Buyer Beware: Exotic Snakebite
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(Equatorial Spitting Cobra) Venom a P
The Journal of Venomous Animals and Toxins including Tropical Diseases ISSN 1678-9199 | 2011 | volume 17 | issue 4 | pages 451-459 Biochemical and toxinological characterization of Naja sumatrana ER P (Equatorial spitting cobra) venom A P Yap MKK (1), Tan NH (1), Fung SY (1) RIGINAL O (1) Department of Molecular Medicine, Center for Natural Products and Drug Research (CENAR), Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia. Abstract: The lethal and enzymatic activities of venom from Naja sumatrana (Equatorial spitting cobra) were determined and compared to venoms from three other Southeast Asian cobras (Naja sputatrix, Naja siamensis and Naja kaouthia). All four venoms exhibited the common characteristic enzymatic activities of Asiatic cobra venoms: low protease, phosphodiesterase, alkaline phosphomonoesterase and L-amino acid oxidase activities, moderately high acetylcholinesterase and hyaluronidase activities and high phospholipase A2. Fractionation of N. sumatrana venom by Resource® S cation exchange chromatography (GE Healthcare, USA) yielded nine major protein peaks, with all except the acidic protein peak being lethal to mice. Most of the protein peaks exhibit enzymatic activities, and L-amino acid oxidase, alkaline phosphomonoesterase, acetylcholinesterase, 5’-nucleotidase and hyaluronidase exist in multiple forms. Comparison of the Resource® S chromatograms of the four cobra venoms clearly indicates that the protein composition of N. sumatrana venom is distinct from venoms of the other two spitting cobras, N. sputatrix (Javan spitting cobra) and N. siamensis (Indochinese spitting cobra). The results support the revised systematics of the Asiatic cobra based on multivariate analysis of morphological characters. The three spitting cobra venoms exhibit two common features: the presence of basic, potentially pharmacologically active phospholipases A2 and a high content of polypeptide cardiotoxin, suggesting that the pathophysiological actions of the three spitting cobra venoms may be similar. -

Fibrinogenolytic Toxin from Indian Monocled Cobra (Naja Kaouthia) Venom
Fibrinogenolytic toxin from Indian monocled cobra (Naja kaouthia) venom CCHANDRA SEKHAR and DIBAKAR CHAKRABARTY* Department of Biological Sciences, Birla Institute of Technology and Science–Pilani, KK Birla Goa Campus, Zuarinagar, Goa 403 726, India *Corresponding author (Fax, +91-832-255-7033; Email, [email protected], [email protected]) A fibrinogenolytic toxin of molecular weight 6.5 kDa has been purified from the venom of Indian monocled cobra (Naja kaouthia) by repeated cation exchange chromatography on CM-sephadex C-50. The purified toxin did not show any phospholipase activity but was mildly hemolytic on human erythrocytes. This toxin, called Lahirin, cleaved fibrinogen in a dose- and time-dependent manner. The digestion process apparently started with the Aα chain, and gradually other lower-molecular-weight chains were also cleaved to low-molecular-weight peptides. The fibrinolytic activity was completely lost after treatment with ethylene di-amine tetra acetic acid (EDTA). However, exposure to 100°C for 1 min or pre-treatment with phenyl methyl sulfonyl fluoride (PMSF) did not affect the fibrinolytic activity. Cleavage of di-sulphide bonds by β-mercaptoethanol or unfolding the protein with 4 M urea caused complete loss of activity of pure Lahirin. [Chandra Sekhar C and Chakrabarty D 2011 Fibrinogenolytic toxin from Indian monocled cobra (Naja kaouthia) venom. J. Biosci. 36 355–361] DOI 10.1007/s12038-011-9068-3 1. Introduction venom. However, in the course of the present study, these authors came across several anticoagulant/fibrinogenolytic Monocled and spectacled cobras are the most frequently factors of wide-ranging molecular weights (MWs) in mono- encountered venomous snakes in India. -
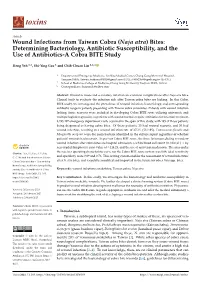
Naja Atra) Bites: Determining Bacteriology, Antibiotic Susceptibility, and the Use of Antibiotics-A Cobra BITE Study
toxins Article Wound Infections from Taiwan Cobra (Naja atra) Bites: Determining Bacteriology, Antibiotic Susceptibility, and the Use of Antibiotics-A Cobra BITE Study Heng Yeh 1,2, Shi-Ying Gao 1 and Chih-Chuan Lin 1,2,* 1 Department of Emergency Medicine, Lin-Kou Medical Center, Chang Gung Memorial Hospital, Taoyuan 33305, Taiwan; [email protected] (H.Y.); [email protected] (S.-Y.G.) 2 School of Medicine, College of Medicine, Chang Gung University, Taoyuan 33302, Taiwan * Correspondence: [email protected] Abstract: Wound necrosis and secondary infection are common complications after Naja atra bites. Clinical tools to evaluate the infection risk after Taiwan cobra bites are lacking. In this Cobra BITE study, we investigated the prevalence of wound infection, bacteriology, and corresponding antibiotic usage in patients presenting with Taiwan cobra snakebites. Patients with wound infection lacking tissue necrosis were included in developing Cobra BITE score utilizing univariate and multiple logistic regression, as patients with wound necrosis require antibiotics for infection treatment. 8,295,497 emergency department visits occurred in the span of this study, with 195 of those patients being diagnosed as having cobra bites. Of these patients, 23 had wound necrosis, and 30 had wound infection, resulting in a wound infection rate of 27.2% (53/195). Enterococcus faecalis and Morganella morganii were the main bacteria identified in the culture report regardless of whether patients’ wounds had necrosis. As per our Cobra BITE score, the three factors predicting secondary wound infection after cobra bites are hospital admission, a white blood cell count (in 103/µL) × by neu-trophil-lymphocyte ratio value of ≥114.23, and the use of antivenin medication. -

Snake Venomics of Monocled Cobra (Naja Kaouthia) and Investigation of Human Igg Response Against Venom Toxins
Downloaded from orbit.dtu.dk on: May 08, 2019 Snake venomics of monocled cobra (Naja kaouthia) and investigation of human IgG response against venom toxins Laustsen, Andreas Hougaard; Gutiérrez, José María; Lohse, Brian; Rasmussen, Arne R.; Fernández, Julián; Milbo, Christina; Lomonte, Bruno Published in: Toxicon Link to article, DOI: 10.1016/j.toxicon.2015.03.001 Publication date: 2015 Document Version Peer reviewed version Link back to DTU Orbit Citation (APA): Laustsen, A. H., Gutiérrez, J. M., Lohse, B., Rasmussen, A. R., Fernández, J., Milbo, C., & Lomonte, B. (2015). Snake venomics of monocled cobra (Naja kaouthia) and investigation of human IgG response against venom toxins. Toxicon, 99, 23-35. https://doi.org/10.1016/j.toxicon.2015.03.001 General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. Users may download and print one copy of any publication from the public portal for the purpose of private study or research. You may not further distribute the material or use it for any profit-making activity or commercial gain You may freely distribute the URL identifying the publication in the public portal If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. *Manuscript Click here to view linked References 1 2 Snake venomics of monocled cobra (Naja kaouthia) and 3 investigation of human IgG response against venom toxins 4 5 Andreas H. -
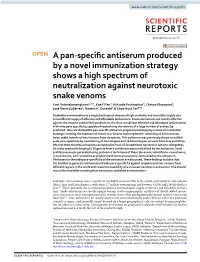
A Pan-Specific Antiserum Produced by a Novel Immunization Strategy
www.nature.com/scientificreports OPEN A pan-specifc antiserum produced by a novel immunization strategy shows a high spectrum of neutralization against neurotoxic snake venoms Kavi Ratanabanangkoon1,2 ✉ , Kae Yi Tan3, Kritsada Pruksaphon4, Chaiya Klinpayom5, José María Gutiérrez6, Naeem H. Quraishi7 & Choo Hock Tan8 ✉ Snakebite envenomation is a neglected tropical disease of high mortality and morbidity largely due to insufcient supply of efective and afordable antivenoms. Snake antivenoms are mostly efective against the venoms used in their production. It is thus crucial that efective and afordable antivenom(s) with wide para-specifcity, capable of neutralizing the venoms of a large number of snakes, be produced. Here we studied the pan-specifc antiserum prepared previously by a novel immunization strategy involving the exposure of horses to a ‘diverse toxin repertoire’ consisting of 12 neurotoxic Asian snake toxin fractions/ venoms from six species. This antiserum was previously shown to exhibit wide para-specifcity by neutralizing 11 homologous and 16 heterologous venoms from Asia and Africa. We now show that the antiserum can neutralize 9 out of 10 additional neurotoxic venoms. Altogether, 36 snake venoms belonging to 10 genera from 4 continents were neutralized by the antiserum. Toxin profles previously generated using proteomic techniques of these 36 venoms identifed α-neurotoxins, β-neurotoxins, and cytotoxins as predominant toxins presumably neutralized by the antiserum. The bases for the wide para-specifcity of the antiserum are discussed. These fndings indicate that it is feasible to generate antivenoms of wide para-specifcity against elapid neurotoxic venoms from diferent regions in the world and raises the possibility of a universal neurotoxic antivenom. -

Research Journal of Pharmaceutical, Biological and Chemical
ISSN: 0975-8585 Research Journal of Pharmaceutical, Biological and Chemical Sciences Diversity of Squamates (Scaled Reptiles) in Selected Urban Areas of Cagayan de Oro City, Misamis Oriental. John C Naelga*, Daniel Robert P Tayag, Hazel L Yañez, and Astrid L Sinco. Xavier University – Ateneo De Cagayan, Kinaadman Resource Center. ABSTRACT This study was conducted to provide baseline information on the local urban diversity of squamates in the selected areas of Barangay Kauswagan, Barangay Balulang, and Barangay FS Catanico in Cagayan de Oro City. These urban sites are close to the river and are likely to be inhabited by reptiles. Each site had at least ten (10) points and was sampled no less than five (5) times in the months of September to November 2016 using homemade traps and the Cruising-Transect walk method. One representative per species was preserved. A total of two hundred sixty-seven (267) individuals, grouped into four (4) families and ten (10) species were found in the sampling areas. Six (6) snake species were identified, namely: Boiga cynodon, Naja samarensis, Chrysopelea paradisi, Gonyosoma oxycephalum, Coelegnathus erythrurus eryhtrurus, and Dendrelaphis pictus; while four (4) species were lizards namely: Gekko gecko, Hemidactylus platyurus, Lamprolepis smaragdina philippinica, and Eutropis multifasciata.In Barangay Kauswagan, Hemidactylus platyurus was the most abundant (RA= 52.94%). In Barangay Balulang, the most abundant species was Hemidactylus platyurus (RA= 43.82%). In Barangay FS Catanico, the most abundant was Hemidactylus platyurus (RA= 40.16%). The area with the highest species diversity was Barangay FS Catanico (H= 1.36), followed by Barangay Balulang (H= 1.28), and Barangay Kauswagan (H= 1.08). -

First Record of the Southern Philippine Cobra Naja Samarensis on Siquijor Island, Philippines
SEAVR 2020: 036‐037 ISSN: 2424‐8525 Date of publication: 29 October 2020 Hosted online by ecologyasia.com First record of the Southern Philippine Cobra Naja samarensis on Siquijor Island, Philippines Emerson Y. SY & Abner A. BUCOL [email protected] (Sy) Observer: Frank Wronsky. Photograph by: Frank Wronsky. Subject identified by: Emerson Y. Sy. Location: Siquijor Island, Barangay Tambisan, Municipality of San Juan, Siquijor Province, Philippines. Elevation: 10 metres ASL. Habitat: Near the coast and adjacent to farmland. Date and time: 31 July 2015, 14:50 hrs. Identity of subject: Southern Philippine Cobra, Naja samarensis (Reptilia: Squamata: Serpentes: Elapidae). Description of record: A snake, approximately 60 cm in total length, was observed struggling to escape from entanglement in discarded nylon fishing net on the ground (Fig. 1). Fig. 1. © Frank Wronsky Remarks: The snake, locally known as Ugahipon in Cebuano language, and also known as Peters’ Cobra or Samar Cobra, was identified as Naja samarensis based on (i) loreal scale is absent, (ii) one preocular, (iii) three postoculars, (iv) seven upper labials, 3rd and 4th in contact with eye, (v) neck colour is yellow, (vi) dorsal body colour is dark grey, and (iv) skin between dorsal scales is yellow (Taylor, 1922). This endemic species is known to occur in Mindanao faunal region on the following islands: 36 Basilan, Bohol, Camiguin Sur, Dinagat, Leyte, Mindanao, and Samar (Sy and Mangkabong, 2018). A more recent observation of the species on Siquijor was in Barangay Cangasagan, Municipality of San Juan (O. Lalim, pers. comm. to EYS on 4 May 2020). Siquijor is surrounded by four major islands belonging to two faunal regions – Negros and Cebu (Western Visayas faunal region) and Bohol and Mindanao (Mindanao faunal region). -
Endangered Species (Import and Export) Act (Chapter 92A)
1 S 23/2005 First published in the Government Gazette, Electronic Edition, on 11th January 2005 at 5:00 pm. NO.S 23 ENDANGERED SPECIES (IMPORT AND EXPORT) ACT (CHAPTER 92A) ENDANGERED SPECIES (IMPORT AND EXPORT) ACT (AMENDMENT OF FIRST, SECOND AND THIRD SCHEDULES) NOTIFICATION 2005 In exercise of the powers conferred by section 23 of the Endangered Species (Import and Export) Act, the Minister for National Development hereby makes the following Notification: Citation and commencement 1. This Notification may be cited as the Endangered Species (Import and Export) Act (Amendment of First, Second and Third Schedules) Notification 2005 and shall come into operation on 12th January 2005. Deletion and substitution of First, Second and Third Schedules 2. The First, Second and Third Schedules to the Endangered Species (Import and Export) Act are deleted and the following Schedules substituted therefor: ‘‘FIRST SCHEDULE S 23/2005 Section 2 (1) SCHEDULED ANIMALS PART I SPECIES LISTED IN APPENDIX I AND II OF CITES In this Schedule, species of an order, family, sub-family or genus means all the species of that order, family, sub-family or genus. First column Second column Third column Common name for information only CHORDATA MAMMALIA MONOTREMATA 2 Tachyglossidae Zaglossus spp. New Guinea Long-nosed Spiny Anteaters DASYUROMORPHIA Dasyuridae Sminthopsis longicaudata Long-tailed Dunnart or Long-tailed Sminthopsis Sminthopsis psammophila Sandhill Dunnart or Sandhill Sminthopsis Thylacinidae Thylacinus cynocephalus Thylacine or Tasmanian Wolf PERAMELEMORPHIA -

Types of Snakes in the Philippines
Types of Snakes in the Philippines The tropical climate of the Philippines makes it an ideal habitat for many types of snake. The tropical climate of the Philippines makes it an ideal habitat for many types of snake. The ecosystems found throughout the archipelago are prime habitat for a large number of snake species. While most of the snake species found there are harmless, the Philippines is also home to some of the deadliest snakes in the world. Venomous snakes in the Philippines fall into four categories. John Foxx/Stockbyte/Getty Images Cobras Easily identified by the intimidating hoods that extend on both sides of their heads, various cobra species inhabit the Philippines. The king cobra, the world's largest venomous snake, reaching a maximum length of 16 feet here. Three species of spitting cobras are native to the Philippines: the Northern Philippine cobra, the Southeastern Philippine cobra and the equatorial spitting cobra. In addition to inflicting deadly bites, these cobras have the ability to spit a blinding stream of venom at a target nearly 10 feet away. Pit Vipers These brightly colored snakes dwell in trees throughout the Philippines. Wagler’s, Philippine, Polillo, and Bataan are all different species of lance-headed pit vipers that inhabit the archipelago. A unique feature of lance-headed pit vipers is that they give live birth to their young instead of laying eggs. Pit viper venom attacks red blood cells instead of the nervous system like other snake venom. Coral Snakes Several species of coral snakes are found in the Philippines, including the Palawan long-glanded coral snake and the Luzon coral snake. -

Snake Venomics of Monocled Cobra (Naja Kaouthia) and Investigation of Human Igg Response Against Venom Toxins
Downloaded from orbit.dtu.dk on: Sep 27, 2021 Snake venomics of monocled cobra (Naja kaouthia) and investigation of human IgG response against venom toxins Laustsen, Andreas Hougaard; Gutiérrez, José María; Lohse, Brian; Rasmussen, Arne R.; Fernández, Julián; Milbo, Christina; Lomonte, Bruno Published in: Toxicon Link to article, DOI: 10.1016/j.toxicon.2015.03.001 Publication date: 2015 Document Version Peer reviewed version Link back to DTU Orbit Citation (APA): Laustsen, A. H., Gutiérrez, J. M., Lohse, B., Rasmussen, A. R., Fernández, J., Milbo, C., & Lomonte, B. (2015). Snake venomics of monocled cobra (Naja kaouthia) and investigation of human IgG response against venom toxins. Toxicon, 99, 23-35. https://doi.org/10.1016/j.toxicon.2015.03.001 General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. Users may download and print one copy of any publication from the public portal for the purpose of private study or research. You may not further distribute the material or use it for any profit-making activity or commercial gain You may freely distribute the URL identifying the publication in the public portal If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. *Manuscript Click here to view linked References 1 2 Snake venomics of monocled cobra (Naja kaouthia) and 3 investigation of human IgG response against venom toxins 4 5 Andreas H. -

How the Cobra Got Its Flesh-Eating Venom: Cytotoxicity As a Defensive Innovation and Its Co-Evolution with Hooding, Aposematic Marking, and Spitting
toxins Article How the Cobra Got Its Flesh-Eating Venom: Cytotoxicity as a Defensive Innovation and Its Co-Evolution with Hooding, Aposematic Marking, and Spitting Nadya Panagides 1,†, Timothy N.W. Jackson 1,†, Maria P. Ikonomopoulou 2,3,†, Kevin Arbuckle 4,†, Rudolf Pretzler 1,†, Daryl C. Yang 5,†, Syed A. Ali 1,6, Ivan Koludarov 1, James Dobson 1, Brittany Sanker 1, Angelique Asselin 1, Renan C. Santana 1, Iwan Hendrikx 1, Harold van der Ploeg 7, Jeremie Tai-A-Pin 8, Romilly van den Bergh 9, Harald M.I. Kerkkamp 10, Freek J. Vonk 9, Arno Naude 11, Morné A. Strydom 12,13, Louis Jacobsz 14, Nathan Dunstan 15, Marc Jaeger 16, Wayne C. Hodgson 5, John Miles 2,3,17,‡ and Bryan G. Fry 1,*,‡ 1 Venom Evolution Lab, School of Biological Sciences, University of Queensland, St. Lucia, QLD 4072, Australia; [email protected] (N.P.); [email protected] (T.N.W.J.); [email protected] (R.P.); [email protected] (S.A.A.); [email protected] (I.K.); [email protected] (J.D.); [email protected] (B.S.); [email protected] (A.A.); [email protected] (R.C.S.); [email protected] (I.H.) 2 QIMR Berghofer Institute of Medical Research, Herston, QLD 4049, Australia; [email protected] (M.P.I.); [email protected] (J.M.) 3 School of Medicine, The University of Queensland, Herston, QLD 4002, Australia 4 Department of Biosciences, College of Science, Swansea University, Swansea SA2 8PP, UK; [email protected] 5 Monash Venom Group, Department of Pharmacology, Monash University, -

2017 Jones B Msc
Bangor University MASTERS BY RESEARCH The Evolution of Defensive Strategies in Cobras Jones, Bryony Award date: 2017 Awarding institution: Bangor University Link to publication General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal ? Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Download date: 28. Sep. 2021 The Evolution of Defensive Strategies in Cobras Bryony Jones Supervisor: Dr Wolfgang Wüster Thesis submitted for the degree of Masters of Science by Research Biological Sciences The Evolution of Defensive Strategies in Cobras Abstract Species use multiple defensive strategies aimed at different sensory systems depending on the level of threat, type of predator and options for escape. The core cobra clade is a group of highly venomous Elapids that share defensive characteristics, containing true cobras of the genus Naja and related genera Aspidelaps, Hemachatus, Walterinnesia and Pseudohaje. Species combine the use of three visual and chemical strategies to prevent predation from a distance: spitting venom, hooding and aposematic patterns.