Eye Disease Enc-Eye-Clopedia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

12 Retina Gabriele K
299 12 Retina Gabriele K. Lang and Gerhard K. Lang 12.1 Basic Knowledge The retina is the innermost of three successive layers of the globe. It comprises two parts: ❖ A photoreceptive part (pars optica retinae), comprising the first nine of the 10 layers listed below. ❖ A nonreceptive part (pars caeca retinae) forming the epithelium of the cil- iary body and iris. The pars optica retinae merges with the pars ceca retinae at the ora serrata. Embryology: The retina develops from a diverticulum of the forebrain (proen- cephalon). Optic vesicles develop which then invaginate to form a double- walled bowl, the optic cup. The outer wall becomes the pigment epithelium, and the inner wall later differentiates into the nine layers of the retina. The retina remains linked to the forebrain throughout life through a structure known as the retinohypothalamic tract. Thickness of the retina (Fig. 12.1) Layers of the retina: Moving inward along the path of incident light, the individual layers of the retina are as follows (Fig. 12.2): 1. Inner limiting membrane (glial cell fibers separating the retina from the vitreous body). 2. Layer of optic nerve fibers (axons of the third neuron). 3. Layer of ganglion cells (cell nuclei of the multipolar ganglion cells of the third neuron; “data acquisition system”). 4. Inner plexiform layer (synapses between the axons of the second neuron and dendrites of the third neuron). 5. Inner nuclear layer (cell nuclei of the bipolar nerve cells of the second neuron, horizontal cells, and amacrine cells). 6. Outer plexiform layer (synapses between the axons of the first neuron and dendrites of the second neuron). -

Onchocerciasis
11 ONCHOCERCIASIS ADRIAN HOPKINS AND BOAKYE A. BOATIN 11.1 INTRODUCTION the infection is actually much reduced and elimination of transmission in some areas has been achieved. Differences Onchocerciasis (or river blindness) is a parasitic disease in the vectors in different regions of Africa, and differences in cause by the filarial worm, Onchocerca volvulus. Man is the the parasite between its savannah and forest forms led to only known animal reservoir. The vector is a small black fly different presentations of the disease in different areas. of the Simulium species. The black fly breeds in well- It is probable that the disease in the Americas was brought oxygenated water and is therefore mostly associated with across from Africa by infected people during the slave trade rivers where there is fast-flowing water, broken up by catar- and found different Simulium flies, but ones still able to acts or vegetation. All populations are exposed if they live transmit the disease (3). Around 500,000 people were at risk near the breeding sites and the clinical signs of the disease in the Americas in 13 different foci, although the disease has are related to the amount of exposure and the length of time recently been eliminated from some of these foci, and there is the population is exposed. In areas of high prevalence first an ambitious target of eliminating the transmission of the signs are in the skin, with chronic itching leading to infection disease in the Americas by 2012. and chronic skin changes. Blindness begins slowly with Host factors may also play a major role in the severe skin increasingly impaired vision often leading to total loss of form of the disease called Sowda, which is found mostly in vision in young adults, in their early thirties, when they northern Sudan and in Yemen. -

JMSCR Vol||08||Issue||02||Page 208-210||February 2020
JMSCR Vol||08||Issue||02||Page 208-210||February 2020 http://jmscr.igmpublication.org/home/ ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v8i2.40 Keratomalacia - A Case Report Authors Deepthi Pullepu1*, Deepthi Janga2, V Murali Krishna3 *Corresponding Author Deepthi Pullepu Department of Ophthalmology, Rangaraya Medical College, Kakinada, Andhra Pradesh, India Abstract Xerophthalmia refers to an ocular condition of destructive dryness of conjunctiva and cornea caused due to severe vitamin A deficiency. Usually affects infants, children and women of reproductive age group. It is estimated to affect about one-third of children under the age of five around the world. Keratomalacia means dry and cloudy cornea which melts and perforates, caused due to severe vitamin A deficiency. Here we describe a case of 21 year old female with neurofibromatosis type 1 presenting with keratomalacia. Keywords: Vitamin A deficiency, Xerophthalmia, Keratomalacia. Introduction blindness is a significant contributor Vitamin A is essential for the functioning of the In India, it is estimated that there are immune system, healthy growth and development approximately 6.8 million people who have vision of body and is usually acquired through diet. less than 6/60 in at least one eye due to corneal Globally, 190 million children under five years of diseases; of these, about a million have bilateral age are affected by vitamin A deficiency involvement. They suffer from an increased risk of visual Corneal blindness resulting due to this disease can impairment, illness and death from childhood be completely prevented by institution of effective infections such as measles and those causing preventive or prophylactic measures at the diarrhoea community level. -
Approach to the Patient with Presumed Cellulitis Daniela Kroshinsky, MD,* Marc E
Approach to the Patient With Presumed Cellulitis Daniela Kroshinsky, MD,* Marc E. Grossman, MD, FACP,† and Lindy P. Fox, MD‡ Dermatologists frequently are consulted in the evaluation and management of the patient with cellulitic-appearing skin. For routine cellulitis, the clinical presentation and patient symptoms are usually sufficient for an accurate diagnosis. However, when the clinical presentation is somewhat atypical, or if the patient fails to respond to appropriate therapy for cellulitis because of routine bacterial pathogens, the differential diagnosis should be rapidly expanded. We discuss the approach to the patient with presumed cellulitis, with an emphasis on the differential diagnosis of cellulitis in both the immunocompetent and immunucompromised patient. Semin Cutan Med Surg 26:168-178 © 2007 Elsevier Inc. All rights reserved. KEYWORDS cellulitis, erysipelas 53-year-old woman with a history of recurrent breast of cellulitis, and telangiectasia and scattered enlarged mes- Acancer diagnosed 2 years before presentation and treated enchymal cells, characteristic of radiation changes. with radiation and chemotherapy (docetaxel, anastrozole, exemestane, gemcitabine) most recently 6 months before presentation was admitted for 3 weeks of worsening chest Clinical Problem wall pain and a rash over her mastectomy scar. Despite 5 days Dermatologists frequently are consulted in the evaluation of empiric antibiotic therapy with doxycycline and vancomy- and management of the patient with cellulitic-appearing cin, the chest wall erythema and pain were increasing. A dermatology consultation was called. An ulceration and sur- skin. Although the dermatologist may be consulted early on rounding erythematous papules were concentrated over the in the patient’s course, more often a dermatology consult is mastectomy scar with ill-defined erythematous patches that requested when a patient fails to respond to treatment. -

Abstract: a 19 Year Old Male Was Diagnosed with Vitamin a Deficiency
Robert Adam Young Abstract: A 19 year old male was diagnosed with vitamin A deficiency (VAD). Clinical examination shows conjunctival changes with central and marginal corneal ulcers. Patient history and lab testing were used to confirm the diagnosis. I. Case History 19 year old Hispanic Male Presents with chief complaint of progressive blur at distance and near in both eyes, foreign body sensation, ocular pain, photophobia, and epiphora; signs/symptoms are worse in the morning upon wakening. Started 6 months to 1 year ago, and has progressively gotten worse. Patient reports that the right eye is worse than the left eye. Ocular history of Ocular Rosacea Medical history of Hypoaldosteronism, Pernicious Anemia, and Type 2 Polyglandular Autoimmune Syndrome Last eye examination was two weeks ago at a medical center Presenting topical/systemic medications - Tobramycin TID OU, Prednisolone Acetate QD OU (has used for two weeks); Fludrocortisone (used long-term per PCP) Other pertinent info includes reports that patient cannot gain weight, although he has a regular appetite. Patient presents looking very slim, malnourished, and undersized for his age. II. Pertinent findings Entering unaided acuities are 20/400 OD with no improvement with pinhole; 20/50 OS that improves to 20/25 with pinhole. Pupil testing shows (-)APD; Pupils are 6mm in dim light, and constrict to 4mm in bright light. Ocular motilities are full and smooth with no reports of diplopia or pain. Tonometry was performed with tonopen and revealed intraocular pressures of 12 mmHg OD and 11 mmHG OS. Slit lamp examination shows 2+ conjunctival injection with trace-mild bitot spots both nasal and temporal, OU. -

Onchocerciasis: a Potential Risk Factor for Glaucoma P R Egbert, D W Jacobson, S Fiadoyor, P Dadzie, K D Ellingson
796 WORLD VIEW Br J Ophthalmol: first published as 10.1136/bjo.2004.061895 on 17 June 2005. Downloaded from Onchocerciasis: a potential risk factor for glaucoma P R Egbert, D W Jacobson, S Fiadoyor, P Dadzie, K D Ellingson ............................................................................................................................... Br J Ophthalmol 2005;89:796–798. doi: 10.1136/bjo.2004.061895 Series editors: W V Good and S Ruit Background: Onchocerciasis is a microfilarial disease that causes ocular disease and blindness. Previous See end of article for evidence of an association between onchocerciasis and glaucoma has been mixed. This study aims to authors’ affiliations ....................... further investigate the association between onchocerciasis and glaucoma. Methods: All subjects were patients at the Bishop John Ackon Christian Eye Centre in Ghana, west Africa, Correspondence to: undergoing either trabeculectomy for advanced glaucoma or extracapsular extraction for cataracts, who Peter Egbert, MD, Department of also had a skin snip biopsy for onchocerciasis. A cross sectional case-control study was performed to Ophthalmology, Stanford assess the difference in onchocerciasis prevalence between the two study groups. University School of Results: The prevalence of onchocerciasis was 10.6% in those with glaucoma compared with 2.6% in those Medicine, Stanford Eye with cataracts (OR, 4.45 (95% CI 1.48 to 13.43)). The mean age in the glaucoma group was significantly Center, 900 Blake Wilbur Drive, RoomW3002, younger than in the cataract group (59 and 65, respectively). The groups were not significantly different Stanford, CA 94305, USA; with respect to sex or region of residence. In models adjusted for age, region, and sex, subjects with [email protected] glaucoma had over three times the odds of testing positive for onchocerciasis (OR, 3.50 (95% CI 1.10 to Accepted for publication 11.18)). -

Current Health Issues in the Caribbean BLINDNESS in THE
Current Health Issues in the Caribbean BLINDNESS IN THE CARIBBEAN Alfred L. Anduze, M.D. St. Croix Vision Center St. Croix Hospital St. Croix U.S. Virgin Islands Caribbean Studies Association Merida, Mexico May 26, 1994 Abstract: Blindness in the Caribbean Background: The prevailing of blindness in the Caribbean region are reviewed in the context of world blindness statistics to identify differences and similarities that might exist. Method: A review of the status of blindness in the U.S. Virgin Islands, Barbados, Jamaica, Puerto Rico, Trinidad, and Mexico; individually with regard to causal etiology, epidemiology, treatment and possible future research. Results: Blindness in the Caribbean is the result of genetics, tropical environment and cultural habits of the inhabitants and consist of Age-related macular disease, Infectious diseases, Diabetes mellitus, Glaucoma, Congenital defects, Xerophthalmia, Trachoma, Trauma and Cataracts. Conclusion: There are almost 50 million people who are legally blind worldwide (i.e. with a vision of 20/200 or less) 2-3 million in the Caribbean region. The social and economic consequences are serious additional deterrents in developing countries. Outline: Causes of Blindness in the Caribbean I. Age-related macular disease a. Vascular insufficiency b. Senile macular degeneration II. Cataracts III. Glaucoma IV. Diabetes mellitus V. Infectious diseases a. Trachoma b. Onchocerciasis c. Leprosy d. Toxoplasmosis e. Toxocariasis f. AIDS VI. Trauma a. industrial/work-related b. sports c. home accidents VII. Nutritional a. Xerophthalmia/keratomalacia b. Iron-deficiency anemia c. Tobacco/Alcohol Retinopathy VIII. Congenital defects a. genetic syndromes b. strabismus Legal blindness is acceptably defined as vision 20/200 (6/60) or less. -
2002 Samel 10 Most Common Systemic Health Conditions with A
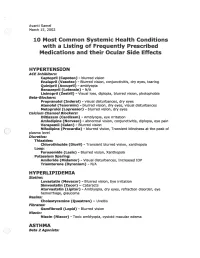
Avanti Samel / March 15, 2002 10 Most Common Systemic Health Conditions with a Listing of Frequently Prescribed Medications and their Ocular Side Effects HYPERTENSION ACE Inhibitors: Captopril (Capoten}- blurred vision Enalapril (Vasotec) - Blurred vision, conjunctivitis, dry eyes, tearing Quinipril (Accupril)- amblyopia Benazepril (Lotensin)- N/A Lisinopril (Zestril) - Visual loss, diplopia, blurred vision, photophobia Beta-Blockers: Propranolol (Inderal)- visual disturbances, dry eyes Atenolol (Tenormin)- blurred vision, dry eyes, visual disturbances Metoprolol (Lopressor) - blurred vision, dry eyes calcium Channel Blockers: Diltiazem (Cardizem)- Amblyopia, eye irritation Amlodipine (Norvasc)- abnormal vision, conjunctivitis, diplopia, eye pain Verapamil (Calan)- Blurred vision Nifedipine (Procardia) - blurred vision, Transient blindness at the peak of plasma level · Diuretics: Thiazides: Chlorothiazide (Diuril) - Transient blurred vision, xanthopsia Loop: Furosemide (Lasix) - Blurred vision, Xanthopsia Potassium Sparing: Amiloride (Midamor) - Visual disturbances, Increased lOP Triamterene (Dyrenium)- N/A HYPERLIPIDEMIA Statins: Lovastatin (Mevacor) - Blurred vision, Eye irritation Simvastatin (Zocor)- Cataracts Atorvastatin (Lipitor)- Amblyopia, dry eyes, refraction disorder, eye hemorrhage, glaucoma Resins: Cholestyramine (Questran)- Uveitis Fibrates: Gemfibrozil (Lopid)- Blurred vision Niacin: Niacin (Niacor) - Toxic amblyopia, cystoid macular edema ASTHMA ( ) Beta 2 Agonists: Albuterol (Proventil) - N/A ( Salmeterol (Serevent)- -

© Alan Macfarlane and Gerry Martin, 2002 1 MYOPIA: ITS
© Alan Macfarlane and Gerry Martin, 2002 MYOPIA: ITS COMPARATIVE INCIDENCE AND PROBABLE CAUSES What Rasmussen encountered in his many years of working with Chinese eye problem astonished him. He summarized his impressions thus. 'Three facts stand out clearly in both ancient and modern records of Chinese eyesight: one that they are a highly myopic nation; two that keratomalacia is the major cause of ocular disease; and three that presbyopia is earlier than in the West by about five years. They stand out against an historical background of neglect and abuse, malnutrition, and centuries of State indifference.' (p.48) Moving on to the statistics of myopia, he summarized the research of a quarter of a century by saying that 'only 20 per cent. of all lenses supplied by the ancients, and similar amount by the moderns (excluding high astigmatic) were for old-sight lenses. It is the other 80 per cent. that matters; the 65 per cent. for myopia and the 15 per cent. for glare and therapeutics.' (p.20) Elsewhere he gives slightly different statistics, which applied to those aged under forty years, showed that approximately 75 per cent. of the lenses were supplied for myopia. In a detailed table he presents the figures; in the 'Ancient Chinese Sight Records', 65% were for myopia; in the 'Modern Chinese Sight Records' myopia (simple) or with astigmatism combined accounted for 70% of the lenses.(p.48) The second figure of 70% was based on 120,000 case histories collected by Rasmussen and his colleagues over a period of 25 years. (p.49) The significance of the degree of myopia only comes out if we compare the Chinese figures with those for other nationalities. -

The Main Causes of Blindness and Low Vision in School for Blind
26ORIGINAL ARTICLE DOI 10.5935/0034-7280.20160006 The main causes of blindness and low vision in school for blind As principais causas de cegueira e baixa visão em escola para deficientes visuais Abelardo Couto Junior1, Lucas Azeredo Gonçalves de Oliveira2 ABSTRACT Objective: Identify and analyze the main causes of blindness and low vision in school for blind. Methods: One hundred sixty-five medical records of visually impaired students were reviewed in an institution specialized in teaching the blind, treated between august 2013 and may 2014. The variables analyzed were age, sex, visual acuity, primary and secondary diagnoses, treatment, optical prescription features and prognosis. Results: 165 students were evaluated, 91 students (55%) are legally blind and only 74 (45%) of the students are classified as low vision. The main causes of blindness were: retinopathy of prematurity (21%), optic nerve atrophy (18%), congenital glaucoma (16%), retinal dystrophy (11%) and cancer (8%). The causes of low vision were: congenital cataract (18%), congenital glaucoma (15%) and retinochoroidal scarring (12%). Conclusion: The main causes of blindness and low vision in the Benjamin Constant Institute are from preventable diseases. Keywords: Blindness; Low vision; Visual acuity; Child; Health school RESUMO Objetivo: Identificar e analisar as principais causas de cegueira e baixa visão em escola para deficientes visuais. Métodos: Foram revisados 165 prontuários de alunos portadores de deficiência visual em instituição especializada no ensino de cegos, atendidos no período de agosto de 2013 a maio de 2014. As variáveis analisadas foram: idade, gênero, acuidade visual, diagnóstico principal e secundário, tratamento, recursos ópticos prescritos e prognóstico. Resultados: Dos 165 alunos avaliados, 91 alunos (55%) são legalmente cegos e apenas 74 (45%) dos alunos são enquadrados como baixa visão. -

Assessment of Bacterial Profile of Ocular Infections Among Subjects Undergoing Ivermectin Therapy in Onchocerciasis Endemic Area in Nigeria
Ophthalmology Research: An International Journal 9(4): 1-9, 2018; Article no.OR.46610 ISSN: 2321-7227 Assessment of Bacterial Profile of Ocular Infections among Subjects Undergoing Ivermectin Therapy in Onchocerciasis Endemic Area in Nigeria Okeke-Nwolisa, Benedictta Chinweoke1*, Enweani, Ifeoma Bessie1, Oshim, Ifeanyi Onyema1, Urama, Evelyn Ukamaka1, Olise, Augustina Nkechi2, Odeyemi, Oluwayemisi3 and Uzozie, Chukwudi Charles4 1Department of Medical Laboratory Science, Faculty of Health Sciences and Technology, College of Health Sciences, Nnamdi Azikiwe University, Anambra State, Nigeria. 2Department of Medical Laboratory Science, School of Basic Medical Science, University of Benin, Benin-City, Nigeria. 3Department of Medical Microbiology, Nnamdi Azikiwe University Teaching Hospital, Anambra State, Nigeria. 4Department of Ophthalmology (Guinness Eye Centre, Onitsha), NAUTH, Nnewi, Nigeria. Authors’ contributions Author ONBC performed the sample collection, processing and data analyses. Author EIB conceived and supervised the research work. Author OIO participated in literature review, manuscript writing and editing. Author UCC was involved in training of the researcher on the collection of conjunctival swab samples. Authors UEU, OO and OAN were also involved in editing and reviewing of the manuscript. Article Information DOI: 10.9734/OR/2018/v9i430094 Editor(s): (1) Dr. Kota V Ramana, Professor, Department of Biochemistry & Molecular Biology, University of Texas Medical Branch, USA. Reviewers: (1) Dr. Augustine U. Akujobi, Imo State University Owerri, Nigeria. (2) Engy M. Mostafa, Sohag University, Egypt. (3) Asaad Ahmed Ghanem, Mansoura University, Egypt. Complete Peer review History: http://www.sdiarticle3.com/review-history/46610 Received 12 November 2018 Original Research Article Accepted 30 January 2019 Published 23 February 2019 ABSTRACT Bacteria are the major contributor of ocular infections worldwide. -

Infectious Organisms of Ophthalmic Importance
INFECTIOUS ORGANISMS OF OPHTHALMIC IMPORTANCE Diane VH Hendrix, DVM, DACVO University of Tennessee, College of Veterinary Medicine, Knoxville, TN 37996 OCULAR BACTERIOLOGY Bacteria are prokaryotic organisms consisting of a cell membrane, cytoplasm, RNA, DNA, often a cell wall, and sometimes specialized surface structures such as capsules or pili. Bacteria lack a nuclear membrane and mitotic apparatus. The DNA of most bacteria is organized into a single circular chromosome. Additionally, the bacterial cytoplasm may contain smaller molecules of DNA– plasmids –that carry information for drug resistance or code for toxins that can affect host cellular functions. Some physical characteristics of bacteria are variable. Mycoplasma lack a rigid cell wall, and some agents such as Borrelia and Leptospira have flexible, thin walls. Pili are short, hair-like extensions at the cell membrane of some bacteria that mediate adhesion to specific surfaces. While fimbriae or pili aid in initial colonization of the host, they may also increase susceptibility of bacteria to phagocytosis. Bacteria reproduce by asexual binary fission. The bacterial growth cycle in a rate-limiting, closed environment or culture typically consists of four phases: lag phase, logarithmic growth phase, stationary growth phase, and decline phase. Iron is essential; its availability affects bacterial growth and can influence the nature of a bacterial infection. The fact that the eye is iron-deficient may aid in its resistance to bacteria. Bacteria that are considered to be nonpathogenic or weakly pathogenic can cause infection in compromised hosts or present as co-infections. Some examples of opportunistic bacteria include Staphylococcus epidermidis, Bacillus spp., Corynebacterium spp., Escherichia coli, Klebsiella spp., Enterobacter spp., Serratia spp., and Pseudomonas spp.