Pre-HCT Treatment for Hodgkin's / Non-Hodgkin's Lymphoma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Page 1 EXAMPLES of ACUTE TOXINS (By CAS#) APPENDIX V(H)-B
EXAMPLES OF ACUTE TOXINS (by CAS#) APPENDIX V(h)-B Key: SA -- Readily Absorbed Through the Skin Revised: 12/2012 ___________________________________________________ _____________ _________________________ | | | CHEMICAL NAME CAS # | SA | TARGET ORGAN | ___________________________________________________ ____________ | _ | _______________________ | AFLATOXINS 000000-00-0 | | systemic | ANILINE AND COMPOUNDS 000000-00-0 | x | blood | ARSENIC ACID AND SALTS 000000-00-0 | x | systemic | ARSENIUOS ACID AND SALTS 000000-00-0 | | systemic | ARSONIC ACID AND SALTS 000000-00-0 | | systemic | BOTULINUM TOXINS 000000-00-0 | | systemic | CYANIDE AND COMPOUNDS 000000-00-0 | x | blood | CYANOGEN AND COMPOUNDS 000000-00-0 | | blood | METHYL MERCURY AND COMPOUNDS 000000-00-0 | x | CNS | VENOM, SNAKE, CROTALUS ADAMANTEUS 000000-00-0 | | systemic | VENOM, SNAKE, CROTALUS ATROX 000000-00-0 | | systemic | MITOMYCIN C 000050-07-7 | | systemic | DINITROPHENOL, 2,4- 000051-28-5 | x | systemic | ATROPINE 000051-55-8 | x | CNS | HN2 (NITROGEN MUSTARD-2) 000051-75-2 | x | systemic | THIOTEPA 000052-24-4 | | systemic | NICOTINE 000054-11-5 | x | CNS | NITROGEN MUSTARD HYDROCHLORIDE 000055-86-7 | x | systemic | PARATHION 000056-38-2 | x | CNS | CYANIDE 000057-12-5 | x | blood | STRYCHNINE 000057-24-9 | | systemic,CNS | TUBOCURARINE CHLORIDE HYDRATE,(+)- 000057-94-3 | x | systemic | METHYL HYDRAZINE 000060-34-4 | x | pulmonary,CNS,blood | ANILINE 000062-53-3 | x | blood | DICHLORVOS 000062-73-7 | x | systemic | SODIUM FLUOROACETATE 000062-74-8 | x | systemic | COLCHICINE -

The Chemotherapy of Malignant Disease -Practical and Experimental Considerations
Postgrad Med J: first published as 10.1136/pgmj.41.475.268 on 1 May 1965. Downloaded from POSTGRAD. MED. J. (1965), 41,268 THE CHEMOTHERAPY OF MALIGNANT DISEASE -PRACTICAL AND EXPERIMENTAL CONSIDERATIONS JOHN MATTHIAS, M.D., M.R.C.P., F.F.A., R.C.S. Physician, The Royal Marsden Hospital, London, S.W.3. THE TERM chemotherapy was introduced by positively charged alkyl (CH2) radicles of Ehrlich to describe the specific and effective the agent. treatment of infectious disease by chemical (a) The nitrogen mustards: mustine (HN2 substances. It is currently also applied to the 'nitrogen mustard', mechlorethamine, treatment of malignant disease. Unfortunately mustargen), trimustine (Trillekamin no aspect of tumour metabolism has been HN3), chlorambucil (Leukeran, phenyl discovered which has allowed the development butyric mustard), melphalan (Alkeran, of drugs capable of acting specifically upon the phenyl alanine mustard), uramustine malignant cell, so that cytotoxic drugs also (Uracil mustard), cyclophosphamide affect normal cells to a greater or lesser degree. (Endoxan or Cytoxan), mannomustine The most susceptible or sensitive of the normal (DegranoO). tissues are those with the highest rates of cell (b) The ethylenamines: tretamine (trie- turnover and include the haemopoietic and thanomelamine, triethylene melamine, lympho-reticular tissues, the gastro-intestinal TEM), thiotepa (triethylene thiopho- the the testis and the hair epithelium, ovary, sphoramide), triaziquone (Trenimon).by copyright. follicles. (c) The epoxides: triethyleneglycoldigly- Cancer chemotherapy may be said to encom- cidyl ether (Epodyl). pass all treatments of a chemical nature (d) The sulphonic acid esters: busulphan administered to patients with the purpose of (Myleran), mannitol myleran. restricting tumour growth or destroying tumour 2. -

Hodgkin Lymphoma Treatment Regimens
HODGKIN LYMPHOMA TREATMENT REGIMENS (Part 1 of 5) Clinical Trials: The National Comprehensive Cancer Network recommends cancer patient participation in clinical trials as the gold standard for treatment. Cancer therapy selection, dosing, administration, and the management of related adverse events can be a complex process that should be handled by an experienced health care team. Clinicians must choose and verify treatment options based on the individual patient; drug dose modifications and supportive care interventions should be administered accordingly. The cancer treatment regimens below may include both U.S. Food and Drug Administration-approved and unapproved indications/regimens. These regimens are provided only to supplement the latest treatment strategies. These Guidelines are a work in progress that may be refined as often as new significant data become available. The NCCN Guidelines® are a consensus statement of its authors regarding their views of currently accepted approaches to treatment. Any clinician seeking to apply or consult any NCCN Guidelines® is expected to use independent medical judgment in the context of individual clinical circumstances to determine any patient’s care or treatment. The NCCN makes no warranties of any kind whatsoever regarding their content, use, or application and disclaims any responsibility for their application or use in any way. Classical Hodgkin Lymphoma1 Note: All recommendations are Category 2A unless otherwise indicated. Primary Treatment Stage IA, IIA Favorable (No Bulky Disease, <3 Sites of Disease, ESR <50, and No E-lesions) REGIMEN DOSING Doxorubicin + Bleomycin + Days 1 and 15: Doxorubicin 25mg/m2 IV push + bleomycin 10units/m2 IV push + Vinblastine + Dacarbazine vinblastine 6mg/m2 IV over 5–10 minutes + dacarbazine 375mg/m2 IV over (ABVD) (Category 1)2-5 60 minutes. -

Cancer Drug Pharmacology Table
CANCER DRUG PHARMACOLOGY TABLE Cytotoxic Chemotherapy Drugs are classified according to the BC Cancer Drug Manual Monographs, unless otherwise specified (see asterisks). Subclassifications are in brackets where applicable. Alkylating Agents have reactive groups (usually alkyl) that attach to Antimetabolites are structural analogues of naturally occurring molecules DNA or RNA, leading to interruption in synthesis of DNA, RNA, or required for DNA and RNA synthesis. When substituted for the natural body proteins. substances, they disrupt DNA and RNA synthesis. bendamustine (nitrogen mustard) azacitidine (pyrimidine analogue) busulfan (alkyl sulfonate) capecitabine (pyrimidine analogue) carboplatin (platinum) cladribine (adenosine analogue) carmustine (nitrosurea) cytarabine (pyrimidine analogue) chlorambucil (nitrogen mustard) fludarabine (purine analogue) cisplatin (platinum) fluorouracil (pyrimidine analogue) cyclophosphamide (nitrogen mustard) gemcitabine (pyrimidine analogue) dacarbazine (triazine) mercaptopurine (purine analogue) estramustine (nitrogen mustard with 17-beta-estradiol) methotrexate (folate analogue) hydroxyurea pralatrexate (folate analogue) ifosfamide (nitrogen mustard) pemetrexed (folate analogue) lomustine (nitrosurea) pentostatin (purine analogue) mechlorethamine (nitrogen mustard) raltitrexed (folate analogue) melphalan (nitrogen mustard) thioguanine (purine analogue) oxaliplatin (platinum) trifluridine-tipiracil (pyrimidine analogue/thymidine phosphorylase procarbazine (triazine) inhibitor) -

Vincristine (Conventional): Drug Information
Official reprint from UpToDate® www.uptodate.com ©2017 UpToDate® Vincristine (conventional): Drug information Copyright 1978-2017 Lexicomp, Inc. All rights reserved. (For additional information see "Vincristine (conventional): Patient drug information" and see "Vincristine (conventional): Pediatric drug information") For abbreviations and symbols that may be used in Lexicomp (show table) Special Alerts Vincristine Sulfate Safety Alert October 2015 Health Canada is notifying health care providers that certain lots of Hospira’s vincristine sulfate 1 mg/mL injection (DIN 02183013: 2 mL vial, list #7077A001; 5 mL vial, list #7082A001) have incorrect or outdated safety information on the inner/outer labels and package insert, which may increase the risk to patients and may result in significant patient harm requiring medical intervention. These warnings include: - Vincristine should only be administered by the intravenous (IV) route. Administration of vincristine by any other route can be fatal. - Syringes containing this product should be labeled “Warning - for IV use only.” - Extemporaneously prepared syringes containing this product must be packaged in an overwrap which is labeled “Do not remove covering until moment of injection. For IV use only - fatal if given by other routes.” - Contraindication of vincristine in patients with demyelinating Charcot-Marie-Tooth syndrome. - Potential risk of acute shortness of breath when vincristine is coadministered with mitomycin-C and GI toxicities including necrosis with administration of vincristine. Health care providers are requested to consult with the approved Canadian product monograph for vincristine sulfate 1 mg/mL for the most updated information. Consumers with questions should contact their health care provider for more information. ALERT: US Boxed Warning Experienced physician: Vincristine should be administered by individuals experienced in the administration of the drug. -

HODGKIN LYMPHOMA TREATMENT REGIMENS (Part 1 of 2)
HODGKIN LYMPHOMA TREATMENT REGIMENS (Part 1 of 2) The selection, dosing, and administration of anticancer agents and the management of associated toxicities are complex. Drug dose modifications and schedule and initiation of supportive care interventions are often necessary because of expected toxicities and because of individual patient variability, prior treatment, and comorbidities. Thus, the optimal delivery of anticancer agents requires a healthcare delivery team experienced in the use of such agents and the management of associated toxicities in patients with cancer. The cancer treatment regimens below may include both FDA-approved and unapproved uses/regimens and are provided as references only to the latest treatment strategies. Clinicians must choose and verify treatment options based on the individual patient. NOTE: GREY SHADED BOXES CONTAIN UPDATED REGIMENS. REGIMEN DOSING Classical Hodgkin Lymphoma—First-Line Treatment General treatment note: Routine use of growth factors is not recommended. Leukopenia is not a factor for treatment delay or dose reduction (except for escalated BEACOPP).1 CR=complete response IPS=International Prognostic Score PD=progressive disease PFTs=pulmonary function tests PR=partial response RT=radiation therapy SD=stable disease Stage IA, IIA Favorable ABVD (doxorubicin [Adriamycin] Days 1 and 15: Doxorubicin 25mg/m2 IV + bleomycin 10mg/m2 IV + vinblastine + bleomycin + vinblastine + 6mg/m2 IV + dacarbazine 375mg/m2 IV. dacarbazine [DTIC-Dome]) + Repeat cycle every 4 weeks for 2–4 cycles. involved-field radiotherapy (IFRT)1–4 Follow with IFRT after completion of chemotherapy. Abbreviated Stanford V Weeks 1, 3, 5 and 7: Vinblastine 6mg/m2 IV + doxorubicin 25mg/m2 IV. (doxorubicin + vinblastine + Weeks 1 and 5: Mechlorethamine 6mg/m2. -

(Rituxan®), Rituximab-Abbs (Truxima®), Rituximab-Pvvr (Ruxience®) Prior Authorization Drug Coverage Policy
1 Rituximab Products: Rituximab (Rituxan®), Rituximab-abbs (Truxima®), Rituximab-pvvr (Ruxience®) Prior Authorization Drug Coverage Policy Effective Date: 2/1/2021 Revision Date: n/a Review Date: 7/2/20 Lines of Business: Commercial Policy type: Prior Authorization This Drug Coverage Policy provides parameters for the coverage of rituximab (Rituxan®), rituximab-abbs (Truxima®), and rituximab-pvvr (Ruxience®). Consideration of medically necessary indications are based upon U.S. Food and Drug Administration (FDA) indications, recommended uses within the Centers of Medicare & Medicaid Services (CMS) five recognized compendia, including the National Comprehensive Cancer Network (NCCN) Drugs & Biologics Compendium (Category 1 or 2A recommendations), and peer-reviewed scientific literature eligible for coverage according to the CMS, Medicare Benefit Policy Manual, Chapter 15, section 50.4.5 titled, “Off- Label Use of Anti-Cancer Drugs and Biologics.” This policy evaluates whether the drug therapy is proven to be effective based on published evidence-based medicine. Drug Description1-3 Rituximab (Rituxan®), rituximab-abbs (Truxima®), and rituximab-pvvr (Ruxience®) are monoclonal antibodies that target the CD20 antigen expressed on the surface of pre-B and mature B- lymphocytes. Upon binding to cluster of differentiation (CD) 20, rituximab mediates B-cell lysis. Possible mechanisms of cell lysis include complement dependent cytotoxicity (CDC) and antibody dependent cell mediated cytotoxicity (ADCC). B cells are believed to play a role in the pathogenesis of rheumatoid arthritis (RA) and associated chronic synovitis. In this setting, B cells may be acting at multiple sites in the autoimmune/inflammatory process, including through production of rheumatoid factor (RF) and other autoantibodies, antigen presentation, T-cell activation, and/or proinflammatory cytokine production. -
R-Chop-21 / Chop-21
Lymphoma group R-CHOP-21 / CHOP-21 INDICATION Lymphoma Omit rituximab if CD20-negative. TREATMENT INTENT Curative or disease modification depending on clinical circumstances PRE-ASSESSMENT 1. Ensure histology is confirmed prior to administration of chemotherapy and document in notes. 2. Record stage and IPI of disease - CT scan (neck, chest, abdomen and pelvis), and/or PET- CT, presence or absence of B symptoms, clinical extent of disease, consider bone marrow aspirate and trephine. 3. Blood tests – FBC, U&Es, LDH, ESR, urate, calcium, Vitamin D level,magnesium, creatinine, LFTs, glucose, Igs, β2 microglobulin, hepatitis B core antibody and hepatitis B surface Ag, hepatitis C antibody, EBV, CMV, VZV, HIV 1+2 after consent, group and save. 4. Urine pregnancy test • before cycle 1 of each new chemotherapy course for women of child- bearing age unless they are post-menopausal, have been sterilised or undergone a hysterectomy. 5. ECG +/- Echo and baseline BP in all patients with a cardiac history or at risk of cardiac complications (hypertension, smokers, diabetes). 6. Record performance status (WHO/ECOG). 7. Record height and weight. 8. Consent - ensure patient has received adequate verbal and written information regarding their disease, treatment and potential side effects. Document in medical notes all information that has been given. Obtain written consent on the day of treatment. 9. Fertility - it is very important the patient understands the potential risk of infertility. All patients should be offered fertility advice by referring to the Oxford Fertility Unit. 10. Hydration – in patients with bulky disease pre-hydrate with sodium chloride 0.9% 1 litre over 4- 6 hours. -

Salvage Chemotherapy for Recurrent Primary Brain Tumors in Children
Salvage chemotherapy for recurrent primary brain tumors in children Jan van Eys, PhD, MD, Tallie Z. Baram, MD, PhD, Ayten Cangir, MD, Janet M. Bruner, MD, and J. Martinez-Prieto, MD From the Departments of Pediatrics, Neurooncology, and Pathology, The Universityof Texas M, D. Anderson Cancer Center at Houston Sixty consecutive evaluable children with recurrent primary tumors of the central nervous system were treated with a regimen of vincristine, nitrogen mustard, procarbazine, and prednisone over a 12-year period. Tumor types included medulloblastoma (19), brain-stem glioma (16), astrocytoma (13), and a miscellaneous glioma (12). Responses and sustained survivals were achieved. Responses were highly dependent on tumor type. Disease progres- sion was halted in 73% of the children with medulloblastoma, and three have survived in complete remission for more than 10 years from the start of therapy with vincristine, nitrogen mustard, procarbazine, and prednisone. Two of four patients with anaplastic glioma, are long-term survivors. In contrast, less than one third of children with brain-stem gliomas responded. Toxicity consisted mainly of neutropenia, thrombocytopenia, infections, and rarely a procarba- zine rash. (J PEDIAI'R1988;113:601-6) Therapy for recurrent brain tumors in children remains METHODS unsatisfactory; most die of their disease regardless of Patients. Sixty-five children with a median age of 6 therapy, l We have repbrted on the responsiveness of years (range, 1 to 16 years) were treated with MOPP for recurrent brain tumors in children to chemotherapy with recurrent brain tumors. Sixty patients were eligible for vincristine, nitrogen mustard, procarbazine, and predni- evaluation; the other five patients were excluded because 1 sone. -

Anaplastic Large Cell Lymphoma (ALCL)
Helpline (freephone) 0808 808 5555 [email protected] www.lymphoma-action.org.uk Anaplastic large cell lymphoma (ALCL) This page is about anaplastic large-cell lymphoma (ALCL), a type of T-cell lymphoma. On this page What is ALCL? Who gets it? Symptoms Treatment Relapsed and refractory ALCL Research and targeted treatments We have separate information about the topics in bold font. Please get in touch if you’d like to request copies or if you would like further information about any aspect of lymphoma. Phone 0808 808 5555 or email [email protected]. What is ALCL? Anaplastic large cell lymphoma (ALCL) is a type of T-cell lymphoma – a non-Hodgkin lymphoma that develops from white blood cells called T cells. Under a microscope, the cancerous cells in ALCL look large, undeveloped and very abnormal (‘anaplastic’). There are four main types of ALCL. They have complicated names based on their features and the types of proteins they make: • ALK-positive ALCL (also known as ALK+ ALCL) is the most common type. In ALK-positive ALCL, the abnormal T cells have a genetic change (mutation) that means they make a protein called ‘anaplastic lymphoma kinase’ (ALK). In other words, they test positive for ALK. ALK-positive ALCL is a fast-growing (high-grade) lymphoma. Page 1 of 6 © Lymphoma Action • ALK-negative ALCL (also known as ALK- ALCL) is a high-grade lymphoma that accounts for around 3 in every 10 cases of ALCL. The abnormal T cells do not make the ALK protein – they test negative for ALK. -
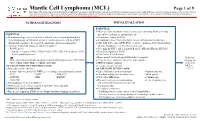
Mantle Cell Lymphoma (MCL)
Mantle Cell Lymphoma (MCL) Page 1 of 9 Disclaimer: This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson’s specific patient population, services and structure, and clinical information. This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient's care. This algorithm should not be used to treat pregnant women. PATHOLOGIC DIAGNOSIS INITIAL EVALUATION ESSENTIAL: ● Physical exam: attention to node-bearing areas, including Waldeyer's ring, ESSENTIAL: size of liver and spleen, and patient’s age ● Hematopathology review of all slides with at least one tumor paraffin block. ● Performance status (ECOG) Hematopathology confirmation of classic versus aggressive variant of MCL ● B symptoms (fever, drenching night sweats, unintentional weight loss) (blastoid/pleomorphic). Re-biopsy if consult material is non-diagnostic. ● CBC with differential, LDH, BUN, creatinine, albumin, AST, total bilirubin, 1 ● Adequate immunophenotype to confirm diagnosis alkaline phosphatase, serum calcium, uric acid ○ Paraffin panel: ● Screening for HIV 1 and 2, hepatitis B and C (HBcAb, HBaAg, HCVAb) - Pan B-cell marker (CD19, CD20, PAX5), CD3, CD5, CD10, and cyclin D1 ● Beta-2 microglobulin (B2M) - Ki-67 (proliferation rate) ● Chest x-ray, PA and lateral or ● Bone marrow bilateral biopsy with unilateral aspirate Induction ○ Flow cytometry immunophenotyping: -
Anticancer Alkylating Agents-Part-I.Pdf
Anticancer Agents Medicinal Chemistry III B Pharm Dr. bilal al-jaidi Assistant Professor, Pharmaceutical Medicinal Chemistry Faculty of Pharmacy, Philadelphia University-Jordan Email: [email protected] Learning Outcome At the end of this lesson students will be able to – Outline the current status, causes and treatment strategies of cancer – Explain the mechanism of action, SAR, therapeutic uses and side effects of following classes of anti-cancer agents: • Alkylating Agents QUIZ = 20 Marks • Heavy metal compounds (Metallating Agents) • Anti-metabolite • Antibiotics • Plant Extracts • Topoisomerase inhibitors • Hormones • Combination of chemotherapy with other treatments • Others First Examination= 20 Marks The Status of Cancer • Cancer is a leading cause of death worldwide, accounting for 12.6 million new cases and 7.6 million deaths every year. THIS IS EQUIVALENT TO ONE PERSON, EVERY 5 SECONDS OF EVERYDAY Source: GLOBOCAN 2008 By 2020 the World Health Organisation (WHO) expects this rise to 16 million. Cancer • A new growth of tissue in which multiplication of cells is uncontrolled and progressive (tumour). • Abnormal cells can spread to other parts of the body (metastasise). Cancer Types Cancer types are categorized based on the functions/locations of the cells from which they originate: Carcinoma: a tumor derived from epithelial cells, those cells that line the inner or outer surfaces of our skin and organs (80-90% of all cancer cases reported) Sarcoma: a tumor derived from muscle, bone, cartilage, fat or connective tissues. Leukemia: a cancer derived from white blood cells or their precursors. Lymphoma: a cancer of bone marrow derived cells that affects the lymphatic system. Myelomas: a cancer involving the white blood cells responsible for the production of antibodies (B lymphocytes).