Review of Progress Against Healthcare Standards for Wales
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ablett Unit and Car Park Development Planning Statement
Glan Clywd Hospital: Ablett Unit and Car Park Development Planning Statement Prepared by WYG on behalf of The Betsi Cadwaladr University Health Board and BAM Construction August 2020 Quay West at MediaCityUK, Trafford Wharf Road, Trafford Park, Manchester, M17 1HH Tel: +44 (0)161 872 3223 Fax: +44 (0)161 872 3193 Email: Website: www. wyg .com WYG Environment Planning Transport Limited. Registered in England & Wales Number: 03050297 Registered Office: 3 Sovereign Square, Sovereign Street, Leeds, West Yorkshire, LS1 4ER Document control Document: Planning Statement Project: Glan Clwyd Hospital – Ablett Unit Prepared By: Peter Campbell Reviewed By: Peter Shannon Client: Betsi Cadwaladr University Health Board and BAM Construction Job Number: A114096 Issue: V2.1 – Planning Consultation Draft Version – 18.08.2020 www.wyg.com creative minds safe hands Contents 1 INTRODUCTION ........................................................................................................... 1 1.1 SCOPE AND PURPOSE ................................................................................................................ 1 1.2 DEVELOPMENT PROPOSALS ......................................................................................................... 1 1.3 APPLICATION DOCUMENTS ......................................................................................................... 1 1.4 STRUCTURE OF REPORT ............................................................................................................. 2 2 BACKGROUND ............................................................................................................. -

Paper 1: Betsi Cadwaladr University Health Board
Pwyllgor Iechyd, Gofal Cymdeithasol a Chwaraeon Health, Social Care and Sport Committee HSCS(5)-26-19 Papur 1 / Paper 1 Betsi Cadwaladr University Health Board submission to the Health, Social Care and Sport Committee’s general scrutiny inquiry. Contact: Gary Doherty, Chief Executive Date: 6th September, 2019 Introduction 1. Betsi Cadwaladr welcomes this opportunity to contribute to the Health, Social Care and Sport Committee’s general scrutiny inquiry. About the organisation 2. The Health Board is responsible for improving the health and well-being of the population of around 678,000 across the six counties of North Wales (Anglesey, Gwynedd, Conwy, Denbighshire, Flintshire and Wrexham). It is also responsible for the provision of primary, community and mental health as well as acute hospital services. It operates three main hospitals (Ysbyty Gwynedd in Bangor, Glan Clwyd Hospital in Bodelwyddan and Wrexham Maelor Hospital) along with a network of community hospitals, health centres, clinics, mental health units and community team bases. The Health Board commissions the work of 105 GP practices, and NHS services provided by dentists, opticians and pharmacists as well as ensuring the population of North Wales can access high quality specialised services provided by NHS Trusts in England. In 2018/19, the Health Board had a revenue income of £1.54 billion and we employ approximately 18,000 people (15,500 whole time equivalents). Overview 3. The past year has been another very challenging period for the Health Board. Although progress has been made in moving the organisation forwards, much more needs to be done, across a number of fronts, to return the Health Board to a secure footing for the future. -

NORTH WALES MEDICINES RESEARCH SYMPOSIUM Symposiwm Ymchwil Meddyginiaethau Gogledd Cymru
NORTH WALES MEDICINES RESEARCH SYMPOSIUM Symposiwm Ymchwil Meddyginiaethau Gogledd Cymru 1st July 2015 Faenol Fawr Hotel, Bodelwyddan Programme 6.00 Buffet & Poster viewing 6.40 Welcome Professor Dyfrig Hughes, Bangor University 6.45 Keynote presentation: “Medicines non- Professor Andrew Farmer, University adherence: managing a complex problem” of Oxford 7.30 Magnetic nanoparticle-directed enzyme therapy Dr Jenny Halliwell, Bangor University 7.50 Using medication-related acute kidney injury Janet Thomas, Betsi Cadwaladr admissions to build a preventative cross-sector University Health Board risk reduction response 8.10 The role of nationally agreed Prescribing Professor Philip Routledge, Cardiff Indicators in promoting prudent prescribing: University Experience in Wales (2002-14) 8.30 Economic evaluation of antibiotic central venous Dr Colin Ridyard, Bangor University catheters in paediatric intensive care settings 9.00 Close and depart Gogledd Cymru North Local Practice Forum Fforwm Practisiau Lleol SYMPOSIWM YMCHWIL MEDDYGINIAETHAU GOGLEDD CYMRU North Wales Medicines Research Symposium 1af Gorffennaf 2015 Gwesty Faenol Fawr, Bodelwyddan Rhaglen 6.00 Bwffe & Darllen posteri 6.40 Croeso Yr Athro Dyfrig Hughes, Prifysgol Bangor 6.45 Prif gyflwyniad: “Diffyg ymlyniad at feddyginiaeth: Yr Athro Andrew Farmer, Prifysgol rheoli problem gymhleth” Rhydychain 7.30 Therapi ensymau a gyfeirir gan nanoronynnau Dr Jenny Halliwell, Prifysgol Bangor magnetig 7.50 Defnyddio derbyniadau oherwydd anafiadau Janet Thomas, Bwrdd Iechyd aciwt i'r arennau -

Hospital Inspection (Unannounced) Ysbyty Glan Clwyd, Betsi Cadwaladr University Health Board, Ward 1 and Ward 2B
Hospital Inspection (Unannounced) Ysbyty Glan Clwyd, Betsi Cadwaladr University Health Board, Ward 1 and Ward 2B Inspection date: 4,5,6 July 2017 Publication date: 9 October 2017 This publication and other HIW information can be provided in alternative formats or languages on request. There will be a short delay as alternative languages and formats are produced when requested to meet individual needs. Please contact us for assistance. Copies of all reports, when published, will be available on our website or by contacting us: In writing: Communications Manager Healthcare Inspectorate Wales Welsh Government Rhydycar Business Park Merthyr Tydfil CF48 1UZ Or via Phone: 0300 062 8163 Email: [email protected] Fax: 0300 062 8387 Website: www.hiw.org.uk Digital ISBN 978-1-78859-415-8 © Crown copyright 2017 Contents 1. What we did ....................................................................................................... 5 2. Summary of our inspection ................................................................................ 6 3. What we found ................................................................................................... 7 Quality of patient experience ............................................................................. 8 Delivery of safe and effective care .................................................................. 16 Quality of management and leadership ........................................................... 23 4. What next? ...................................................................................................... -
Digital Networking Across North Wales
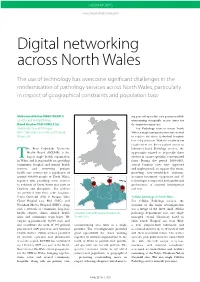
LABORATORIES www.hospitalhealthcare.com Digital networking across North Wales The use of technology has overcome significant challenges in the modernisation of pathology services across North Wales, particularly in respect of geographical constraints and population base Muhammad Aslam MBBS FRCPATH support sub-specialist care provision while Clinical Lead Histopathology maintaining acceptable access times for David Fletcher PhD FIBMS C.Sci the majority of patients. Directorate General Manager For Pathology services across North Betsi Cadwaladr University Health Board, Wales, a single managed service was created Bangor, UK to replace the three individual hospital- based departments. With the relatively low requirement for direct patient access to he Betsi Cadwaladr University laboratory-based Pathology services, the Health Board (BCUHB) is the opportunity existed to re-provide these Tlargest single health organisation services in a more specialist, concentrated in Wales, and is responsible for providing form. During the period 2010–2015, community, hospital and mental health several business cases were approved services, and overseeing primary and implemented, to support this vision, health care services for a population of providing new/refurbished premises, around 680,000 people in North Wales, specialist laboratory equipment and IT together with providing some services technologies to improved both quality and to residents of North Powys and parts of performance of essential investigations Cheshire and Shropshire. The services and tests. are provided from three acute hospitals: Ysbyty Gwynedd (YG) in Bangor; Glan Cellular pathology in North Wales Clwyd Hospital near Rhyl (YGC); and For Cellular Pathology services, the Wrexham Maelor Hospital (YMW), along outcome of this major reconfiguration with a network of community hospitals, was a merge of the three small cellular health centres, clinics, mental health Location of BCUHB Acute Hospitals in pathology departments into one single units and community team bases. -

11 Bodelwyddan Avenue Old Colwyn Conwy LL29 9NP
Cadwgan Surgery The map of our Practice Area 11 Bodelwyddan Avenue Old Colwyn Conwy LL29 9NP Telephone Emergencies only 515410 Appointments 515787 The area covered by the Practice Fax 513270 www.cadwgansurgery.org Practice boundary (for ------------ Drs Roberts, Parry, Stone, Ratchford, Williamson, patients previously Lansberry, Jones and Michael registered with the Practice) 36 NHS Direct Wales (www.nhsdirect.wales.nhs.uk) 0845 4647 Contents NHS Immunisation Information (www.immunisation.nhs.uk) Page No. North Wales Relate (www.relate.org.uk) 01492 533919 Welcome to Cadwgan/Doctors/Nurses/HCAs/ 4-6 Practice Manager Occupational Therapy Social Services 01492 531332 Attached Staff 7-8 Organ Donation Wales ( www.organdonationwales.org ) 03001232323 Surgery Hours/Appointments/Home Visits/ 8-11 Physiotherapy Department (Colwyn Bay Hospital) 01492 807519 Emergency Care Royal Alexandra Hospital, Rhyl 01745 443000 Test Results 11 Samaritans (www.samaritans.org.uk) 01745 354545 Ordering Prescriptions/Repeat Prescriptions 12 Screening for Life ( www.screeningforlife.wales.nhs.uk/home ) Booking Hospital Transport 12 - information about AAA, Breast, Cervical, Bowel, Antenatal, Newborn Hearing, Newborn Bloodspot screening in Wales Sickness Certificates 13 02920397222 Social Services Older Peoples Team 01492 575600 Private Work/Fees 13 Speech and Language Therapy (SALT) 01745583910 Patient Participation Group 14 St David’s Hospice, Llandudno 01492 879058 Health Services 14 St Kentigern’s Hospice, St Asaph 01745 585221 Immunisations 14-16 Tros Gynnal -

Bodelwyddan Key Strategic Site
APPENDIX 2 Denbighshire County Council Draft Site Development Brief: Bodelwyddan Key Strategic Site Consultation Report Development Planning and Policy Team July 2014 DRAFT SITE DEVELOPMENT BRIEF: BODELWYDDAN KEY STRATEGIC SITE CONSULTATION REPORT July 2014 1. CONSULTATION UNDERTAKEN 1.1 Consultation on the draft Site Development Brief: Bodelwyddan Key Strategic Site ran for 8 weeks from 31st March to 26th May 2014. This was a public consultation and was open for anyone to respond. The consultation included the following: Letters were sent to approximately 1,300 people. This included anyone on the LDP database; public bodies; statutory consultees; local, regional and national organisations with an interest in the LDP; and neighbouring Local Authorities and City, Town & Community Councils Town & Community Councils received hard copies of all the consultation documents and response forms Council libraries and One‐Stop‐Shops also received hard copies of the consultation documents and response forms Two drop‐in events were held in Bodelwyddan Community Centre (2nd and 12th May) Officers attended a public meeting organised by Bodelwyddan Development Action Group The draft Site Development Brief was published on the Council’s website, with electronic versions of the response form available to download A press release was issued before the consultation period and a public notice placed in local newspapers 1.2 A total of 107 responses were received, largely from local residents. Representations also included comments from Bodelwyddan Town Council, Rhuddlan Town Council, Dwr Cymru/Welsh Water, Natural Resources Wales, AONB Joint Advisory Committee, Betsi Cadawaladr University Health Board, North Wales Police, and Menter Iath Sir Dinbych. -

Radiology Service – Betsi Cadwaladr University Health Board
Radiology Service – Betsi Cadwaladr University Health Board Audit year: 2016 Date issued: June 2017 Document reference: 238A2017 This document has been prepared as part of work performed in accordance with statutory functions. In the event of receiving a request for information to which this document may be relevant, attention is drawn to the Code of Practice issued under section 45 of the Freedom of Information Act 2000. The section 45 code sets out the practice in the handling of requests that is expected of public authorities, including consultation with relevant third parties. In relation to this document, the Auditor General for Wales and the Wales Audit Office are relevant third parties. Any enquiries regarding disclosure or re-use of this document should be sent to the Wales Audit Office at [email protected]. The team who delivered the work comprised Tracey Davies, Philip Jones and Katrina Febry. Contents Overall, we concluded that day-to-day operations are well managed, but increasing demand, workforce challenges, poor IT systems, aging equipment and weak strategic planning present risks to future service delivery. Summary report Background 4 Our main findings 7 Recommendations 8 Detailed report Factors affecting patient experience Out-of-hours access to radiology services is limited but waiting times and reporting times are generally good. Audit arrangements are comprehensive and there is an effective culture for learning from incidents 10 Demand and capacity issues affecting service performance Demand for radiology services is generally beyond local control and despite workforce challenges, productivity is higher than average. Problems with IT systems inhibit more effective appointment booking 26 Extent to which radiology services are well managed Site-level management arrangements are clear, although there is no overall strategic plan for radiology and senior staff lack confidence in directorate management arrangements. -

Training & Living in North Wales
+ Training & Living in North Wales + A guide for anaesthetic doctors rotating to North Wales Helping you and your family prepare for moving to North Wales: • Life in North Wales • Where to live • Where to go out • Training opportunities • Contact details • Helpful tips Edition 1.2 Jul-16 2 12 + Congratulations! Llongyfarchiadau! Da iawn! If you are reading this you have Outstanding Natural Beauty. It is no wonder succeeded in gaining a post that will bring that so many people come back every year you to one of the most beautiful parts of the for their holidays. world. If you have never been to North For some of you, North Wales may not have Wales before you are in for a very pleasant been your first choice of a place to work. surprise! That’s OK; we understand it is a long way to You will be living and working in a popular travel from South Wales. It’s even worse if holiday region with a unique history and you are separated from partners or family. culture. On the doorstep of Snowdonia We will do our best to help you get the most National Park; perfect for adventures in the out of your time in North Wales; and we are outdoors or losing yourself amongst the confident that when your rotation here has scenery that inspired Tolkien. You will also ended you will leave with very happy be a stones throw from the breathtaking memories. Many of you will be pleasantly coastline of Anglesey and the Llyn Peninsula surprised and will want to come back here with stunning beaches for watersports, for consultant jobs! We value our doctors in strolling or just relaxing to get away from it training. -

12 July 2013 Darren Millar AM Chair Public Accounts Committee
Swyddfa Bangor | Bangor Office 11 Llys Castan | 11 Chestnut Court Ffordd y Parc Parc Menai Bangor Gwynedd LL57 4FH Ffôn | Tel: 01248 679 284 12th July 2013 Darren Millar AM Chair Public Accounts Committee National Assembly for Wales Cardiff Dear Mr Millar Public Accounts Committee – Governance Arrangements at Betsi Cadwaladr University Health Board Thank you for your letter of the 3rd July 2013, relating to the Public Accounts Committee inquiry into the findings of the recent joint report from the Auditor General for Wales and Healthcare Inspectorate Wales on ‘An Overview of Governance Arrangements - Betsi Cadwaladr University Health Board.’ The North Wales Community Health Council (‘CHC’) is willing to co-operate in providing evidence for your inquiry and I trust that the following will provide the Public Accounts Committee with a detailed view of the CHC’s position relating to the public consultation ‘Healthcare in North Wales is Changing’ and the CHC’s response to the joint report. For ease of reference, the evidence on behalf of the CHC is provided in several parts. All documents are listed in chronological order on the relevant indexes: Appendix A - Healthcare in North Wales is Changing (response and press releases) Appendix B - Correspondence with the Minister for Health and Social Services Appendix C - Action following publication of the joint report ‘An Overview of Governance Arrangement – Betsi Cadwaladr University Health Board’. Following Ministerial direction, the CHC and the health board have reached a local agreement in accordance with the National Guidance for Engagement and Consultation on Changes to Health Services in Wales. A joint letter dated 3rd July 2013 (copy included in Appendix B) has been submitted to the Minister’s office and confirmation of receipt acknowledged on the 5th July 2013. -
Glan Clwyd Hospital Foundation Programme Year 1 Updated: August 2020
Glan Clwyd Hospital Foundation Programme Year 1 Updated: August 2020 1 Welcome to North Wales Discover…. Snowdonia Beautiful beaches North Wales is the Adrenaline Capital of the UK Famous zip wires Surf Snowdonia 2 Glan Clwyd hospital is a 5 minute drive from Grwych Castle, location for 2020 I’m a Celebrity Get Me Out of Here. 35 minute drive to the historical city of Chester – fantastic for shopping and eating out One hour drive to Manchester Airport Working at Betsi Cadwaladr University Local Health Board Betsi Cadwaladr University Health Board is the largest health organisation in Wales, providing a full range of primary, community, mental health and acute hospital services for a population of around 676,000 people across the six counties of North Wales (Anglesey, Gwynedd, Conwy, Denbighshire, Flintshire and Wrexham) as well as some parts of mid Wales, Cheshire and Shropshire. The Health Board employs around 16,500 staff and has a budget of around £1.2billion. It is responsible for the operation of three district general hospitals (Ysbyty Gwynedd in Bangor, Ysbyty Glan Clwyd near Rhyl, and Wrexham Maelor Hospital) as well as 22 other acute and community hospitals, and a network of over 90 health centres, clinics, community health team bases and mental health units. It also coordinates the work of 107 GP practices and NHS services provided by North Wales dentists, opticians and pharmacies. 3 Glan Clwyd Hospital (Ysbyty Glan Clwyd) Glan Clwyd Hospital is located in an area of recognised natural beauty with Snowdonia, stunning pristine beaches and enchanting castles all nearby. The local area offers a wide variety of lifestyle and family options, and for those keen to maintain ties further afield, the area has excellent transport links including fast direct trains to London. -
Betsi Cadwaladr University Health Board Summer Vacation Placements 2020
Betsi Cadwaladr University Health Board Summer Vacation Placements 2020 We are the largest health organisation in Wales, servicing a quarter of the population. We provide a bilingual integrated acute and community service across North Wales. We are a friendly, innovative and progressive pharmacy team, benefitting from recent redesign, automation (robotic dispensing) and e- discharges. Our strong links with Bangor and Glyndwr Universities mean we capitalise on academic expertise to innovate healthcare for the future. Each year we recruit pre-registration pharmacists and Foundation grade pharmacists to funded Clinical Diploma/MSc programmes. Within the Health Board we have 3 acute hospital sites In the Central Area - Ysbyty Glan Clwyd Hospital, Bodelwyddan, LL18 5UJ In the East Area - Ysbyty Maelor Hospital, Wrexham, LL13 7TD In the West Area - Ysbyty Gwynedd Hospital, Bangor, LL57 2PW Visit our website for further information: https://www.trainworklivenorthwales.co.uk/pharmacy/ What are we offering? We are offering unpaid placements for up to 1 week to pharmacy undergraduates during June and July 2020. These placements will provide you with an opportunity to undertake a short period of work experience in a hospital and primary care health environment. A rotational programme will be designed to provide experience in the following areas: • Clinical Services on wards and/or in clinics • Procurement and Stores • Aseptic Unit/Non-sterile Production • Medicines Information • Primary Care How to Apply Applications are welcomed from all MPharm students but priority will be given to MPharm year 3 students. If you are interested send: • A copy of your CV which needs to include contact details for 2 suitable people who are able to provide a reference for you.