2 Denise F. Blake, 3Derelle A. Young and 4Lawrence H. Brown 1Emergency Department, The Townsville Hospital, Douglas, Queensland, Australia 2School of Marine and Tropical Biology, James Cook University, Townsville, Queensland, 4814, Australia 3Hyperbaric Medicine Unit, The Townsville Hospital, Townsville, Queensland, Australia 4Mount Isa Centre for Rural and Remote Health, Faculty of Medicine, Health and Molecular Sciences, James Cook University, Townsville, QLD, 4814, Australia Article history Abstract: Hyperbaric nursing has become a specialty requiring high skill Received: 24-09-2014 and knowledge. Nitrogen narcosis is a perceived risk for all inside Revised: 03-10-2014 hyperbaric chamber nurses. The actual degree of impairment at pressure Accepted: 16-12-2015 has not been quantified. Twenty eight subjects participated in the study. Sixteen hyperbaric nurse candidates and five experienced hyperbaric Corresponding Author: Denise F. Blake, nurses completed Trail Making Test A (TMTA) pre and post compression Emergency Department, and at 180 kPa and 300 kPa. Seven experienced hyperbaric staff acted as The Townsville Hospital, an unpressurized reference. Time to completion of the test was recorded in Douglas, Queensland, Australia seconds; pre-test anxiety and perceived symptoms of narcosis at 300 kPa Email: [email protected] were also recorded. There were no statistically significant differences in the corrected TMT A times at the four different time periods. There was a trend to poorer performance by the nurse candidates at 180 kPa however this was not statistically significant. Most subjects felt some degree of narcosis at 300 kPa. -

Diving Physics and "Fizzyology"
Phys Diving Physics and "Fizzyology" Introduction Like all animals, human beings need oxygen in order to survive. When we breathe, we extract oxygen from the air, and use that oxygen for metabolism, which is how we convert the food we eat into useable energy to do the things that we do. One of the by-products of metabolism is carbon dioxide; whenever we exhale, we are getting rid of the carbon dioxide that our bodies produce. The main purpose of breathing, therefore, is to provide our bodies with oxygen, and rid our bodies of carbon dioxide. We humans are terrestrial (land-dwelling) mammals, and as such, our lungs are designed to breathe gas. Unlike fishes, we have no gills, so we cannot breathe water. Therefore, the first problem we must overcome to explore the underwater realm is a means to provide breathing gas. However, if this were the only barrier humans must overcome to enter the sea, we would have long-ago discovered most of the mysteries of the ocean. All we would need to remain underwater indefinitely would be a long tube going to the surface -- a huge snorkel -- through which we could breathe. Unfortunately, there is another problem we must over come when descending to the depths -- a problem with far more complex and difficult consequences. That problem is pressure. Pressure Have you ever wondered why nobody makes snorkels that are ten, or twenty, or a hundred feet long? The answer becomes obvious as soon as you try to breathe through a snorkel when your body is more than two or three feet (~1 meter) beneath the surface of the water. -
Gas Issues in Diving Gas Issues • TOO MUCH
Gas Issues in Diving Gas Issues • TOO MUCH • O2, CO2, inert gas narcosis, High Pressure Neurological Syndrome • TOO LITTLE • Hypoxia, hyperventilation • WRONG GAS • CO poisoning, contaminants CNS Ox Tox “VENTID-C” • Vision changes (↓acuity, dazzle, lat • Risk Factors movement, constricted fields) • Exercise • Ears (tinnitus, auditory hallucinations, • Hyper/hypothermia music, bells, knocking) • Hypoventilation, hypercapnia • Immersion • Nausea/vomiting • Metabolic activity, blood flow to brain • Twitch (lips, cheek, eyelid, tremors…) • Hypoglycemia (DM) • Irritability, behaviour, mood changes • Seizure D?O, +/- meds that lower sx (incl apprehension, apathy, euphoria) threshold • VitE deficiency • Dizzy • Pseudoephedrine, amphetamines, ASA, • Convulsions acetazolamide • Spherocytosis, hypercortisolism • Also pallor, sweaty, palpitations, brady, tachy, panting, grunting, unpleasant gustatory/ olfactory sensations, hiccups CNS OxTox • No consistent pre-convulsion • Tx warning sx • Remove O2 • • Stop travel Often not preceded by other sx • Protect from injuries if seizing • O2 convulsions not inherently • Check DDx (don’t forget hypoglycemia) harmful • Keep patient off O2 for 15 mins after all sx are gone • No pathologic changes in human • Ignore treatment time lost and resume brain, no evidence of clinical sequelae table where last interrupted • No apparent predisposition to future • Don’t forget to compensate for extra sz disorder time for chamber attendants • Harm based on context (seizure • Preventive Measures underwater = drowning) • -

Diving Physiology 3
Diving Physiology 3 SECTION PAGE SECTION PAGE 3.0 GENERAL ...................................................3- 1 3.3.3.3 Oxygen Toxicity ........................3-21 3.1 SYSTEMS OF THE BODY ...............................3- 1 3.3.3.3.1 CNS: Central 3.1.1 Musculoskeletal System ............................3- 1 Nervous System .........................3-21 3.1.2 Nervous System ......................................3- 1 3.3.3.3.2 Lung and 3.1.3 Digestive System.....................................3- 2 “Whole Body” ..........................3-21 3.2 RESPIRATION AND CIRCULATION ...............3- 2 3.2.1 Process of Respiration ..............................3- 2 3.3.3.3.3 Variations In 3.2.2 Mechanics of Respiration ..........................3- 3 Tolerance .................................3-22 3.2.3 Control of Respiration..............................3- 4 3.3.3.3.4 Benefits of 3.2.4 Circulation ............................................3- 4 Intermittent Exposure..................3-22 3.2.4.1 Blood Transport of Oxygen 3.3.3.3.5 Concepts of and Carbon Dioxide ......................3- 5 Oxygen Exposure 3.2.4.2 Tissue Gas Exchange.....................3- 6 Management .............................3-22 3.2.4.3 Tissue Use of Oxygen ....................3- 6 3.3.3.3.6 Prevention of 3.2.5 Summary of Respiration CNS Poisoning ..........................3-22 and Circulation Processes .........................3- 8 3.2.6 Respiratory Problems ...............................3- 8 3.3.3.3.7 The “Oxygen Clock” 3.2.6.1 Hypoxia .....................................3- -

Autopsy & the Investigation of Scuba Diving Fatalities
Autopsy & the Investigation of Scuba Diving Fatalities Contents 1. Investigation ............................................................................................ 1 1.1. Apparatus............................................................................................. 1 2. Causes of Death in Divers....................................................................... 2 2.1. Decreased level of consciousness....................................................... 2 2.2. Decompression sickness ..................................................................... 3 2.3. Natural disease .................................................................................... 4 2.4. Physical injury ...................................................................................... 4 2.5. Error in judgement ............................................................................... 4 3. Post Mortem Examination ....................................................................... 5 3.1. The history ........................................................................................... 5 3.2. Body storage........................................................................................ 6 3.3. Radiological examination for gas as part of the post mortem examination................................................................................................. 6 3.4. Autopsy................................................................................................ 8 4. External Examination.............................................................................. -
Problems with Pressure
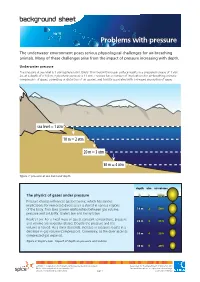
background sheet Problems with pressure The underwater environment poses serious physiological challenges for air-breathing animals. Many of these challenges arise from the impact of pressure increasing with depth. Underwater pressure The pressure at sea level is 1 atmosphere (atm). Every 10 m below the ocean surface results in a pressure increase of 1 atm. So, at a depth of a 100 m, hydrostatic pressure is 11 atm. Pressure has a number of implications for air-breathing animals: compression of gases; squeezing or distortion of air spaces; and toxicity associated with increased absorption of gases. sea level = 1 atm 10 m = 2 atm 20 m = 3 atm 30 m = 4 atm figure 1: pressure at sea level and depth depth atm air volume The physics of gases under pressure 0 1 100% Pressure change influences gas behaviour, which has serious implications for immersed divers as air is stored in various regions of the body. Two laws govern relationships between gas volume, 1010m m 2 50% pressure and solubility: Boyle’s law and Henry’s law. Boyle’s Law: For a fixed mass of gas at constant temperature, pressure 2020m m 3 33% and volume are inversely related. Double the pressure and the volume is halved. As a diver descends, increase in pressure results in a decrease in gas volume (compression). Conversely, as the diver ascends 3030m m 4 25% compressed gas expands. figure 2: Boyle’s Law - impact of depth on pressure and volume 4040m m 5 20% ast0850 | Adaptations 6: Problems with pressure (background sheet) developed for the Department of Education WA © The University of Western Australia 2012 for conditions of use see spice.wa.edu.au/usage version 1.0 reviewed October 2012 page 1 Licensed for NEALS Henry’s Law: At constant temperature, the amount Risks for human divers of gas that dissolves in solution increases with gas pressure. -

Diving and the Risk of Barotrauma
S20 Thorax 1998;53(Suppl 2):S20±S24 Thorax: first published as 10.1136/thx.53.2008.S20 on 1 August 1998. Downloaded from Diving and the risk of barotrauma Erich W Russi Pulmonary Division, Department of Internal Medicine, University Hospital Zurich, Switzerland Introductory article Risk factors for pulmonary barotrauma in divers K Tetzlaff, M Reuter, B Leplow, M Heller, E Bettinghausen Study objectives. Pulmonary barotrauma (PBT) of ascent is a feared complication in compressed air diving. Although certain respiratory conditions are thought to increase the risk of suffering PBT and thus should preclude diving, in most cases of PBT, risk factors are described as not being present. The purpose of our study was to evaluate factors that possibly cause PBT. Design. We analyzed 15 consecutive cases of PBT with respect to dive factors, clinical and radiologic features, and lung function. They were compared with 15 cases of decompression sickness without PBT, which appeared in the same period. Results. Clinical features of PBT were arterial gas embolism (n=13), mediastinal emphysema (n=1), and pneumothorax (n=1). CT of the chest (performed in 12 cases) revealed subpleural emphysematous blebs in 5 cases that were not detected in preinjury and postinjury chest radiographs. A comparison of predive lung function between groups showed signi®cantly lower midexpiratory ¯ow rates at 50% and 25% of vital capacity in PBT patients (p<0.05 and p<0.02, respectively). Conclusions. These results indicate that divers with preexisting small lung cysts and/or end-expiratory ¯ow limitation may be at http://thorax.bmj.com/ risk of PBT. -
Oxygen Toxicity & Nitrogen Narcosis
N2 narcosis Mattijn Buwalda Anaesthesiologist-intensivist & DMP www.mattijnb.nl Runtime: 25 min Slides: 22 Nitrogen narcosis Air dive @ 47 meter https://youtu.be/0fD1gsLlqMY N2 narcosis - symptoms • slowing of mentation • loss of memory • overconfidence • excitement • euphoria • hallucinations • stupefaction • coma Neuro cognitive effects • Noticeable from 30 msw (average) • 10–20 msw: impairment of unrehearsed mental and physical tasks, such as sorting cards • 30-50 msw: central processing affected > amnesia • decreased pain perception! • decreased manual dexterity, reaction times • linear to depth • automated motor skills are relatively preserved Kowalski JT, Seidack S, Klein F, Varn A, Rottger S, Kahler W, et al. Does inert gas narcosis have an influence on perception of pain? Undersea Hyperb Med. 2012;39:569–76. Kneller W, Hobbs M. Inert gas narcosis and the encoding and retrieval of long-term memory. Aviat Space Environ Med. 2013;84:1235–9. Poulton EC, Catton MJ, Carpenter A. Efficiency at sorting cards in compressed air. Br J Ind Med. 1964;21:242–5. Neuro cognitive effects N2 narcosis - history • Early report by Colladon 1826: “a state of exicitement as if I had drunk some alcoholic liquor” • Green 1861: sleepiness, hallucinations • Damant 1930: loss of memory • Hill 1933: semi loss of consciousness attributed to: – impure air from faulty compressors – carbon dioxide • Behnke 1935 recognized N2 as the culprit Inert gas narcosis • Traditional view: – expansion of the phospholipid bilayer by uptake of inert gas – fluidization of the gel like bilayer – pressure reversal of anaesthetic effect • Modern view: – interaction with membrane proteins – ligand-gated ion channels Molecular and basic mechanisms of anaesthesia (postgraduate issue).