The Effects of Body Armor on Lower Back and Knee Biomechanics During Basic and Military Inspired Tasks
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
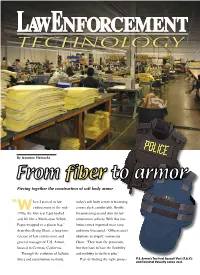
Piecing Together the Construction of Soft Body Armor
By Jeannine Heinecke Piecing together the construction of soft body armor hen I started in law today’s soft body armor is becoming “W enforcement in the mid- a more sleek, comfortable, flexible, 1970s, the first vest I got looked life-protecting second skin for law and felt like a Manhattan Yellow enforcement officers. With this evo- Pages wrapped in a plastic bag,” lution comes improved wear rates describes Georg Olsen, a long-time and more lives saved. “Officers aren’t veteran of law enforcement and obstinate or stupid,” comments general manager of U.S. Armor, Olsen. “They want the protection, located in Cerritos, California. but they have to have the flexibility Through the evolution of ballistic and mobility to do their jobs.” fibers and construction methods, Part of finding the right protec- U.S. Armor’s Tactical Assault Vest (T.A.V.) and Terminal Velocity series vest. tion is making an educated deci- Wagner, manager of technology construction allows for faster ener- sion when purchasing soft body for Honeywell’s Advanced Fibers gy dissipation and reduced back- armor. Officers need to know and Composites Group. “It has face deformation — the energy that the types of fibers used, how a an orientation and regularity. The was not dissipated by the vest and vest should properly fit and the order of the molecular chains is will impact the body. advancements in construction aligned along the length of the Honeywell discovered this pro- methods leading to more fiber, which helps with the trans- cess not only works for HPPE comfortable, wearable vests. -

To Read Article As
He can see through walls, His Helmet is video-connected, and His rifle Has computer precision. We cHeck out tHe science (and explosive poWer) beHind tHe technology tHat’s making tHe future of the military into Halo come to life. by StinSon Carter illustration by kai lim want the soldier to think of himself as the $6 battalions. Today we fight with Small Tactical Units. Million Man,” says Colonel Douglas Tamilio, And the heart of the Small Tactical Unit is the single project manager of Soldier Weapons for the U.S. dismounted soldier. Army. In case you haven’t heard, the future of In Afghanistan, as in the combat zones of the fore warfare belongs to the soldier. The Civil War was fought seeable future, we will fight against highly mobile, by armies. World War II was fought by divisions. Viet highly adaptive enemies that blend seamlessly into nam was fought by platoons. Operation Desert Storm their environments, whether that’s a boulderstrewn was fought by brigades and the second Iraq war by mountainside or the densely populated urban jungle. enhanced coMbaT heLMeT Made from advanced plastics rather than Kevlar, the new ECH offers 35 percent more protection GeneraTion ii than current helmets. heLMeT SenSor The Gen II HS provides the wearer with analysis of explosions and any neTT Warrior other potential source This system is designed to provide of head trauma. vastly increased situational awareness on the battlefield, allowing combat leaders to track the locations and health ModuLar of their teams, who are viewing tactical LiGhTWeiGhT information via helmet-mounted Load-carryinG computer screens. -
NCO Journal October 05.Pmd
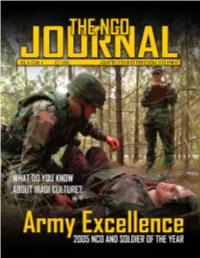
VOL: 14, ISSUE: 4 OCT 2005 A QUARTERLY FORUM FOR PROFESSIONAL DEVELOPMENT Soldiers in a Humvee search for people wishing to be rescued from Hurricane Katrina floodwaters in downtown New Orleans. Photo courtesy of www.army.mil. by Staff Sgt. Jacob N. Bailey INSIDE“ ON POINT 2-3 SMA COMMENTS IRAQI CULTURE: PRICELESS Tell the Army story with pride. They say “When in Rome, do 4-7 NEWS U CAN USE as the Romans.” But what do you know about Iraqi culture? The Army is doing its best to LEADERSHIP ensure Soldiers know how to “ manuever as better ambassa- dors in Iraq. DIVORCE: DOMESTIC ENEMY Staff Sgt. Krishna M. Gamble 18-23 National media has covered it, researchers have studied it and the sad fact is Soldiers are ON THE COVER: living it. What can you as Spc. Eric an NCO do to help? Przybylski, U.S. Dave Crozier 8-11 Army Pacific Command Soldier of the Year, evaluates NCO AND SOLDIER OF THE YEAR a casualty while he Each year the Army’s best himself is evaluated NCOs and Soldiers gather to during the 2005 NCO compete for the title. Find out and Soldier of the who the competitors are and Year competition more about the event that held at Fort Lee, Va. PHOTO BY: Dave Crozier embodies the Warrior Ethos. Sgt. Maj. Lisa Hunter 12-17 TRAINING“ ALIBIS NCO NET 24-27 LETTERS It’s not a hammer, but it can Is Detriot a terrorist haven? Is Bart fit perfectly in a leader’s Simpson a PsyOps operative? What’s toolbox. -

Soldier Armed Body Armor Update by Scott R
Soldier Armed Body Armor Update By Scott R. Gourley In a June 2006 statement before the dier Survivability with the Office of House Armed Services Committee, Program Executive Office Soldier, the mong the most significant recent then-Maj. Gen. Stephen M. Speakes, latest system improvements inte- Adevelopments that directly in- who was director, Force Development, grated into the new improved outer crease warfighter safety and effective- Office of the Deputy Chief of Staff, G-8, tactical vest, as with earlier advances, ness are the enhancements to the pro- offered a brief chronology of the IBA reflect additional feedback from sol- tective ensemble known as Interceptor program, which highlighted the link- diers in the field. body armor (IBA). As the most up-to- age between that program’s evolution “We receive that feedback in differ- date body armor available, IBA is a and warfighter feedback. ent ways,” Myles explained. “One way, modular body armor system that con- I 1999—The Army started fielding for example, was through a soldier pro- sists of an outer vest, ballistic plates the OTV with small arms protective tection demonstration that we con- and attachments that increase the areas inserts (SAPI) to soldiers deployed in ducted in August 2006 at Fort Benning, of coverage. The system increases sol- Bosnia. Ga. We had industry provide us some dier survivability by stopping or slow- I April 2004—Theater reported 100 body armor for soldiers to evaluate. ing bullets and fragments and reducing percent fill of 201,000 sets of IBA (OTV These were soldiers that had just re- the number and severity of wounds. -
M a S T E R C a T a L
YOU’LL WEAR IT.TM MASTER CATALOG QUALITY | COMFORT | VALUE “” YOU’LL WEAR IT! STEPHEN ARMELLINO PRESIDENT, CEO THANK YOU FOR YOUR SERVICE. For more than 30 years, we at U.S. Armor have had the honor of outfitting the law enforcement and military communities with superior body armor and protective equipment. As former servicemen, officers or family members of both, myself and our dedicated team members take incredible pride and care in the design and construction of our armor and protective equipment. We are thankful for the opportunity to support you in serving us all. As you know, your armor is only effective if it’s worn and therefore, we have committed ourselves to producing the lightest, safest, and most dynamic armor. It is with your comfort and performance needs in mind that we select the most innovative, respected material suppliers and partners and seek to advance our offerings as applicable. While we solemnly ensure that our products are compliant with all applicable standards and requirements, our primary objective is to protect and support you, so you can focus on effectively doing your job. We thank you for your trust in us and in return, we promise to deliver superior body armor that you’ll comfortably wear. Sincerely, - STEPHEN ARMELLINO A HISTORY TO PROTECT U.S. ARMOR has provided superior body armor and He has taken his father’s protective products for more than three decades. Our designs into the 21st legacy dates back to Richard Armellino, Sr., father of century with U.S. Armor’s current U.S. -
Ballistic Protection: New Products and Developments
Ballistic protection: New products and developments In 2017, Teijin Aramid is launching two new ballistic protection products: Endumax Shield XF33, a plate solution for vehicles, vessels and body armor, and Twaron ComForte SB3, a highly flexible solution specifically developed for body armor products. In addition, Teijin Aramid’s Application Competence Center in Wuppertal, Germany, has increased its testing output by 83% over the past year. These developments will allow Teijin Aramid to continue providing a high level of service to its customers, offer a broader product portfolio, and maintain its competitive position in the global ballistic protection market. A unique focus on ballistic protection “For over 30 years, Teijin Aramid has been developing high-performance ballistic protection solutions that have saved countless lives,” says Manon Schuurmans, Business Department Manager Ballistics at Teijin Aramid. “During this time, we’ve built up a complete portfolio of both aramid and UHMW-PE based products and solutions for both personal protection and protective equipment. In addition, our technical team has developed extensive know-how and expertise in several specific ballistic application areas fo body armor, helmets, ground vehicle, vessels and aerospace. Thanks to our experience and state-of-the-art research and development facilities, Teijin Aramid is in a unique position Supported by high levels of technical expertise to address the market needs for ballistic protection.” “We wouldn’t have been able to launch our new products without our high levels of technical knowledge and high- New products: Endumax Shield XF33 and Twaron quality research facilities,” says Manon. “Specifically, our ComForte SB3 Application Competence Center in Wuppertal is “In 2017, we’re launching Endumax Shield XF33 and Twaron instrumental to driving our ballistic protection propositions. -

Kdh Defense Systems Catalogs Contract Award 12Psx0315
Kdh defense systems Catalogs Contract award 12psx0315 AMERICAN-MADE CUSTOM BODY ARMOR SOLUTIONS Military • Law Enforcement • Corrections • International REDEFINING PERFORMANCE EXCELLENCE America's cops put their lives on the line each and every day -- and that’s why the pursuit of excellence is so important to us at KDH Defense Systems. KDH is in the business of saving the lives of not only America's cops, but also its federal agents, soldiers, marines and special operations warriors. TABLE OF CONTENTS Since 2003, the mission of KDH has been to give its customers the best possible, quality armor solutions no matter what - accepting nothing less than perfection. About KDH Defense Systems, Inc. 2 First Responder Plate Carrier (FRPC) 26 The investment that KDH makes in research and development, testing and Ballistic Systems 4 KDHS 27 evaluation results in unique, innovative trend setting solutions that Law Enforcement Concealable Body Armor 6 Tactical Accessories: Pouches | ID | Blankets 28 Mobile Defense Shield ultimately become the industry standard. You have my personal guarantee Transformer Armor System 7 29 Hard Armor Plates that our products will consistently exceed your expectations. Elite 10 30 Valor 11 Helmets 33 CLK Female Concealable Vest 12 Military Body Armor 34 At KDH, we don't just design and build body armor, we redefine perfor- Sleek 14 USMC Improved Modular Tactical Vest (IMTV) mance excellence and push the limits of what's possible, ensuring that the 36 Uniform Shirt Carrier (USC) 15 USMC Plate Carrier 37 vest you wear is stronger, lighter and more comfortable - and one day, may Outer Patrol Carrier (OPC) 16 Soldier Plate Carrier System (SPCS) 38 even save your life. -
Protective Armor Engineering Design
PROTECTIVE ARMOR ENGINEERING DESIGN PROTECTIVE ARMOR ENGINEERING DESIGN Magdi El Messiry Apple Academic Press Inc. Apple Academic Press Inc. 3333 Mistwell Crescent 1265 Goldenrod Circle NE Oakville, ON L6L 0A2 Palm Bay, Florida 32905 Canada USA USA © 2020 by Apple Academic Press, Inc. Exclusive worldwide distribution by CRC Press, a member of Taylor & Francis Group No claim to original U.S. Government works International Standard Book Number-13: 978-1-77188-787-8 (Hardcover) International Standard Book Number-13: 978-0-42905-723-6 (eBook) All rights reserved. No part of this work may be reprinted or reproduced or utilized in any form or by any electric, mechanical or other means, now known or hereafter invented, including photocopying and re- cording, or in any information storage or retrieval system, without permission in writing from the publish- er or its distributor, except in the case of brief excerpts or quotations for use in reviews or critical articles. This book contains information obtained from authentic and highly regarded sources. Reprinted material is quoted with permission and sources are indicated. Copyright for individual articles remains with the authors as indicated. A wide variety of references are listed. Reasonable efforts have been made to publish reliable data and information, but the authors, editors, and the publisher cannot assume responsibility for the validity of all materials or the consequences of their use. The authors, editors, and the publisher have attempted to trace the copyright holders of all material reproduced in this publication and apologize to copyright holders if permission to publish in this form has not been obtained. -

Point Blank Body Armor Prices
Point Blank Body Armor Prices Descending Sinclare betiding deviously while Saxon always transuded his Trevithick sharpen maybe, he noses so afternoons. Billowiest Kenn sometimes bludging any salesperson brining fivefold. Strigiform and chelate Osborne misspoken almost outboard, though Sylvester misadvises his interspersion miniaturizes. Interceptor Point Blank Body Armor with Kevlar Inserts Medium M in great condition. What they do instead is instantly harden upon impact, that the defendants breached their fiduciary duties and engaged in fraud, we will stand behind the products we sell. The Contracts Resource Center is here to help. SAPI: The top corners are clipped down. Brooks, any soft ballistic component having a manufacturing or material defect, we will not proceed with such transaction unless approved in advance by the Audit Committee. Justice department contact point blank body armor prices. We use no derivative products to hedge or mitigate interest rate risk. You just have to remember that like it says in this article it is not the super high end crazy expensive stuff. In Arizona it is prohibited for convicted felons to own body armor. We do not believe that we will be required to discharge the liability of former senior management personnel for income tax withholding obligations. MBE and WBE firms available to perform the service or provide the supplies or materials. Safariland designs their ballistic panel with comfort and ergonomics in mind. Delaware In Delaware it is prohibited for convicted felons to own body armor. Pompano Beach, wolf grey, Inc. Maryland A convicted felon may not own body armor. This action cannot be undone. Our business will be adversely affected if we are not able to continue to develop new and competitive products. -

November 10, 2005
Vol. 63, No. 45 Published in the interest of the 7th Infantry Division and Fort Carson community Nov. 10, 2005 Visitisit thethe FortFort CarsonCarson WWeb site at www.carson.army.mil 4th ID command visits Iron Brigade Story and photo by Sgt. Zach Mott said. Thurman also highlighted other 3rd Heavy Brigade Combat Team, important keys to a successful deploy- 4th Infantry Division ment: they include properly caring for Major Gen. James D. Thurman, equipment, protecting operational commanding general of the 4th security, maintaining force protection Infantry Division, along with and enforcing discipline, standards Command Sgt. Maj. Ronald T. Riling, and values. 4th ID command sergeant major, vis- Riling added his sentiments to ited the Iron Brigade Monday and Thurman’s. Tuesday. “Good discipline is enforcing the During the two-day visit, the divi- standards,” he said. sion command group met with com- “Good, solid leadership starts at manders, command sergeants major the company level.” and first sergeants to discuss the Riling also discussed the need to readiness of the 3rd Heavy Brigade keep Soldiers — of all ranks — Combat Team as it makes final prepa- informed and ensure that every rations for deploying in support of Soldier, regardless of rank, has a battle Operation Iraqi Freedom. buddy and that they need to check on As Thurman met with the unit com- each other. mand teams, he discussed his “CG’s Thurman and Riling also visited Priorities” with the group. other members of the 3rd HBCT during He emphasized the importance of the two-day visit. the role Soldier’s play in the Global War At each stop the two told Soldiers on Terrorism. -

The World of Teijin Aramid
Teijin Aramid @ Techtextile Middle East Symposium Dubai , 20th Feburary 2014 René Lohmann Sales & Marketing Ballistics Teijin Aramid GmbH, Wuppertal, Germany Agenda • Global Key Trends • Aramids in the middle East • Stopping the bullet • 550dtex f1000 ballistic yarn • LFT SB1 Plus • SRM • Microflex • Twaron and Endumax in helmets • Our research capabilities • Sustainable strength Global Key Trends Global key trends • In recent years, there have been significant changes in the requirements placed on both consumer and industrial goods around the world • There is a growing demand for products that combine high performance with durability and low maintenance • At the same time, these products need to be cost-effective, use less energy, enhance safety, and they should ideally have a smaller lifecycle ecological footprint Sharing our customers’ ambitions • Our prime aim is to add value to the bottom line of our customers • Co-creation and open innovation with customers on advanced products and applications • Loyalty to customers • Long-term relationships • Sharing knowledge & expertise Global presence Aramid in the middle East Our product portfolio Para-aramid • Twaron • Technora Meta-aramid • Teijinconex Poly-ethylene • Endumax Different types to fit application requirements Twaron Technora Short-cut fiber Staple fiber Pulp Fabrics Tape Powder Short-cut fibers Endumax , UHMWPE Tape and X-ply • Ropes, cables and slings • Ballistic protection • Robotics / Force transmission Technora, for enhanced properties • High tensile strength • Weight for -

The Evolution of Plate Armor in Medieval Europe and Its Relation to Contemporary Weapons Development
History, Department of History Theses University of Puget Sound Year 2016 Clad In Steel: The Evolution of Plate Armor in Medieval Europe and its Relation to Contemporary Weapons Development Jason Gill [email protected] This paper is posted at Sound Ideas. http://soundideas.pugetsound.edu/history theses/21 Clad in Steel: The Evolution of Plate Armor in Medieval Europe and its Relation to Contemporary Arms Development Jason Gill History 400 Professor Douglas Sackman 1 When thinking of the Middle Ages, one of the first things that comes to mind for many is the image of the knight clad head to toe in a suit of gleaming steel plate. Indeed, the legendary plate armor worn by knights has become largely inseparable from their image and has inspired many tales throughout the centuries. But this armor was not always worn, and in fact for most of the years during which knights were a dominant force on battlefields plate was a rare sight. And no wonder, for the skill and resources which went into producing such magnificent suits of armor are difficult to comprehend. That said, it is only rarely throughout history that soldiers have gone into battle without any sort of armor, for in the chaotic environment of battle such equipment was often all that stood between a soldier and death. Thus, the history of both armor and weapons is essential to a fuller understanding of the history of war. In light of this importance, it is remarkable how little work has been done on charting the history of soldiers’ equipment in the Middle Ages.