The Impact of the Fragile Health System on the Implementation of Health Policies in Yemen
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

In Yemen, 2012
Updated Food Security Monitoring Survey Yemen Final Report September 2013 Updated Food Security Monitoring Survey (UFSMS), Yemen, Sept. 2013 Foreword Food insecurity and malnutrition are currently among the biggest challenges facing Yemen. Chronic malnutrition in the country is unacceptably high – the second highest rate in the world. Most of Yemen’s governorates are at critical level according to classifications by the World Health Organization. While the ongoing social safety net support provided by the government’s Social Welfare Fund has prevented many poor households from sliding into total destitution, WFP’s continued humanitarian aid operations in collaboration with government and partners have helped more than 5 million severely food insecure people to manage through difficult times in 2012 and 2013. However, their level of vulnerability has remained high, as most of those food insecure people have been forced to purchase food on credit, become more indebted and to use other negative coping strategies - and their economic condition has worsened during the past two years. Currently, about 10.5 million people in Yemen are food insecure, of whom 4.5 million are severely food insecure and over 6 million moderately food insecure. The major causes of the high levels of food insecurity and malnutrition include unemployment, a reduction in remittances, deterioration in economic growth, extreme poverty, high population growth, volatility of prices of food and other essential commodities, increasing cost of living including unaffordable health expenses, and insecurity. While the high level of negative coping strategies being used by food-insecure households continues, the food security outlook does not look better in 2014, as the major causes of current food insecurity are likely to persist in the coming months, and may also be aggravated by various factors such as uncertainties in the political process, declining purchasing power, and continued conflicts and the destruction of vital infrastructure including oil pipelines and electricity power lines. -

Entre La Inestabilidad Y El Colapso, Yemen, El Fracaso Del Proyecto Republicano
MASTER EN RELACIONES INTERNACIONALES Departamento de Derecho Internacional Público y Relaciones Internacionales Facultad de Ciencias Políticas y Sociología UNIVERSIDAD COMPLUTENSE DE MADRID Entre la inestabilidad y el colapso, Yemen, el fracaso del proyecto republicano Moisés García Corrales Trabajo de investigación de final de Máster dirigido por la profesora Paloma González del Miño Yemen, el fracaso del proyecto republicano__________________________________________________ ENTRE LA INESTABILIDAD Y EL COLAPSO: YEMEN, EL FRACASO DEL PROYECTO REPUBLICANO Introducción metodológica Identificación del objeto de investigación Motivación del tema de estudio Delimitación temporal Formulación del tema de estudio Formulación de la hipótesis de partida I. El sistema político y la gobernanza en la República de Yemen 1. INTRODUCCIÓN HISTÓRICA 1.1. La división de Yemen: un país, dos naciones 1.2. La unificación de Yemen: el proyecto republicano 2. LA REALIDAD TRIBAL FRENTE A LA REALIDAD ESTATAL 3. EL PROYECTO REPUBLICANO Y SU DERIVA POLÍTICA 3.1. El constitucionalismo en la República de Yemen 3.1.1. El sistema constitucional y sus reformas 3.1.2. Los derechos y deberes ciudadanos 3.2. El Gobierno y la gobernanza en la República de Yemen 3.2.1. El sistema de partidos 3.2.2. La sucesión presidencial Yemen, el fracaso del proyecto republicano__________________________________________________ 3.2.3. El papel de las Fuerzas Armadas 3.2.4. La descentralización 3.2.5. La lucha contra la corrupción II. El fracaso del proyecto republicano de unificación 4. LOS CONFLICTOS DESEQUILIBRANTES DE LA REPÚBLICA DE YEMEN 4.1. El borde del colapso 4.2. Disidencias y rebeliones internas 4.2.1. Insurgencia huthi en la gobernación de Saada (a) Las causas pendientes del zaydismo (b) Al Qaeda e Irán: la sombra de la duda (c) Desarrollo del conflicto 4.2.2. -
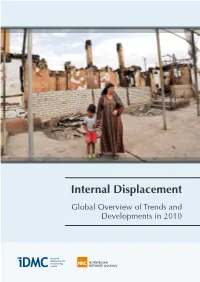
Internal Displacement Global Overview of Trends and Developments in 2010 Internally Displaced People Worldwide December 2010
Internal Displacement Global Overview of Trends and Developments in 2010 Internally displaced people worldwide December 2010 Turkey FYR Macedonia 954,000– Russian Federation Armenia Azerbaijan Uzbekistan Turkmenistan 650 1,201,000 6,500–78,000 At least 8,000 Up to About 3,400 Undetermined 593,000 Serbia Kyrgyzstan About About 75,000 225,000 Georgia Kosovo Up to Afghanistan 18,300 258,000 At least 352,000 Croatia 2,300 Bosnia and Herzegovina 113,400 Cyprus Pakistan Up to 208,000 At least 980,000 Israel Nepal Undetermined About 50,000 Occupied Palestinian Territory At least 160,000 India At least 650,000 Algeria Undetermined Chad Bangladesh 171,000 Undetermined Iraq Senegal 2,800,000 Laos 10,000–40,000 Undetermined Mexico Syria Sri Lanka About 120,000 Liberia At least At least Undetermined 327,000 The Philippines 433,000 At least 15,000 Côte d´Ivoire Lebanon Undetermined At least 76,000 Guatemala Togo Yemen Myanmar Undetermined Undetermined About 250,000 At least 446,000 Eritrea Indonesia Niger About 10,000 About 200,000 Timor-Leste Colombia Undetermined Undetermined 3,600,000–5,200,000 Ethiopia Nigeria About Undetermined CAR 300,000 192,000 Peru Sudan Somalia About 150,000 4,500,000– Republic of About 1,500,000 5,200,000 the Congo Kenya Up to 7,800 About 250,000 DRC Uganda About At least 166,000 1,700,000 Rwanda Undetermined Angola Burundi Undetermined Up to 100,000 Zimbabwe 570,000–1,000,000 Internal Displacement Global Overview of Trends and Developments in 2010 March 2011 Children at the displace- ment camp of Karehe. -
Preparatory Survey Report on the Project for Capacity Building of the Yemeni Coast Guard for Combating Piracy and Terrorism (Building of the Patrol Vessels)
No. REPUBLIC OF YEMEN YEMENI COAST GUARD PREPARATORY SURVEY REPORT ON THE PROJECT FOR CAPACITY BUILDING OF THE YEMENI COAST GUARD FOR COMBATING PIRACY AND TERRORISM (BUILDING OF THE PATROL VESSELS) JANUARY 2011 JAPAN INTERNATIONAL COOPERATION AGENCY JAPAN MARINE SCIENCE INC. EID JR 11-004 REPUBLIC OF YEMEN YEMENI COAST GUARD PREPARATORY SURVEY REPORT ON THE PROJECT FOR CAPACITY BUILDING OF THE YEMENI COAST GUARD FOR COMBATING PIRACY AND TERRORISM (BUILDING OF THE PATROL VESSELS) JANUARY 2011 JAPAN INTERNATIONAL COOPERATION AGENCY JAPAN MARINE SCIENCE INC. PREFACE Japan International Cooperation Agency (JICA) decided to conduct the Preparatory Survey on the Project for Capacity Building of the Yemeni Coast Guard for Combating Piracy and Terrorism (Building of Patrol Vessels) in the Republic of Yemen and sent the survey team from April 12th to May 16th, 2010 to Yemen. The team held discussions with the officials concerned of the Government and conducted a field survey at the study area. As the result of further study in Japan and the discussions regarding the draft of the outline design report which were conducted from October 29th to November 8th, 2010 in Yemen, this present report was finalized. I hope that this report will contribute the promotion of the Project and the enhancement of friendly relations between our two countries. Finally, I wish to express my sincere application to the officials concerned of the Government of the Republic of Yemen for their close cooperation extended to the team. January 2011 Atsufumi KONISHI Director General, Economic Infrastructure Department Japan International Cooperation Agency Summery Summery 1. Outline of Yemen The Republic of Yemen (hereafter referred to as “Yemen”) is located at the southwest end of the Arabian Peninsula, from north latitude of 12 to 19 degrees, east longitude 43 to 54 degrees, neighboring Saudi Arabia to the north, and Oman to the east. -

Charles Schmitz
December, 2011 Scholar Policy Paper Crisis in the Yemeni Economy: a Troubled Transition to Post-Hydrocarbon Growth By: Charles Schmitz — In Memorium — Middle EastMiddle Institute Dedicated to the memory of our friend and colleague Chris Boucek, 1973-2011 Middle East Institute 1761 N Street NW, Washington, DC 20036 202-785-1141 www.mei.edu 1 | Crisis in the Yemeni Economy Charles Schmitz | 2 solution to Yemen’s water scarcity lies in state leadership and capacity, just as the economy requires effective state leadership. INDICA T ORS OF DEVELOPMEN T Obviously this year will not be good one for the Yemeni economy. Prior to the political crisis, growth was forecast to be about 3.4%, but now the economy will shrink substantially. In the heat of the political crisis Ali Abdalla Saleh is accused of betraying the promise of Yemeni unity and there is no doubt that the YEMEN ’S ECONOMIC TRANSI T ION Yemeni economy could have achieved far more had it been better managed, but the reality is that the Yemeni economy has achieved substantial progress over Yemen’s political stalemate is destroying the economy. Violence and labor strife the last twenty years since Unity, not to mention since the establishment of the have shut down oil production, the central bank’s foreign reserves are being Republic forty years ago. In fact, in 2010 the Yemeni economy grew at 8% as a drawn down, and the fighting, demonstrations, electrical outages, and fuel result of the new LNG exports. shortages have paralyzed local businesses to the extent that banks and money exchangers are refusing to buy Yemeni Riyal. -

Mapping of Shoreline Topography Along the Coastline of Yemen
Republic of Yemen TNC-BUR Mapping of Shoreline Topography Along The Coastline of Yemen Final Report Dr.Kadri AbdulBaki Ahmed (head of the team)* Feb. 2018 *Professor of physical geography Aden University EM: [email protected] Contributors • Dr. Gamal Bawazeer (Head of Marine Ecology Center EM: [email protected] • Dr. Fuad Al-Qadasy (Renewed Natural Recourses Center of General Authority of Agriculture Development) EM: [email protected] • AbolGhaith, G. PhD student, GIS&RS Expert EM: [email protected] Project Description Project Title: Third National Communication and First Biennial Update Report Job Title: Mapping of Shoreline Topography Along The Coastline of Yemen Project Number: 00088711 Contracts No.: IC 0043/2017 Duration: 4 Months Starting Date: 09/11/2017 Duty Station: Home based 1 Acknowledgement The authors would like to express their deepest appreciation to all those who provided them the possibility to achieve and complete this report. The authors first gratefully acknowledge the UNDP leaders in Sanaa Yemen, especially those who deserve our greatest gratitude, namely : Hyewon Jung, Team Leader, Economic Resilience and Recovery Unit (ERRU), UNDP CO/YE, Fuad Ali Abdullah, Deputy Team Leader, Economic Resilience and Recovery Unit (ERRU), UNDP CO/YE and Bushra Al-Shirae, Programme Analyst, Economic Resilience and Recovery Unit (ERRU), UNDP CO/YE. The authors would like also to thank Associate Dr. Ameen Ali Mohamed member of geography department, Aden University for his support and encouragement. Eng. Ahmed .R. An Nasiri for his assistance in drawing geologic and land cover maps We also greatly appreciate and thank the team of UNDP in Aden for their security care through project time namely: Mohammed Alsoufi - local Security Associate, Ahmed Al Amodi Admin Assistant and Khulood Sheikh Programme Coordinator. -

Climate Change and Migration: Evidence from the Middle East and North Africa
A WORLD BANK STUDY Public Disclosure Authorized Public Disclosure Authorized Climate Change and Migration Public Disclosure Authorized EVIDENCE FROM THE MIDDLE EAST AND NORTH AFRICA Quentin Wodon, Andrea Liverani, Public Disclosure Authorized George Joseph, and Nathalie Bougnoux Editors Climate Change and Migration A WORLD BANK STUDY Climate Change and Migration Evidence from the Middle East and North Africa Quentin Wodon, Andrea Liverani, George Joseph, and Nathalie Bougnoux, Editors Washington, D.C. © 2014 International Bank for Reconstruction and Development / The World Bank 1818 H Street NW, Washington, DC 20433 Telephone: 202-473-1000; Internet: www.worldbank.org Some rights reserved 1 2 3 4 17 16 15 14 World Bank Studies are published to communicate the results of the Bank’s work to the development community with the least possible delay. The manuscript of this paper therefore has not been prepared in accordance with the procedures appropriate to formally edited texts. This work is a product of the staff of The World Bank with external contributions. The findings, interpretations, and conclusions expressed in this work do not necessarily reflect the views of The World Bank, its Board of Executive Directors, or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. Nothing herein shall constitute or be considered to be a limitation upon or waiver of the privileges and immuni- ties of The World Bank, all of which are specifically reserved. -

Weekly Epidemiological Record Relevé Épidémiologique Hebdomadaire
2013, 88, 81–88 No. 8 Weekly epidemiological record Relevé épidémiologique hebdomadaire 22 FEBRUARY 2013, 88th YEAR / 22 FÉVRIER 2013, 88e ANNÉE No. 8, 2013, 88, 81–88 http://www.who.int/wer Contents Schistosomiasis: number Schistosomiase: nombre de 81 Schistosomiasis: number of people treated in 2011 personnes traitées en 2011 of people treated in 2011 Background Généralités Sommaire The number of countries considered en- L’augmentation du nombre de pays d’endémie demic for schistosomiasis increased from de la schistosomiase, passé de 77 en 2010 à 81 Schistosomiase: nombre de 77 in 2010 to 78 in 2011, reflecting the in- 78 en 2011, est due au fait que le Soudan du personnes traitées en 2011 dependence of South Sudan in 2011. Large- Sud a accédé à l’indépendance en 2011. Le trai- scale treatment for the disease is war- tement de masse contre la maladie n’est assuré ranted in only 52 countries and territo- que dans 52 pays et territoires.1 La transmis- ries.1 It is thought that transmission of sion de la schistosomiase pourrait être faible schistosomiasis may be low in 7 countries, dans 7 pays, mais cela reste à établir; en outre, but this remains to be ascertained, and the l’arrêt de la transmission doit être confirmé interruption of schistosomiasis transmis- dans 19 pays. La maladie demeure un grave sion needs to be verified in 19 countries. problème de santé publique, particulièrement The disease is still a major public health en Afrique.2 Les estimations du nombre de problem, particularly in Africa.2 Estimates personnes nécessitant une chimioprévention of the number of people requiring preven- contre la schistosomiase ont été revues et tive chemotherapy for schistosomiasis communiquées en 2012.3 On considère qu’au were revised and reported in 2012.3 At moins 237 216 451 personnes avaient besoin least 237 216 451 people were estimated to d’un traitement contre la schistosomiase en require treatment for schistosomiasis in 2010. -

The Role of Communications Globalization in Revolutions of the Middle East
Special Issue INTERNATIONAL JOURNAL OF HUMANITIES AND February 2016 CULTURAL STUDIES ISSN 2356-5926 The role of communications globalization in revolutions of the Middle East Nader Mohammadmisa MA in Political Science, Iran [email protected] Hamed Mohagegh Nia Assistant Professor and Faculty Member of Azad University of Ahvaz, Iran [email protected] Abstract Protests in the Middle East and North Africa against dictatorial and hereditary regimes, started in Tunisia in late 2010 and spread to other countries, brought a major change in this area. This uprising began to protest against the lack of free elections and freedom of expression, widespread discrimination in political and economic levels, the accumulation of power and wealth in the hands of the ruling class and its relatives, repression of the opponents and the lack of development and finally resulted in overthrow of the rulers in Tunisia, Libya, Egypt and Yemen. As yet it continues in some countries. Undoubtedly, the speed of these developments in the first few months followed by observers' wonder and there also were those who explored the reasons for the success of popular uprisings in the region and the Islamic world in order to identify hidden aspects of it. The present research is going to explain the role of media and social networks with the aim of trying to explain the role of this factor in the Islamic world developments. Thus, after describing the background of Arab Spring formation and precipitating factors, the position of the media and its importance in the contemporary world and function of the three networks of Facebook, Twitter and YouTube was interpreted. -
1 Introduction
Introduction General framework of the National Anti-Corruption Strategy's Trends Corruption, in its comprehensive concept, is considered to be the main cause behind the failure of development efforts and perpetuation of poverty in any community. In the presence of corruption he state's ability to achieve its development goals related to the welfare of citizens and provision of equality and justice is diminished, as it eats up the bulk of the resources allocated to finance development programs. In light of the major changes experienced by the communities, particularly in the presence of openness the world is witnessing today in term of open borders and the movement of people, ideas, data, information and capitals, opportunities for corruption are growing, and its approaches are strengthened to reach a level at which corruption becomes one of the attributes of communities living in the stage of political and economic transformation. The Republic of Yemen has realized the organic link between anti- corruption efforts and the success of development plans, and had therefore placed anti-corruption efforts at the top of its priorities included in the national agenda for comprehensive reforms, recognizing that the major point to start is in the optimum use of available and limited resources in the overall development and the application of an effective poverty reduction strategy can only be achieved through containment of corruption as well as attempts to drain its origins. In this context, a strong and purposeful will to combat corruption was crystallized for the political leadership, hence a series of national reforms has began in this field, starting with the comprehensive national reform program on March, 1995 which was the cornerstone for launching a series of the national reform in the economic, political, administrative and financial aspects. -
The Battle of the Camel II the Clash of Sects: How Will Sunnis and Shia
The Battle of the Camel II1 The Clash of Sects: How will Sunnis and Shia conflict shape Syria? Presented at FLACSO-ISA Joint Conference, July 24th, 2014, Buenos Aires Nawar Kassomeh Lancaster University [email protected] Tensions between Sunnis and Shia have increased after the Islamic Revolution in Iran and recently these tensions reached a high level of confrontation especially after the American invasion to Iran in 2003. In the last decade, the battle between Sunnis and Shia has taken place in Iraq, Lebanon, and Syria. Many signs support this assumption including the sectarian civil war in Iraq, the two attempts to destroy Hezbollah in 2006 and in 2008, the current Syrian civil war, and other incidents including the clashes between Saudi forces and Hothis (2009–2010) in Yemen,2 as well as the Saudi military intervention in Bahrain in March 2011 to back its Sunni rulers.3 In the Middle East, it is impossible to separate politics from religion. The current conflict in Syria is another episode of the long religious conflict and animosity within the Muslim World between Sunnis and Shia (Crittenden, 2012). The sectarian conflict became more obvious in the last decade and more intense specifically after the U.S. invasion to Iraq in 2003. The rivalry between Muslim sects and principally between Sunnis and Shia determines the nature of the conflict in Syria and in the Middle East. This sectarian war had started right after the American Invasion to Iraq and later reached the Syrian territories in what can be called the second “Battle of Camel.” Iraq has been governed by Sunnis under Saddam 1 The title refers to the Battle of the Camel in the year 656 between supporters of Ali (the Fourth caliph) and supporters of Aisha the Prophet’s wife. -

Yemen Market Study
Table of Contents Table of Contents .................................................................................................................................... 2 Executive Summary ................................................................................................................................. 3 Background and Objectives .................................................................................................................... 6 Methodology and Sampling Framework ................................................................................................. 7 Household Food Security and Markets in Yemen ................................................................................... 8 Market Functioning and Determinants of National-Level Food Availability in Yemen ........................ 14 Yemen, International Markets and the Macro-economy ................................................................. 17 Domestic Yemeni Markets .................................................................................................................... 25 Structure and Conduct ...................................................................................................................... 25 Market Integration and Food Flows ..................................................................................................... 31 Household Food Access: Purchase conditions for households ............................................................. 34 Evolution and Behaviour of Prices ...................................................................................................