Optimization of a Microfluidics-Based Next Generation Sequencing Assay for Clinical Oncology Diagnostics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Recent Advances in Droplet-Based Microfluidic Technologies
micromachines Review Recent Advances in Droplet-based Microfluidic Technologies for Biochemistry and Molecular Biology 1, 1, 2, Joel Sánchez Barea y , Juhwa Lee y and Dong-Ku Kang * 1 Department of Chemistry, Incheon National University, Incheon 22012, Korea; [email protected] (J.S.B.); [email protected] (J.L.) 2 Department of Chemistry, Research Institute of Basic Sciences, Incheon National University, Incheon 22012, Korea * Correspondence: [email protected]; Tel.: +82-32-835-8094 These authors contribute equally to this article. y Received: 2 May 2019; Accepted: 18 June 2019; Published: 20 June 2019 Abstract: Recently, droplet-based microfluidic systems have been widely used in various biochemical and molecular biological assays. Since this platform technique allows manipulation of large amounts of data and also provides absolute accuracy in comparison to conventional bioanalytical approaches, over the last decade a range of basic biochemical and molecular biological operations have been transferred to drop-based microfluidic formats. In this review, we introduce recent advances and examples of droplet-based microfluidic techniques that have been applied in biochemistry and molecular biology research including genomics, proteomics and cellomics. Their advantages and weaknesses in various applications are also comprehensively discussed here. The purpose of this review is to provide a new point of view and current status in droplet-based microfluidics to biochemists and molecular biologists. We hope that this review will accelerate communications between researchers who are working in droplet-based microfluidics, biochemistry and molecular biology. Keywords: droplet-based microfluidic; biochemistry; molecular biology; digital PCR; biochip; biosensor; digital quantification; microfluidic; single cell analysis 1. -

Interfacing to Biological Systems Using Microfluidics
University of Tennessee, Knoxville TRACE: Tennessee Research and Creative Exchange Doctoral Dissertations Graduate School 12-2018 Interfacing to Biological Systems Using Microfluidics Peter Golden Shankles University of Tennessee, [email protected] Follow this and additional works at: https://trace.tennessee.edu/utk_graddiss Recommended Citation Shankles, Peter Golden, "Interfacing to Biological Systems Using Microfluidics. " PhD diss., University of Tennessee, 2018. https://trace.tennessee.edu/utk_graddiss/5315 This Dissertation is brought to you for free and open access by the Graduate School at TRACE: Tennessee Research and Creative Exchange. It has been accepted for inclusion in Doctoral Dissertations by an authorized administrator of TRACE: Tennessee Research and Creative Exchange. For more information, please contact [email protected]. To the Graduate Council: I am submitting herewith a dissertation written by Peter Golden Shankles entitled "Interfacing to Biological Systems Using Microfluidics." I have examined the final electronic copy of this dissertation for form and content and recommend that it be accepted in partial fulfillment of the requirements for the degree of Doctor of Philosophy, with a major in Energy Science and Engineering. Scott T. Retterer, Major Professor We have read this dissertation and recommend its acceptance: Steven M. Abel, Mitchel J. Doctycz, Jennifer L. Morrell-Falvey Accepted for the Council: Dixie L. Thompson Vice Provost and Dean of the Graduate School (Original signatures are on file with official studentecor r ds.) Interfacing to Biological Systems Using Microfluidics A Dissertation Presented for the Doctor of Philosophy Degree The University of Tennessee, Knoxville Peter Golden Shankles December 2018 Copyright © 2018 by Peter Golden Shankles All rights reserved. -

A Flexible Microfluidic System for Single-Cell Transcriptome Profiling
www.nature.com/scientificreports OPEN A fexible microfuidic system for single‑cell transcriptome profling elucidates phased transcriptional regulators of cell cycle Karen Davey1,7, Daniel Wong2,7, Filip Konopacki2, Eugene Kwa1, Tony Ly3, Heike Fiegler2 & Christopher R. Sibley 1,4,5,6* Single cell transcriptome profling has emerged as a breakthrough technology for the high‑resolution understanding of complex cellular systems. Here we report a fexible, cost‑efective and user‑ friendly droplet‑based microfuidics system, called the Nadia Instrument, that can allow 3′ mRNA capture of ~ 50,000 single cells or individual nuclei in a single run. The precise pressure‑based system demonstrates highly reproducible droplet size, low doublet rates and high mRNA capture efciencies that compare favorably in the feld. Moreover, when combined with the Nadia Innovate, the system can be transformed into an adaptable setup that enables use of diferent bufers and barcoded bead confgurations to facilitate diverse applications. Finally, by 3′ mRNA profling asynchronous human and mouse cells at diferent phases of the cell cycle, we demonstrate the system’s ability to readily distinguish distinct cell populations and infer underlying transcriptional regulatory networks. Notably this provided supportive evidence for multiple transcription factors that had little or no known link to the cell cycle (e.g. DRAP1, ZKSCAN1 and CEBPZ). In summary, the Nadia platform represents a promising and fexible technology for future transcriptomic studies, and other related applications, at cell resolution. Single cell transcriptome profling has recently emerged as a breakthrough technology for understanding how cellular heterogeneity contributes to complex biological systems. Indeed, cultured cells, microorganisms, biopsies, blood and other tissues can be rapidly profled for quantifcation of gene expression at cell resolution. -

RNA-Seq and Microfluidic Digital PCR Identification of Transcriptionally Active Spirochetes in Termite Gut Microbial Communities
4-1 RNA-Seq and microfluidic digital PCR identification of transcriptionally active spirochetes in termite gut microbial communities Abstract CO2-reductive acetogenesis in termite hindguts is a bacterial process with significant impact on the nutrition of wood-feeding termites. Acetogenic spirochetes have been identified as key mediators of acetogenesis. Here, we use high-throughput, short transcript sequencing (RNA-Seq) and microfluidic, multiplex digital PCR to identify uncultured termite gut spirochetes transcribing genes for hydrogenase-linked formate dehydrogenase (FDHH) enzymes, which are required for acetogenic metabolism in the spirochete, Treponema primitia. To assess FDHH gene (fdhF) transcription within the gut community of a wood-feeding termite, we sequenced ca. 28,000,000 short transcript reads of gut microbial community RNA using Illumina Solexa technology. RNA-Seq results indicate that fdhF transcription in the gut is dominated by two fdhF genotypes: ZnD2sec and Zn2cys. This finding was independently corroborated with cDNA inventory and qRT-PCR transcription measurements. We, therefore, propose that RNA-Seq mapping of microbial community transcripts is specific and quantitative. Following transcriptional assessments, we performed microfluidic, multiplex digital PCR on single termite gut bacterial cells to discover the identity of uncultured bacteria encoding fdhF 4-2 genotypes ZnD2sec and Zn2cys. We identified the specific 16S rRNA gene ribotype of the bacterium encoding Zn2cys fdhF and report that the bacterium is a spirochete. Phylogenetic analysis reveals that this uncultured spirochete, like T. primitia, possesses genes for acetogenic metabolism – formyl-tetra-hydrofolate synthetase and both selenocysteine and cysteine variants of formate dehydrogenase. Microfluidic results also imply a spirochetal origin for ZnD2sec fdhF, but further gene pair associations are required for verification. -

Microbes and Metagenomics in Human Health an Overview of Recent Publications Featuring Illumina® Technology TABLE of CONTENTS
Microbes and Metagenomics in Human Health An overview of recent publications featuring Illumina® technology TABLE OF CONTENTS 4 Introduction 5 Human Microbiome Gut Microbiome Gut Microbiome and Disease Inflammatory Bowel Disease (IBD) Metabolic Diseases: Diabetes and Obesity Obesity Oral Microbiome Other Human Biomes 25 Viromes and Human Health Viral Populations Viral Zoonotic Reservoirs DNA Viruses RNA Viruses Human Viral Pathogens Phages Virus Vaccine Development 44 Microbial Pathogenesis Important Microorganisms in Human Health Antimicrobial Resistance Bacterial Vaccines 54 Microbial Populations Amplicon Sequencing 16S: Ribosomal RNA Metagenome Sequencing: Whole-Genome Shotgun Metagenomics Eukaryotes Single-Cell Sequencing (SCS) Plasmidome Transcriptome Sequencing 63 Glossary of Terms 64 Bibliography This document highlights recent publications that demonstrate the use of Illumina technologies in immunology research. To learn more about the platforms and assays cited, visit www.illumina.com. An overview of recent publications featuring Illumina technology 3 INTRODUCTION The study of microbes in human health traditionally focused on identifying and 1. Roca I., Akova M., Baquero F., Carlet J., treating pathogens in patients, usually with antibiotics. The rise of antibiotic Cavaleri M., et al. (2015) The global threat of resistance and an increasingly dense—and mobile—global population is forcing a antimicrobial resistance: science for interven- tion. New Microbes New Infect 6: 22-29 1, 2, 3 change in that paradigm. Improvements in high-throughput sequencing, also 2. Shallcross L. J., Howard S. J., Fowler T. and called next-generation sequencing (NGS), allow a holistic approach to managing Davies S. C. (2015) Tackling the threat of anti- microbial resistance: from policy to sustainable microbes in human health. -
Microfluidics Coupled Mass Spectrometry for Multi- Omics/Targeted Assays in Translational Research
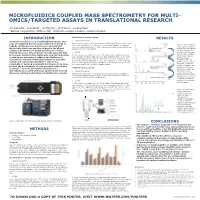
MICROFLUIDICS COUPLED MASS SPECTROMETRY FOR MULTI- OMICS/TARGETED ASSAYS IN TRANSLATIONAL RESEARCH PD Rainville1, G Astarita1, JP Murphy1, ID Wilson2, JI Langridge1 1Waters Corporation, Milford, MA; 2Imperial College, London, United Kingdom INTRODUCTION Lipidomics of human plasma RESULTS Translation medicine is an interdisciplinary science that Sample Preparation Human plasma samples were prepared by modified Bligh-Dyer extraction with aims at combining the information taken from bench to Figure 4. BPI of multiple- bedside. In this process molecules are isolated and chloroform : methanol (2:1) with a (4:1) with human plasma. The samples were then centrifuged at 13,000 RCF for 5 min, dried down, reconstituted and omics experiments from identified in discovery and then utilized in the clinical injected onto the LC-MS system. human urine and plasma setting as biomarkers of health and disease to better run consecutively. The develop therapies. It has become recently apparent that LC-MS profiling of biofluids was carried out in repetitive proteomics, metabolomics, lipidomics, and glycomics data A 1 µL injection was made onto the LC-MS system. The sample was eluted order of polar plasma under gradient conditions with aqueous formic acid/acetonitrile (40/60) and combined are necessary to address the challenge of profiling, plasma acetonitrile/isopropanol (10/90) at a flow rate of 3 µL/min. Separation was translational research which places strain on available lipidomics, and urine carried out on an iKey CSH C18 100 Å, 1.7µm, 150 µm x 100 mm controlled 1-4 profiling over a period of sample and instrument utilization . Due to the at 60 °C. -

Microfluidics Brochure
Microfluidics Comprehensive Microfluidics Solutions for Diagnostics and Life Science Research You r i d e a s . We make them flow. INSIGHT INTO YOUR APPLICATIONS As the world of life science becomes increasingly complex, developers are challenged to build solutions that enable more analysis on smaller samples with easier user workflows. Whether you’re creating instruments for life science research or diagnostics, there’s a likelihood your application will require microfluidics. Our experts enable microfluidics that simplify workflows for assays in a wide range of applications, and we partner with you to develop intricate technology while streamlining functionality, manufacturability, and costs. ASSAYS ENABLED BY MICROFLUIDICS As the global authority in optofluidic subsystems we are proud to be one of the few OEM suppliers with a demonstrated capability to make complex assays work on microfluidic cartridges. From functionalized flow cells and droplet generators for next generation sequencing, to complex sample-to-answer solutions for point-of-care or in-field testing, we are a recognized leader in miniaturizing of an entire laboratory setup into a single device — with on-card reagents, pumps, valves, sensors, and optical interfaces. 2 Applications ORGAN- ON-A-CHIP DEVICES MULTIPLEXED MOLECULAR ASSAY DROPLET- BASED APPLICATIONS NEXT GENERATION CELL SEQUENCING ISOLATION DIAGNOSTICS AND POINT OF CARE MOLECULAR ENRICHMENT WORKFLOWS LIQUID BIOPSY 3 OPTOFLUIDIC PATHWAY Capabilities WE WELCOME THE MOST AMBITIOUS PROJECTS Microfluidic development projects require highly sophisticated technologies and sensitive materials to provide optimized and reliable performance. Although microfluidic consumable devices are undeniably complex, our experts make it easier to develop the right tools for your application. -

Throughput Screening in C. Elegans Using
AUTOMATED QUANTITATIVE PHENOTYPING AND HIGH- THROUGHPUT SCREENING IN C. ELEGANS USING MICROFLUIDICS AND COMPUTER VISION A Dissertation Presented to The Academic Faculty by Matthew Muria Crane In Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the School of Bioengineering Georgia Institute of Technology August 2011 AUTOMATED QUANTITATIVE PHENOTYPING AND HIGH- THROUGHPUT SCREENING IN C. ELEGANS USING MICROFLUIDICS AND COMPUTER VISION Approved by: Dr. Hang Lu, Advisor Dr. Michelle LaPlaca School of Chemical and Biomolecular Engineering School of Biomedical Engineering Georgia Institute of Technology Georgia Institute of Technology Dr. Robert Butera Dr. James Rehg School of Electrical and Computer Engineering School of Interactive Computing Georgia Institute of Technology Georgia Institute of Technology Dr. Oliver Brand School of Electrical and Computer Engineering Georgia Institute of Technology Date Approved: March 10, 2011 To my AsianCajun ACKNOWLEDGEMENTS I wish to thank my labmates for making this process interesting, educational and above all, entertaining. I’d like especially to thank Jeffrey Stirman and Kwanghun Chung for teaming up with me (or allowing me to team up with you), and for the years of coffee breaks and discussions. Ed Park for hours of political distraction and fierce debate. My advisor, Hang Lu, for providing me with all of the feedback and support a graduate student could ask for, while letting me explore this research topic with abandon. Thank you for helping me learn how to research, not just do research. My committee for providing me with valuable feedback and advance to improve this work. My family for supporting and encouraging me and helping to keep me from losing myself in the process. -

Single-Cell Genomics
Single-Cell Genomics Exploring new applications in microfluidics Mark Lynch April 10, 2019 Agenda 1. Microfluidics solutions for single-cell analysis 2. Single-cell total RNA sequencing 3. Single-cell high-throughput (HT) RNA expression and protein sequencing (REAP-seq) 4. Creating single-cell microenvironments 2 Microfluidic solutions for single-cell analysis Cellular analysis cell by cell The single-cell revolution is only beginning Science special issue, A Fantastic Voyage in Science, 2018 Breakthrough of the Year, Genomics, 2017 published in December 4 Driving those advances are techniques for isolating thousands of intact cells from living organisms, efficiently sequencing expressed genetic material in each cell and using computers, or labeling the cells, to reconstruct their relationships in space and time. That technical trifecta ‘will transform the next decade of research,’ says Nikolaus Rajewsky, a systems biologist at the Max Delbrück Center for Molecular Medicine in Berlin. —Elizabeth Pennisi, writing in ‘Science’ about the 2018 Breakthrough of the Year 5 Creating a cell atlas The only way to identify and understand all cells in a tissue Three cell-based approaches: 1. Classification 2. Characterization 3. Context 6 The benefit Individual cells behave differently from the average of many cells Modified from Dominguez et al. Journal of Immunological Methods (2014) 7 Cell characterization Deep profiling of cells to study multiple modes Stuart and Satija. Nature Reviews Genetics (2019) 8 Microfluidics Integrated fluidic circuit -

Research Training of Undergraduates Through Biomems Senior Design Projects
AC 2008-1221: RESEARCH TRAINING OF UNDERGRADUATES THROUGH BIOMEMS SENIOR DESIGN PROJECTS Jin-Hwan Lee, University of Cincinnati Jin-Hwan Lee earned his M.S. and B.S in Material Science Engineering at the Korea University, Seoul, South Korea. He is currently a PhD candidate in the Department of Electrical and Computer Engineering at the University of Cincinnati. He was awarded the Rindsberg Fellowship in 2005 and again in 2006, and has participated in the Preparing Future Faculty program. His research interests include biosensors and microfluidic biochips for environmental and medical applications. Ali Asgar Bhagat, University of Cincinnati Ali Asgar S. Bhagat earned his M.S. in electrical engineering from the University of Cincinnati in 2006, and is currently a Ph.D. candidate in the Department of Electrical and Computer Engineering. His research interests include microfluidics and MEMS devices for chemical and biological assays. He was the teaching assistant for the microfluidics laboratory course discussed in this paper. Karen Davis, University of Cincinnati Dr. Karen C. Davis is an Associate Professor of Electrical & Computer Engineering at the University of Cincinnati. She has advised over 30 senior design students and more than 20 MS/PhD theses in the area of database systems. She has been the recipient of several departmental and college teaching awards, including the Master of Engineering Education Award, the Dean’s Award for Innovation in Engineering Education, and the Wandamacher Teaching Award for Young Faculty. She is a Senior member of IEEE and an ABET Computer Engineering program evaluator. Dr. Davis received a B.S. degree in Computer Science from Loyola University, New Orleans in 1985 and an M.S. -

Microfluidic Single-Cell Whole-Transcriptome Sequencing
Microfluidic single-cell whole-transcriptome sequencing Aaron M. Streetsa,b,1, Xiannian Zhanga,b,1, Chen Caoa,c, Yuhong Panga,c, Xinglong Wua,c, Liang Xionga,c, Lu Yanga,c, Yusi Fua,c, Liang Zhaoa,b,2,3, Fuchou Tanga,c,3, and Yanyi Huanga,b,3 aBiodynamic Optical Imaging Center (BIOPIC), bCollege of Engineering, and cSchool of Life Sciences, Peking University, Beijing 100871, China Edited by Stephen R. Quake, Stanford University, Stanford, CA, and approved April 2, 2014 (received for review February 3, 2014) Single-cell whole-transcriptome analysis is a powerful tool for and has undergone successive improvements since its inception quantifying gene expression heterogeneity in populations of cells. (22, 23), including a recent demonstration of absolute mRNA Many techniques have, thus, been recently developed to perform counting (24). One limitation that remains among most current transcriptome sequencing (RNA-Seq) on individual cells. To probe single-cell RNA-Seq methods, however, is sensitivity. Efficient and subtle biological variation between samples with limiting amounts reproducible reverse transcription and cDNA amplification are of RNA, more precise and sensitive methods are still required. We difficult with the extremely low quantity of total RNA in a single adapted a previously developed strategy for single-cell RNA-Seq cell (around 10 pg in a typical mammalian cell) (11), and insufficient that has shown promise for superior sensitivity and implemented reverse transcription efficiency and bias to highly expressed genes the chemistry in a microfluidic platform for single-cell whole- during amplification impede accurate quantification of low-abun- transcriptome analysis. In this approach, single cells are captured dance transcripts (25). -

Droplet Microfluidics for Synthetic Biology
Lawrence Berkeley National Laboratory Recent Work Title Droplet microfluidics for synthetic biology. Permalink https://escholarship.org/uc/item/6cr3k0v5 Journal Lab on a chip, 17(20) ISSN 1473-0197 Authors Gach, Philip C Iwai, Kosuke Kim, Peter W et al. Publication Date 2017-10-01 DOI 10.1039/c7lc00576h Peer reviewed eScholarship.org Powered by the California Digital Library University of California Lab on a Chip View Article Online CRITICAL REVIEW View Journal | View Issue Droplet microfluidics for synthetic biology Cite this: Lab Chip,2017,17,3388 Philip C. Gach,*ab Kosuke Iwai,ab Peter W. Kim,ab Nathan J. Hillsonacde and Anup K. Singh *ab Synthetic biology is an interdisciplinary field that aims to engineer biological systems for useful purposes. Organism engineering often requires the optimization of individual genes and/or entire biological pathways (consisting of multiple genes). Advances in DNA sequencing and synthesis have recently begun to enable the possibility of evaluating thousands of gene variants and hundreds of thousands of gene combinations. However, such large-scale optimization experiments remain cost-prohibitive to researchers following tradi- tional molecular biology practices, which are frequently labor-intensive and suffer from poor reproducibil- ity. Liquid handling robotics may reduce labor and improve reproducibility, but are themselves expensive Received 30th May 2017, and thus inaccessible to most researchers. Microfluidic platforms offer a lower entry price point alternative Accepted 9th August 2017 to robotics, and maintain high throughput and reproducibility while further reducing operating costs through diminished reagent volume requirements. Droplet microfluidics have shown exceptional promise DOI: 10.1039/c7lc00576h for synthetic biology experiments, including DNA assembly, transformation/transfection, culturing, cell rsc.li/loc sorting, phenotypic assays, artificial cells and genetic circuits.