A Case of Isolated Nasal Bone Osteomyelitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nasal Morphology and Its Correlation to Craniofacial Morphology in Lateral Cephalometric Analysis
International Journal of Environmental Research and Public Health Article Nasal Morphology and Its Correlation to Craniofacial Morphology in Lateral Cephalometric Analysis Agnieszka Jankowska 1 , Joanna Janiszewska-Olszowska 2,* and Katarzyna Grocholewicz 2 1 Private Practice “Dental Clinic Jankowscy”, 68-200 Zary,˙ Poland; [email protected] 2 Department of Interdisciplinary Dentistry, Pomeranian Medical University in Szczecin, 70-111 Szczecin, Poland; [email protected] * Correspondence: [email protected]; Tel.: +48-91-466-1690 Abstract: Nose shape, size, and inclination influence facial appearance, but few studies concern the relationship between the nasal profile and craniofacial structures. The objective of this study was to analyze association of nasal cephalometric variables with skeletal structures, age, and sex. Cephalometric and nasal analysis was performed in 386 Polish orthodontic patients (aged 9–25 years). Student t-test and Mann–Whitney test were used to compare quantitative variables and Pearson’s or Spearman’s correlation coefficients—to find correlations. Soft tissue facial convexity angle corre- lates to Holdaway ratio, ANB (A-Nasion-B), and Wits appraisal. Nasal dorsum axis, nose length, nose depth (1) and nose depth (2), nose hump, lower dorsum convexity, and columella convexity increase with age. Nasal base angle, nasolabial angle, nasomental angle, soft tissue facial convex- ity and nasal bone angle decrease with age. Nasal base angle and nasomental angle are smaller in females. Thus, a relationship exists between nasal morphology and sagittal jaw configuration. Nasal parameters significantly change with age. Sexual dimorphism characterizes nasal bone angle Citation: Jankowska, A.; and nasomental angle. Janiszewska-Olszowska, J.; Grocholewicz, K. Nasal Morphology Keywords: nose; nose profile; cephalometry; orthodontics and Its Correlation to Craniofacial Morphology in Lateral Cephalometric Analysis. -

Analysis of Facial Skeletal Morphology: Nasal Bone, Maxilla, and Mandible
Hindawi BioMed Research International Volume 2021, Article ID 5599949, 9 pages https://doi.org/10.1155/2021/5599949 Research Article Analysis of Facial Skeletal Morphology: Nasal Bone, Maxilla, and Mandible Han-Sheng Chen ,1 Szu-Yu Hsiao ,2,3 and Kun-Tsung Lee 4,5 1Dental Department, Kaohsiung Municipal Siao-gang Hospital, Kaohsiung, Taiwan 2School of Dental Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan 3Department of Dentistry for Child and Special Needs, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan 4Division of Clinical Dentistry, Department of Dentistry, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan 5Department of Oral Hygiene, College of Dental Science, Kaohsiung Medical University, Kaohsiung, Taiwan Correspondence should be addressed to Kun-Tsung Lee; [email protected] Received 12 February 2021; Revised 29 March 2021; Accepted 4 May 2021; Published 25 May 2021 Academic Editor: Michael YC Chen Copyright © 2021 Han-Sheng Chen et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The growth and development of facial bones are closely related to each other. The present study investigated the differences in the nasomaxillary and mandibular morphology among different skeletal patterns. Cephalograms of 240 participants were divided into 3 groups based on the skeletal pattern (Class I, Class II, and Class III). The dimensions of nasomaxilla (nasal bone length, nasal ridge length, nasal depth, palatal length, and maxillary height) and mandible (condylar length, ramus length, body length, symphysis length, and entire mandibular length) were measured. One-way analysis of variance and Pearson’s correlation test were used for statistical analysis. -

Dissertation on an OBSERVATIONAL STUDY COMPARING the EFFECT of SPHENOPALATINE ARTERY BLOCK on BLEEDING in ENDOSCOPIC SINUS SURGE
Dissertation On AN OBSERVATIONAL STUDY COMPARING THE EFFECT OF SPHENOPALATINE ARTERY BLOCK ON BLEEDING IN ENDOSCOPIC SINUS SURGERY Dissertation submitted to TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI For M.S.BRANCH IV (OTORHINOLARYNGOLOGY) Under the guidance of DR. F ANTHONY IRUDHAYARAJAN, M.S., D.L.O Professor & HOD, Department of ENT & Head and Neck Surgery, Govt. Stanley Medical College, Chennai. GOVERNMENT STANLEY MEDICAL COLLEGE THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY, CHENNAI-32, TAMILNADU APRIL 2017 CERTIFICATE This is to certify that this dissertation titled AN OBSERVATIONAL STUDY COMPARING THE EFFECT OF SPHENOPALATINE ARTERY BLOCK ON BLEEDING IN ENDOSCOPIC SINUS SURGERY is the original and bonafide work done by Dr. NIGIL SREEDHARAN under the guidance of Prof Dr F ANTHONY IRUDHAYARAJAN, M.S., DLO Professor & HOD, Department of ENT & Head and Neck Surgery at the Government Stanley Medical College & Hospital, Chennai – 600 001, during the tenure of his course in M.S. ENT from July-2014 to April- 2017 held under the regulation of the Tamilnadu Dr. M.G.R Medical University, Guindy, Chennai – 600 032. Prof Dr F Anthony Irudhayarajan, M.S., DLO Place : Chennai Professor & HOD, Date : .10.2016 Department of ENT & Head and Neck Surgery Government Stanley Medical College & Hospital, Chennai – 600 001. Dr. Isaac Christian Moses M.D, FICP, FACP Place: Chennai Dean, Date : .10.2016 Govt.Stanley Medical College, Chennai – 600 001. CERTIFICATE BY THE GUIDE This is to certify that this dissertation titled “AN OBSERVATIONAL STUDY COMPARING THE EFFECT OF SPHENOPALATINE ARTERY BLOCK ON BLEEDING IN ENDOSCOPIC SINUS SURGERY” is the original and bonafide work done by Dr NIGIL SREEDHARAN under my guidance and supervision at the Government Stanley Medical College & Hospital, Chennai – 600001, during the tenure of his course in M.S. -

The Ratio of Biparietal Diameter to Nasal Bone Length
Perinatal Journal • Vol: 18, Issue: 3/December 2010 79 e-Address: http://www.perinataljournal.com/20100183003 The Ratio of Biparietal Diameter to Nasal Bone Length Resul Ar›soy1, Nida Ergin2, Murat Yayla2, Gökhan Göynümer3 1Sa¤l›k Bakanl›¤› Okmeydan› E¤itim Araflt›rma Hastanesi, Kad›n Hastal›klar› ve Do¤um Klini¤i, ‹stanbul, TR 2‹nternational Hospital, Kad›n Hastal›klar› ve Do¤um Klini¤i, ‹stanbul, TR 3Sa¤l›k Bakanl›¤› Göztepe E¤itim Araflt›rma Hastanesi, Kad›n Hastal›klar› ve Do¤um Klini¤i, ‹stanbul, TR Abstract Objective: The aim of this study was to determine the relationship between the ratio of biparietal diameter to nasal bone length and gestational weeks at the second trimester of pregnancy. Methods: We evaluated consecutively fetuses referred to our facility between 15 and 22 weeks’ gestation for perinatal sonography and amniocentesis because of an increased risk of aneuploidy. Anatomically normal and euploid 505 fetuses were included in the study. A detailed structural survey, biometric measurements, and measurement of the nasal bone were obtained before the amnio- centesis procedure. The distribution of fetal nasal bone length between 15-22 gestational weeks was established and their percentiles were calculated. The ratio of biparietal diameter to nasal bone length was calculated for each case. Results: The mean nasal bone length for 15 to 22 week`s gestation was 3.21±0.41, 3.45±0.52, 3.81±0.58, 4.17±0.68, 4.42±0.66, 4.89±0.89, 5.35±0.90 and 5.84±1.02 mm respectively. -

Asian Rhinoplasty
Asian Rhinoplasty Dean M. Toriumi, MDa,*, Colin D. Pero, MDb,c KEYWORDS Asian rhinoplasty Revision rhinoplasty Augmentation rhinoplasty Cosmetic rhinoplasty in the Asian patient popula- Characteristics of the Asian nose include: low tion differs from traditional rhinoplasty approaches nasal dorsum with caudally placed nasal starting in many aspects, including preoperative analysis, point, thick, sebaceous skin overlying the nasal patient expectations, nasal anatomy, and surgical tip and supratip, weak lower lateral cartilages, techniques used. Platyrrhine nasal characteristics small amount of cartilaginous septum, foreshort- are common, with low dorsum, weak lower lateral ened nose, retracted columella, and thickened cartilages, and thick sebaceous skin often noted. alar lobules (Fig. 1). Typically, patients seek augmentation of these ex- Each patient’s desire to balance augmenting isting structures rather than reductive procedures. their Asian nasal features with maintenance of Patient desires and expectations are unique to this the appearance of an Asian nose is unique for population, with patients often seeking improve- each individual and should be elucidated during ment and refinement of their Asian features, not the initial consultation and preoperative visits. radical changes toward more characteristic White Demonstration of the proposed changes to the features. Use of alloplastic or autologous materials patient with a computer-imaging program can is necessary to achieve the desired results; the use aid communication between patient and surgeon of each material carries inherent risks and benefits of the proposed changes (Fig. 2A, C). Fulfillment that should be discussed with the patient. Autolo- of the patient’s stated wishes may produce a modi- gous cartilage, in particular use of costal cartilage, fication of the patient’s ethnic identity, and has shown to be a reliable, low-risk technique, computer imaging helps the patient to better which, when executed properly, produces excel- understand the possible outcome. -

Fetal Nasal Bone Lenght Nomogram
Perinatal Journal• Vol: 14, Issue: 2/June 2006 77 Fetal Nasal Bone Lenght Nomogram Murat Yayla1, Gökhan Göynümer2, Ömer Uysal3 1Clinics of Gynecology and Obstetrics, Haseki Hospital, ‹stanbul 2Clinics of Gynecology and Obstetrics, Göztepe Training and Research Hospital, ‹stanbul 3Department of Statistics, Cerrahpafla Medical Faculty, ‹stanbul University Abstratct Objective: To obtain the nasal bone length nomogram throughout normal gestation with known prognosis, and to compare it with some other growth measurements. Methods: Nasal bone lengths of 540 consecutive cases ranging between 11-39 weeks of pregnancy were measured by ultrasonography prospectively. Biparietal diameter (BPD) and femur lengths (FL) were obtained in the meanwhile. Nasal bone length nomograms of the 276 term fetuses, which were born alive and without malformation were obtained according to, BPD, FL, and gestational week. The correlation between variables was assessed by regression analysis. Results: A linear growth pattern of the nasal bone length was obtained throughout gestation. (Nasal bone length= Gestational week x 0.42- 2.81) (r2 = 0.94). A positive correlation was found between the growth of nasal bone length and the growth of other bone measurements. Conclusion: Measurement of the nasal bone length during gestation shows a linear growth pattern according to gestational week, BPD and FL. Keywords: Fetus, nasal bone, ultrasonography, nomogram Fetal burun kemi¤i uzunluk nomogram› Amaç: Prognozu bilinen normal gebeliklerde fetusun burun kemi¤i uzunlu¤u nomogram›n›n elde edilmesi ve di¤er büyüme ölçümleri ile karfl›- laflt›r›lmas›. Yöntem: Gebeli¤in 11-39 haftalar› aras›nda 540 olguda fetusun burun kemik uzunlu¤u prospektif olarak ultrasonografi ile ölçüldü. -

Nasal Septum Deviation and Inferior Nasal Concha Bone Hypertrophy in Class III Facial Deformity
Int. J. Morphol., 38(6):1544-1548, 2020. Nasal Septum Deviation and Inferior Nasal Concha Bone Hypertrophy in Class III Facial Deformity Desviación del Septum Nasal e Hipertrofia de la Concha Nasal Inferior en Deformidad Facial Clase III Javier Villa1; Leonardo Brito2,3; Marcelo Parra2,4; Pablo Navarro3; Márcio de Moraes6 & Sergio Olate2,4 VILLA, J.; BRITO, L.; PARRA, M.; NACARRO, P.; DE MORAES, M.; OLATE, S. Nasal septum deviation and inferior nasal concha bone hypertrophy in Class III facial deformity. Int. J. Morphol., 38(6):1544-1548, 2020. SUMMARY: The aim of this research was to analyze the morphology of the nasal septum and inferior nasal concha bone in class III facial deformities prior to orthodontic treatment in orthognathic surgery candidates. 40 subjects were included in this research. The inclusion criteria were an Angle class III, negative overjet and SNA angle less than 80º. Patients with facial asymmetry, facial trauma or who had undergone maxillofacial or ENT procedures were excluded. CBCT images were obtained for all the patients and the nasal septum deviation, morphology of inferior nasal concha bone and ostium of the maxillary sinus were analyzed and related to the complexity of the facial deformity expressed by the ANB angle and dental relations. The measurement was standardized by ICC and the data was analyzed using a chi square test and Spearman’s coefficient with a p value < 0.005 for statistical significance. Nasal septal deviation was observed in 77.5 %. The deviation angle was 13.28º (±4.68º) and the distance from the midline to the most deviated septum was 5.56 mm (±1.8 mm) with no statistical relation to the complexity of the facial deformity. -
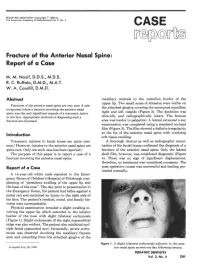
Fracture of the Anterior Nasal Spine: Report of a Case
PEDIATRIC DENTISTRY/Copyright ® 1980 by The American Academy of Pedodontics/Vol. 2, No. 4 CASE Fracture of the Anterior Nasal Spine: Report of a Case M. M. Nazif, D.D.S., M.D.S. R. C. Ruffalo, D.M.D., M.A.T. W. A. Caudill, D.M.D. Abstract maxillary centrals to the vermilion border of the upper lip. Two small areas of abrasion were visible on Fractures of the an tenor nasal spine are very rare. A case the attached gingiva covering the unerupted maxillary is reported where a fracture involving the anterior nasal spine was the only significant sequela of a traumatic injury right and left cuspids (Figure 2). The dentition was to the face. Appropriate methods of diagnosing such a clinically and radiographically intact. The frenum fracture are discussed. area was tender to palpation. A lateral extraoral x-ray examination was completed using a standard occlusal film (Figure 3). The film showed a definite irregularity at the tip of the anterior nasal spine with overlying Introduction soft tissue swelling. Traumatic injuries to facial bones are quite com- A thorough clinical as well as radiographic exami- mon.1 However, injuries to the anterior nasal spine are nation of the facial bones confirmed the diagnosis of a quite rare. Only one such case has been reported.2 fracture of the anterior nasal spine. Only the lateral The purpose of this paper is to report a case of a skull film, however, was considered diagnostic (Figure fracture involving the anterior nasal spine. 4). There was no sign of significant displacement, therefore, no treatment was considered necessary. -

Management of the Post-Traumatic Nasal Deformity
Chapter 174: Management of the Post-Traumatic Nasal Deformity Sameer Ahmed 12/14/11 Background - The nose is the most commonly injured aspect of the face in all maxillofacial injuries due to its prominence and minimal force required to induce fracture. - Traumatic nasal injury alters both the cosmetic nasal appearance and can significantly alter nasal function as well → When assessing blunt nasal trauma, both functional and aesthetic consequences must be considered - Males suffer nasal trauma about twice as often as females; highest incidence between 15 to 30 years. - Most commonly, nasal fractures occur during altercations, sports, motor vehicle and other accidents. Recent studies have shown that airbags do not reduce the incidence of nasal injuries. - Pediatric and elderly facial injuries are most often accidental. Anatomy Bony, cartilaginous, and soft tissue elements. 1. Bony framework is pyramidal - Paired nasal bones articulate with the nasal process of the frontal bone superiorly and ascending process of the maxilla laterally. - Nasal bone complex is thickest at its caudal border and thinner cephalically. 2. Paired nasal cartilages include the upper and lower laterals - The upper lateral/triangular cartilages articulate with the caudal edge of the nasal bones and with the septum medially. → Their integrity is partly responsible for the patency of the internal nasal valve. - The lower lateral/alar cartilage is responsible for the size and shape of the nasal tip. 3. The soft tissue envelope of the nose is loosely attached to the cartilaginous and bony scaffold. All arterial, venous, and nervous structures lie in the superficial plane. Anatomy The nasal septum has cartilaginous and bony components. -

Chapter 7: the Axial Skeleton
Chapter 7: The Axial Skeleton I. The Axial Division of the Skeletal System, p. 206 Objective 1. Identify the bones of the axial skeleton and their functions. • In studying individual bones, we are concerned with their functions, including which bones they connect or articulate with, and their structures and marks, including muscle and ligament attachments, and openings for nerves and blood vessels (foramina). Figure 7-1 • The axial skeleton: - forms the longitudinal axis of the body - has 80 bones • The axial skeleton includes: - the skull (8 cranial bones and 14 facial bones) - bones associated with the skull (6 auditory ossicles and the hyoid bone) - the vertebral column (24 vertebrae, the sacrum and the coccyx) - the thoracic cage (24 ribs and the sternum) • Functions of the axial skeleton include: - support and protect organs in the body cavities - attach to muscles that support head, neck and trunk - attach to breathing muscles - attach to muscles of the appendicular skeleton • Axial bones are strong, with many ligaments, but are restricted in motion. II. The Skull, p. 206 Objectives 1. Identify the bones of the cranium and face, and the significance of their markings. 2. Describe the structures and functions of the nasal complex. 3. Explain the functions of paranasal sinuses. 4. Describe the differences between the skulls of infants, children and adults. • The skull protects the brain and entrances to respiratory and digestive systems. Figure 7-2 • The skull has 22 bones: - 8 cranial bones form the braincase or cranium. The cranial bones enclose the cranial cavity, which contains the brain and associated fluids, blood vessels, nerves and membranes. -

Axis Scientific 22-Part Osteopathic Natural Bone Human Skull A-105940
Axis Scientific 22-Part Osteopathic Natural Bone Human Skull A-105940 Frontal Bone Nasal Bone Nasal Bone (Right) (Left) Frontal Bone Ethmoid Bone Parietal Bone Parietal Bone (Right) (Left) Parietal Bone Lacrimal (Right) Bone (Right) Temporal Bone Nasal Bone Temporal Bone (Left) (Right) (Right) Sphenoid Bone Lacrimal Bone (Right) Lacrimal Bone (Left) R L Zygomatic Bone Zygomatic Bone (Right) (Left) Maxilla & Teeth Maxilla & Teeth (Right Side) (Left Side) Inferior Nasal Sphenoid Bone Inferior Nasal Concha (Left) Concha (Right) Occipital Bone Temporal Bone Zygomatic Bone (Right) (Right) Maxilla & Teeth Mandible & Mandible & (Right Side) Vomer Teeth Teeth Anterior View Lateral View Parietal Bone Parietal Bone (Right) (Left) Maxilla & Teeth Maxilla & Teeth (Right Side) (Left Side) Palatine Palatine Bone (Right) Bone (Left) Zygomatic Zygomatic Bone (Left) Bone (Right) Sphenoid Bone R L L R Vomer Temporal Bone Temporal Bone Temporal Bone (Right) (Left) (Right) Temporal Bone (Left) Parietal Bone Parietal Bone (Left) (Right) Occipital Bone Occipital Bone Mandible & Teeth Inferior View Posterior View Parietal Bone Frontal Bone Parietal Bone (Right) (Left) Parietal Bone Parietal Bone (Right) (Left) Temporal Temporal Bone (Right) Bone (Left) Temporal Bone Temporal Bone (Right) (Left) A Frontal Bone R L C B Sphenoid Sphenoid Sphenoid Bone Bone Bone Occipital Bone D E F Zygomatic Bone (Right) Zygomatic G Bone (Left) Lacrimal Bone (Right) Mandible & Maxilla & Teeth Maxilla & Teeth Maxilla & Teeth Teeth (Right Side) (Left Side) Maxilla & Teeth (Left Side) -

Pharynx, Larynx, Nasal Cavity and Pterygopalatine Fossa
Pharynx, Larynx, Nasal cavity And Pterygopalatine Fossa Mikel H. Snow, Ph.D. Dental Anatomy [email protected] July 29, 2018 Pharynx Food & Air Passage Pharynx The pharynx is a skeletal muscle tube that opens anteriorly with 3 regions. The upper part communicates with nasal cavity, the middle communicates with oral cavity, and the lower communicates with the larynx. Nasal cavity Nasal Oral cavity cavity Larynx Air Nasopharynx: between Oral sphenoid sinus & uvula Food/ cavity Oropharynx: between uvula & epiglottis drink Laryngopharynx: between epiglottis & esophagus Esophagus Trachea The posterior and lateral walls are 3 skeletal muscles (constrictors) that propel food/liquid inferiorly to the esophagus. Constrictors innervated by CNX. Additional muscles elevate the pharynx (stylopharyngeus is external). Stylopharyngeus innervated by CNIX. Stylopharyngeus Superior constrictor Middle constrictor Inferior constrictor Two additional internal muscles we’ll get to later… Key relationship: Glossopharyngeal nerve wraps around stylopharyngeus muscle. CN IX wraps around stylopharyngeus muscle and Stylopharyngeus innervates it. Pharyngeal constrictors Pharynx Interior 1 Nasopharynx: 1. Pharyngeal tonsils 2. Auditory tube ostia 2 3 3. Salpingopharyngeal fold 4 4 Oropharynx: 4. Palatine tonsils 5 5 Laryngopharynx: Slit open 5. Piriform recess constrictors to examine interior Lateral Wall of Pharynx 5. Salpingopharyngeus muscle 6. Levator veli palatini muscle 1. Pharyngeal tonsils 7. Tensor veli palatini muscle 2. Torus tubarius 8. Palatine tonsil 3.