Going to Extremes of Lung Physiology–Deep Breath-Hold Diving
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

What Every Physician Should Know About Doping and Doping Control O Que Todo Médico Deveria Conhecer Sobre Doping E Controle Antidoping
WHATCOMMUNICATION EVERY PHYSICIAN SHOULD KNOW ABOUT DOPING AND DOPING CONTROL What every physician should know about doping and doping control O QUE TODO MÉDICO DEVERIA CONHECER SOBRE DOPING E CONTROLE ANTIDOPING JOSÉ KAWAZOE LAZZOLI1 1Adjunct Professor, Instituto Biomédico, Universidade Federal Fluminense. Specialist in Sports Medicine from Sociedade Brasileira de Medicina do Exercício e do Esporte (SBMEE) and Cardiology from Sociedade Brasileira de Cardiologia (SBC). Former President of the Brazilian Society of Sports Medicine (2009/2011). Secretary General of the Panamerican Confederation of Sports Medicine (Copamede). Treasurer of the International Federation of Sports Medicine (FIMS), Rio de Janeiro, RJ, Brazil http://dx.doi.org/10.1590/1806-9282.62.02.101 Probably the medical professional who is closer to the teria are present in a substance or a method, the theoret- daily life of an athlete, who participates regularly in com- ical possibility of listing occurs. petitions, whether or not high-performance, is the expert Examples of artificial performance enhancement in- in exercise and sports medicine. However, occasionally clude anabolic steroids, which also cause serious risks to the athlete may need to resort to other medical profes- the health of the athlete. This group of substances in- sionals, for various reasons, such as a general practitio- cludes two of the three basic principles of the concept of ner, a dermatologist, a cardiologist, an orthopedist or a doping, and therefore makes the list. gastroenterologist. Therefore, every physician is subject The concept of “violating the spirit of sport” can give to come across a patient who is an intermediate level or rise to subjective interpretations, but these values are ex- high-performance athlete, and will need to go through plained in WADA World Anti-Doping Code as follows: eth- doping controls throughout his sporting life. -

You're Listening to Ocean Currents, a Podcast Brought to You by NOAA's Cordell Bank National Marine Sanctuary
1 July 7th, 2014, oc070714.mp3 Free Diving and El Nino 2014 Jennifer Stock, Francesca Koe, Logan Johnson Jennifer Stock: You're listening to Ocean Currents, a podcast brought to you by NOAA's Cordell Bank National Marine Sanctuary. This radio program was originally broadcast on KWMR in Point Reyes Station, California. Thanks for listening! Welcome to another edition of Ocean Currents, I'm your host, Jennifer Stock. On this show I talk with scientists, educators, explorers, policy-makers, ocean enthusiasts, adventurers and more, all uncovering and learning about the mysterious and vital part of our planet: the blue ocean. I bring this show to you monthly on KWMR from NOAA's Cordell Bank National Marine Sanctuary, one of four national marine sanctuaries in California all working to protect unique and biologically diverse ecosystems. Cordell bank is located just offshore of the KWMR listening radius off the Marin-Sonoma coast, and it's thriving with ocean life above and below the surface. The ocean holds so many mysteries to us: the habitats, the life, the mysterious ways it moves and mixes, its temperatures, its ability to absorb carbon dioxide. And as a species-- as humans-- we've made great strides on being able to enter it and see it below the surface with technology aiding greatly. Before scuba was invented we were limited by our breath to explore underwater, and this is how humans first accessed the sea, and today we still access the sea this way. If you've ever held your breath underwater before you have been free diving. -

Upper Respiratory Tract and Aural Flora of Saturation Divers
J Clin Pathol: first published as 10.1136/jcp.31.8.721 on 1 August 1978. Downloaded from Journal of Clinical Pathology, 1978, 31, 721-723 Upper respiratory tract and aural flora of saturation divers D. M. JONES AND P. DAVIS From the Department ofBacteriology, Withington Hospital, Manchester M20 8LR, UK SUMMARY The conditions of helium saturation diving promote the proliferation of Gram-negative bacterial species in the external auditory meatus of divers. These changes in flora occurred in the absence of operational diving, that is, no contact with water. The colonising bacteria were auto- genous in origin and cross-colonisation was observed between divers. On return to normal atmos- pheric conditions the aural flora became predominantly Gram-positive again within 48 hours. The slow return to normal pressures by deep-sea a high ambient temperature (30°-350C), and the divers, necessary to avoid decompression sickness, relative humidity is high. restricts the period that can be maintained at depth. Underwater exploration is a relatively new indus- This problem is overcome by the saturation diving try and by its nature is extremely dangerous. It is technique whereby the divers are maintained at high important that divers remain fit during the conduct of pressure in their living quarters and are transported a saturation dive because if a diver becomes unwell to the sea bed in a detachable diving bell. The com- the extreme slowness with which decompression can copyright. pression chamber and transfer chamber are anchored be carried out means that immediate medical atten- to the deck of an oil production platform, and the tion is not readily available. -

Download Transcript
SCIENTIFIC AMERICAN FRONTIERS PROGRAM #1503 "Going Deep" AIRDATE: February 2, 2005 ALAN ALDA Hello and welcome to Scientific American Frontiers. I'm Alan Alda. It's said that the oceans, which cover more than two thirds of the earth's surface, are less familiar to us than the surface of the moon. If you consider the volume of the oceans, it's actually more than ninety percent of the habitable part of the earth that we don't know too much about. The main reason for our relative ignorance is simply that the deep ocean is an absolutely forbidding environment. It's pitch dark, extremely cold and with pressures that are like having a 3,000-foot column of lead pressing down on every square inch -- which does sound pretty uncomfortable. In this program we're going to see how people finally made it to the ocean floor, and we'll find out about the scientific revolutions they brought back with them. We're going to go diving in the Alvin, the little submarine that did so much of the work. And we're going to glimpse the future, as Alvin's successor takes shape in a small seaside town on Cape Cod. That's coming up in tonight's episode, Going Deep. INTO THE DEEP ALAN ALDA (NARRATION) Woods Hole, Massachusetts. It's one of the picturesque seaside towns that draw the tourists to Cape Cod each year. But few seaside towns have what Woods Hole has. For 70 years it's been home to the Woods Hole Oceanographic Institution — an organization that does nothing but study the world's oceans. -

Freediving Catalog 2014
Freediving 2014 760B2EG 760B3EG 760B4EG 760B5EG E-GLASS DESCRIPTION Our most popular and all around bifins. The lenght of the blade is compatible with dynamic and constant weight apnea. Composite blades to stock up on maximum energy throughout the bending. TECHNOLOGY Technology : prepreg curing process Fabric : E-glass Resin : epoxy Performance : 30 to 40% more responsive than plastic SPECIFICATIONS Height of blade : 760 mm Width of blade : 210 mm Flat blade for made-to-measure footpocket (free heel) Blade with an angle of 15° to fit in full footpocket 4 kinds of varying hardness that are most likely to suit your style and body type : 760B2EG : soft, dynamic apnea 760B3EG : medium, dynamic and constant weight apnea 760B4EG : hard, constant weight 760B5EG : very hard, constant weight for big guys + 90kg Weight with made-to-measure footpocket = 1,5kg Weight with full footpocket = 1,9kg T profiles along the edges to ensure a good drive and a channeling of the water FOOTPOCKETS 2 kinds of footpockets : - Made-to-measure footpocket : Size 35 to 50 (3 to 15), free heel for better stroke - Tuned full footpocket : cut out footpocket to get a lighter and more responsive swimfin. Beuchat Mundial : 41-42, 43-44, 45-46, 47-48 Imersion : 38-40, 40-42, 42-44, 44-46 Omer : 36-38, 38-40, 40-42, 42-44, 44-46, 46-48, 48-50 760B2SG 760B3SG 760B4SG 760B5SG S-GLASS DESCRIPTION Our most popular and all around bifins. The lenght of the blade is compatible with dynamic and constant weight apnea. Composite blades to stock up on maximum energy throughout the bending. -

The Physiology of Cardiopulmonary Resuscitation
Society for Critical Care Anesthesiologists Section Editor: Avery Tung E REVIEW ARTICLE CME The Physiology of Cardiopulmonary Resuscitation Keith G. Lurie, MD, Edward C. Nemergut, MD, Demetris Yannopoulos, MD, and Michael Sweeney, MD * † ‡ § Outcomes after cardiac arrest remain poor more than a half a century after closed chest cardiopulmonary resuscitation (CPR) was first described. This review article is focused on recent insights into the physiology of blood flow to the heart and brain during CPR. Over the past 20 years, a greater understanding of heart–brain–lung interactions has resulted in novel resuscitation methods and technologies that significantly improve outcomes from cardiac arrest. This article highlights the importance of attention to CPR quality, recent approaches to regulate intrathoracic pressure to improve cerebral and systemic perfusion, and ongo- ing research related to the ways to mitigate reperfusion injury during CPR. Taken together, these new approaches in adult and pediatric patients provide an innovative, physiologically based road map to increase survival and quality of life after cardiac arrest. (Anesth Analg 2016;122:767–83) udden cardiac arrest remains a leading cause of pre- during CPR, and new approaches to reduce injury associ- hospital and in-hospital death.1 Efforts to resuscitate ated with reperfusion.3,5–8,10–48 Given the debate surrounding patients after cardiac arrest have preoccupied scien- what is known, what we think we know, and what remains S 1,2 tists and clinicians for decades. However, the majority unknown about resuscitation science, this article also pro- of patients are never successfully resuscitated.1,3–5 Based vides some contrarian and nihilistic points of view. -
Notes on Diving in Ancient Egypt
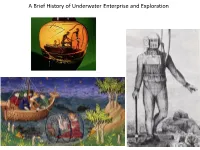
A Brief History of Underwater Enterprise and Exploration The incentives to risk one’s life underwater from the earliest records of diving: 1) Subsistence and general aquatic harvest 2) Commerce/salvage 3) Warfare A sponge diver about to take the plunge, Classical Greece ca. 500 BCE The beginnings: subsistence in Ancient Egypt: skin divers netting fish in the Nile th Tomb of Djar, 11 Dynasty (ca. 2000 BCE) ‘Pull out well! (It is) a Happy day! Measure you, measure you, for you, good great fishes’ Text and image from the tomb of Ankhtifi (ca. 2100 BCE) The beginnings: other kinds of aquatic/underwater harvest: mother of pearl (left) and sponge diving (right) Mesopotamia (southern Iraq, ca. 2500 BCE) Classical Greece (ca. 500 BCE) The so-called ‘Standard of Ur’: a mosaic of lapis lazuli A sponge diver about to take the (from the exotic region of Afghanistan) and mother of plunge with a knife and a sack, the pearl (from the exotic source of a seabed), deposited in jar was also deposited in an elite tomb an elite tomb in Mesopotamia The beginnings: in search of exotic and high value things (things difficult to access/procure) Epic of Gilgamesh (composed in Mesopotamia no later than ca. 2100 BCE) records a heroic dive after a ‘plant of immortality’ on the seabed ‘He tied heavy stones *to his feet+ They pulled him down into the deep [and he saw the plant] He took the plant though it pricked his hands He cut the heavy stones from his feet The sea cast him up upon the shore’ The value of mother of pearl and sea sponge resides, in part, in the process of procuring them The beginnings: salvaging lost cargoes (lost valuable things) Scyllias and his daughter Hydna: the first professional divers known by name, famed for salvaging huge volumes of gold and silver (tribute and booty) from a Persian fleet in the Aegean that lost many ships in a storm (ca. -

No Limits Freediving
1 No Limits Freediving "The challenges to the respiratory function of the breath-hold diver' are formidable. One has to marvel at the ability of the human body to cope with stresses that far exceed what normal terrestrial life requires." Claes Lundgren, Director, Center for Research and Education in Special Environments A woman in a deeply relaxed state floats in the water next to a diving buoy. She is clad in a figure-hugging wetsuit, a dive computer strapped to her right wrist, and another to her calf. She wears strange form-hugging silicone goggles that distort her eyes, giving her a strange bug-eyed appearance. A couple of meters away, five support divers tread water near a diving platform, watching her perform an elaborate breathing ritual while she hangs onto a metal tube fitted with two crossbars. A few meters below the buoy, we see that the metal tube is in fact a weighted sled attached to a cable descending into the dark-blue water. Her eyes are still closed as she begins performing a series of final inhalations, breathing faster and faster. Photographers on the media boats snap pictures as she performs her final few deep and long hyperventilations, eliminating carbon dioxide from her body. Then, a thumbs-up to her surface crew, a pinch of the nose clip, one final lungful of air, and the woman closes her eyes, wraps her knees around the bottom bar of the sled, releases a brake device, and disappears gracefully beneath the waves. The harsh sounds of the wind and waves suddenly cease and are replaced by the effervescent bubbling of air being released from the regulators of scuba-divers. -

Dysbarism - Barotrauma
DYSBARISM - BAROTRAUMA Introduction Dysbarism is the term given to medical complications of exposure to gases at higher than normal atmospheric pressure. It includes barotrauma, decompression illness and nitrogen narcosis. Barotrauma occurs as a consequence of excessive expansion or contraction of gas within enclosed body cavities. Barotrauma principally affects the: 1. Lungs (most importantly): Lung barotrauma may result in: ● Gas embolism ● Pneumomediastinum ● Pneumothorax. 2. Eyes 3. Middle / Inner ear 4. Sinuses 5. Teeth / mandible 6. GIT (rarely) Any illness that develops during or post div.ing must be considered to be diving- related until proven otherwise. Any patient with neurological symptoms in particular needs urgent referral to a specialist in hyperbaric medicine. See also separate document on Dysbarism - Decompression Illness (in Environmental folder). Terminology The term dysbarism encompasses: ● Decompression illness And ● Barotrauma And ● Nitrogen narcosis Decompression illness (DCI) includes: 1. Decompression sickness (DCS) (or in lay terms, the “bends”): ● Type I DCS: ♥ Involves the joints or skin only ● Type II DCS: ♥ Involves all other pain, neurological injury, vestibular and pulmonary symptoms. 2. Arterial gas embolism (AGE): ● Due to pulmonary barotrauma releasing air into the circulation. Epidemiology Diving is generally a safe undertaking. Serious decompression incidents occur approximately only in 1 in 10,000 dives. However, because of high participation rates, there are about 200 - 300 cases of significant decompression illness requiring treatment in Australia each year. It is estimated that 10 times this number of divers experience less severe illness after diving. Physics Boyle’s Law: The air pressure at sea level is 1 atmosphere absolute (ATA). Alternative units used for 1 ATA include: ● 101.3 kPa (SI units) ● 1.013 Bar ● 10 meters of sea water (MSW) ● 760 mm of mercury (mm Hg) ● 14.7 pounds per square inch (PSI) For every 10 meters a diver descends in seawater, the pressure increases by 1 ATA. -

Exploration of the Deep Gulf of Mexico Slope Using DSV Alvin: Site Selection and Geologic Character
Exploration of the Deep Gulf of Mexico Slope Using DSV Alvin: Site Selection and Geologic Character Harry H. Roberts1, Chuck R. Fisher2, Jim M. Brooks3, Bernie Bernard3, Robert S. Carney4, Erik Cordes5, William Shedd6, Jesse Hunt, Jr.6, Samantha Joye7, Ian R. MacDonald8, 9 and Cheryl Morrison 1Coastal Studies Institute, Louisiana State University, Baton Rouge, Louisiana 70803 2Department of Biology, Penn State University, University Park, Pennsylvania 16802-5301 3TDI Brooks International, Inc., 1902 Pinon Dr., College Station, Texas 77845 4Department of Oceanography and Coastal Sciences, Louisiana State University, Baton Rouge, Louisiana 70803 5Department of Organismic and Evolutionary Biology, Harvard University, 16 Divinity Ave., Cambridge, Massachusetts 02138 6Minerals Management Service, Office of Resource Evaluation, New Orleans, Louisiana 70123-2394 7Department of Geology, University of Georgia, Athens, Georgia 30602 8Department of Physical and Environmental Sciences, Texas A&M – Corpus Christi, Corpus Christi, Texas 78412 9U.S. Geological Survey, 11649 Leetown Rd., Keameysville, West Virginia 25430 ABSTRACT The Gulf of Mexico is well known for its hydrocarbon seeps, associated chemosyn- thetic communities, and gas hydrates. However, most direct observations and samplings of seep sites have been concentrated above water depths of approximately 3000 ft (1000 m) because of the scarcity of deep diving manned submersibles. In the summer of 2006, Minerals Management Service (MMS) and National Oceanic and Atmospheric Admini- stration (NOAA) supported 24 days of DSV Alvin dives on the deep continental slope. Site selection for these dives was accomplished through surface reflectivity analysis of the MMS slope-wide 3D seismic database followed by a photo reconnaissance cruise. From 80 potential sites, 20 were studied by photo reconnaissance from which 10 sites were selected for Alvin dives. -

Features of Hemodynamics of Pulmonary Circulation During the Diving Reflex
FULL COMMUNICATIONS PHYSIOLOGY Features of hemodynamics of pulmonary circulation during the diving reflex Ekaterina Podyacheva1, Tatyana Zemlyanukhina1, Lavrentij Shadrin2, and Tatyana Baranova1 1Department of General Physiology, Faculty of Biology, Saint Petersburg State University, Universitetskaya nab., 7–9, Saint Petersburg, 199034, Russian Federation 2Department of Physical Culture and Sports, Saint Petersburg State University, Universitetskaya nab., 7–9, Saint Petersburg, 199034, Russian Federation Address correspondence and requests for materials to Ekaterina Podyacheva, [email protected] Abstract The adaptive cardiovascular reactions of the human diving reflex were studied. The diving reflex was activated by submerging a face in cold water under labo- ratory conditions. Forty volunteers (aged 18–24) were examined. ECG, arterial blood pressure (ABP) and central blood flow were recorded by the impedance rheography method in resting state, during diving simulation (DS) and after apnea. During DS there is a statistically significant decrease in the dicrotic in- dex (DCI), which reflects a decrease in the resistive vessel tone and as well as diastolic index (DSI), characterizing lung perfusion. A comparison of the latent periods (LP) of an increase in ABP and a drop in DCI showed that a decrease in pulmonary vascular tone develops faster than ABP begins to increase. The LP for lowering DCI is from 0.6 to 10 s; for an increase in ABP — from 6 to 30 s. A short LP for DCI and the absence of a correlation between a decrease in ABP and DCI suggests that a decrease in pulmonary vascular tone during DS occurs reflexively and independently of a change in ABP. Keywords: diving reflex, systemic circulation, pulmonary circulation, impedan- ce rheography, plethysmography. -

APNEA TRAINING and PHYSICAL CHARACTERISTICS: ENHANCEMENT of the DIVE RESPONSE, APNEIC TIME, and RECOVERY by Nathanael Stanford A
APNEA TRAINING AND PHYSICAL CHARACTERISTICS: ENHANCEMENT OF THE DIVE RESPONSE, APNEIC TIME, AND RECOVERY by Nathanael Stanford A thesis submitted in partial fulfillment of the requirements for the degree of Master of Science in Kinesiology Boise State University May 2019 © 2019 Nathanael Stanford ALL RIGHTS RESERVED BOISE STATE UNIVERSITY GRADUATE COLLEGE DEFENSE COMMITTEE AND FINAL READING APPROVALS of the thesis submitted by Nathanael Stanford Thesis Title: Apnea Training and Physical Characteristics: Enhancement of The Dive Response, Apneic Time, and Recovery Date of Final Oral Examination: 08 March 2019 The following individuals read and discussed the thesis submitted by student Nathanael Stanford, and they evaluated his presentation and response to questions during the final oral examination. They found that the student passed the final oral examination. Shawn R. Simonson, Ed.D. Chair, Supervisory Committee Timothy R. Kempf, Ph.D. Member, Supervisory Committee Jeffrey M. Anderson, MA Member, Supervisory Committee The final reading approval of the thesis was granted by Shawn R. Simonson, Ed.D., Chair of the Supervisory Committee. The thesis was approved by the Graduate College. ACKNOWLEDGEMENTS I would first like to thank my thesis advisor, Shawn Simonson for his continual assistance and guidance throughout this master thesis. He fostered an environment that encouraged me to think critically about the scientific process. The mentorship he offered directed me on a path of independent thinking and learning. I would like to thank my research technician, Sarah Bennett for the hundreds of hours she assisted me during data collection. This thesis would not have been possible without her help. To my committee member Tim Kempf, I want to express my gratitude for his assistance with study design and the scientific writing process.